Key words
Smoking prevention, social influence, health education intervention, secondary education students
Introduction
Greece occupies a leading position in tobacco consumption per capita in the world. In the rest of Europe, mortality due to smoking is gradually decreasing while in Greece there is a trend of constant increase. [1] Fifty two per cent of Greek men and 32% of Greek women smoke although, in the last few years, the number of male smokers has decreased while that of female smokers has increased. [2]
Smoking habits significantly increase with age among the adolescent Greek population. Thus, while at the age of 11 only 5.2% of boys and 2.4% of girls refer having smoked, at the age of 14, 3 out of 10 teenagers have smoked; this ratio becomes 1 out of 2 at the age of 15 – 16 years. [3,4]
Inception of smoking coincides with the onset of adolescence, while it is also directly correlated with initial psychological impulses that are determined and strengthened by the social environment and are continued with the pharmacological activity of nicotine on the sympathetic and parasympathetic systems and the smoker's addiction at a later age. [5] The need to be identified and accepted by peers is gradually developed during adolescence. Peers have an increasing influence on smoking attitudes and habits. The fear of rejection, the desire to be recognised by peers, as well as the need of adolescents to feel members of a group, lead to social experimentation with smoking. [6] School has also a key role in children's lives, so naturally it influences their smoking habits to a great extent. Existence of relevant stipulations and regulations, their implementation, as well as the smoking habits and attitude of teachers and the rest of the school staff are decisive to students' attitude. [7] Most anti-smoking programmes developed and implemented by researchers at schools, are based on the assumption that if students knew that smoking is harmful they would choose not to smoke. Although programmes based on learning about the consequences of smoking are not necessarily ineffective if they are properly implemented, most researchers consider them incomplete.
Health education programmes dealing with social influences ae based on the work of McGuire. [8] This approach showed encouraging results. [9,10] Social influence is a generic term defining multiple psychological influences exercised by people on an individual. Social psychologists have noted that there are two types of pressure a group can exercise on its members. [11] First the group might require its members to act in accordance with its rules so that they can get or still be accepted by the rest of the group members, so it adopts a normative social influence. Then the group might require its members to share similar attitudes with regards to social meanings and the frequency of the different behaviours, so it adopts an informational social influence. The purpose of a normative social influence programme is to eliminate the pressure exercised on the individual by the group so as to be accepted through smoking, while the purpose of an informational social influence programme is to eliminate the pressure for the adoption of favourable attitudes and principles towards smoking. [12]
Until now, a few studies have been carried out in Greek schools on smoking prevention. The most recent one was published by Koumi and Tsiantis [13] and showed that the intervention implemented by peers can delay the onset of smoking in junior high school students.
Methodology
The objective of this study were to implement a health education programme – including an internet application - for the prevention of smoking based on the social influences model and evaluate the programme effectiveness.
Study design
The study was designed as semi-experimental with control group.
Study sample
The intervention was performed in 88 students of Vocational Schools during the two-hour class of Health Education of the standard programme. The control group consisted of 118 students from three different schools.
The main criterion for the inclusion of these schools was their very good computer infrastructure that was necessary for the educational intervention through a web page. All school directors and teachers were informed on the duration and content of the Health Education intervention, so as to obtain their consent and collaboration. Although the intervention was implemented during the standard programme students were informed that they could decline to participate in the programme either individually or as a class group. The health education intervention was performed from October 2005 to November 2006.
Content of the intervention
The Health Education intervention was implemented in each school class separately. Its duration was two hours once a week for 10 weeks at fixed hours. The Health Education Programme included interactive methods, so as to encourage student participation and to facilitate integration of the material. Methods included Workgroups using printed material and activities sheets, Discussion, Demonstration, Homework, Role play, Games and the use of the Interactive web application. Table 1 shows the content of the lessons, which was based on the Towards No Tobacco (TNT) programme following appropriate permission by the authors. [12]

Questionnaire for the evaluation of the intervention
The questionnaire for the evaluation of the intervention was based on existing questionnaires found in the Greek and international literature and were: a) the anti-smoking attitude and self-esteem scales used by Koumi & Tsiantis [13]; b) the questionnaire developed by Sussman et al. [12] within the framework of the TNT programme for the prevention of smoking at schools; and demographic data. The questionnaire prepared by Sussman et al. [12] was translated by the researcher and then the Greek translation was discussed with health education specialists and high school teachers, so as to ensure the accuracy of the translation, as well as its suitability for students of that age. Next, a different person performed the back translation and the two questionnaires were compared. Authorizations and relevant licenses for all questionnaires were obtained from the authors.
The following variables that are related to the evolution of an adolescent student's smoking behaviour were included in the questionnaire.
• Student's demographic characteristics such as sex, age, place of residence, parents' educational level, parents' profession, living with others, as well as whether they had previously attended other Health Education Programmes.
• Student's smoking behaviour. Two questions regarding history of experimenting and current frequency of smoking, e.g. "My father/mother smokes every day….does not smoke – 4-point scale.
• Intent to smoke in the future, 6 items, e.g. "I might smoke at school", answered on a 5-item scale "very likely to very unlikely".
• Knowledge on health problems and the dependence caused by smoking, including 41 items related to normative social influence, informational social influence and the consequences of smoking on health. Questions are multiple choice or True/False. Questions corresponded to the health education programme content.
• Anti-smoking attitude (17 items) e.g. smoking is a waste of money answered on a 5-point scale from "totally agree" to "totally disagree".
• Rosenberg's self-esteem scale (10 items) that was previously used with samples of Greek adolescent students (e.g. "Overall, I am satisfied with myself": on a 4-point scale from "I agree" to "I disagree").
All scales were analyzed as to their internal consistency by Cronbach’s alpha. The result for the knowledge questionnaire was α=0.83, the self-esteem scale α=0.75, the attitude scale α=0.61 and the intent scale α=0.88.
One week prior to the commencement of the intervention, the questionnaire for evaluating its effectiveness was completed by the participating students. One week after the last lesson, students in all classes were asked to complete again the same questionnaire. During the same period that is immediately after the intervention, the same questionnaire was completed by the control group. Finally, during the third phase, students who participated in the intervention were called to fill in again the same questionnaire, five months after their summer holiday, so as to assess the level of maintenance of knowledge and skills acquired during the programme of smoking prevention. The Health Education Programme was implemented exclusively by the researcher.
Statistical analysis
For the statistical analysis of the data the SPSS 13.00 was used. Since study data did not follow the normal distribution, non-parametric tests were used (chi-square test, Μann-Whitney U test, Kruskal-Wallis and Wilcoxon analyses) for the assessment of the intervention in the control and intervention groups.
Results
Demographic characteristics
In the intervention group, 70(80%) were female and 18(20%) male. Mean age in the intervention group was of 18.77 (SD=4.99) years. In the control group 86(73%) were women and 32(27%) men with mean age 17.38 (SD=3.14) years. In terms of the educational level of the father and mother, 35% and 38% respectively had finished high school in the intervention group, while in the control group were 39% and 42%, respectively. Concerning place of birth, 53% in the intervention group came from Athens while 25% came from Albania. Likewise, 61% in the control group came from Athens while 28% came from Albania. No statistically significant differences were found in the demographic data between the intervention and control groups.
Descriptive results concerning knowledge on smoking
The answer to the 1st question of the knowledge scale which is not included in the calculation of the total knowledge score shows what students believe to be the reason to start smoking. Results showed that 58% of the students during the second measurement for the intervention group and 50% in the control group believed that most people smoke because they see others do so and this gives them a good social image.
Figure 1 shows the evolution of the summary indicator of knowledge, while Figure 2 illustrates the individual indicators in the intervention group and Figure 3 the comparison between intervention and control groups. Statistically significant differences were observed in all groups except for comparison on informational social influence between knowledge at six months after the health education and the knowledge at baseline.

Figure 1: Change in the total knowledge score in all three measurements in the intervention group.
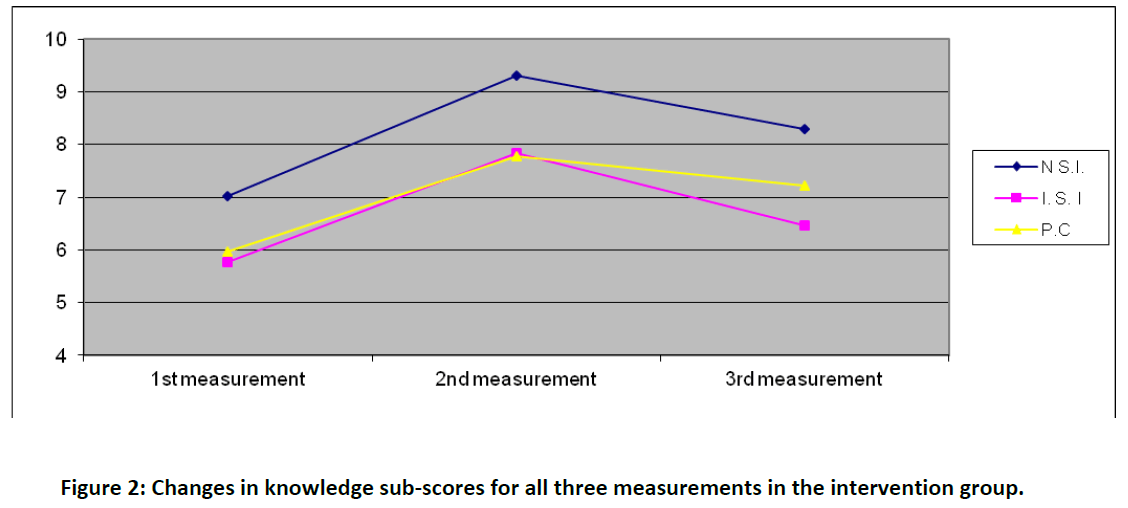
Figure 2: Changes in knowledge sub-scores for all three measurements in the intervention group.

Figure 3: Average values in knowledge score and sub-scores in the intervention and control groups immediately after the intervention.
A statistically significant difference between the total knowledge score after the Health Education programme in the intervention group and that of the control group was found (U=3461, p<0.001). Statistically significant differences were also observed in the knowledge sub-scores (normative influence, informational influence and consequences of smoking) after the health education in the intervention group as compared to the control, group (U=3560 p=0.000U=4119 p=0.015, U=4030, p=0.008, respectively).
Correlations of total knowledge score after health education and demographic data showed a statistically significant difference with the mother’s educational level and staying with parents/others (chi-square=7.54, p= 0.023 and U=1120.5 p=0.025).
Students' anti-smoking attitude
It was found that 89% agreed that smoking is a waste of money; 60% and 65% respectively agreed that smoking should be prohibited in public places and in advertising; while 68% agreed that it is difficult to quit smoking. Moreover, 72% disagreed that smoking forms part of growing up, 70% that it helps you make friends, 75% that it makes others like you more, 71% that it is fun and 62% that peers who smoke look older. Comparison with the control group showed that percentages of agreement on the attitudes in terms of prohibiting smoking in advertising and public places, social image of smoking as well as the financial aspect of smoking are similar.
Smoking behaviour
Smoking behaviour and, more specifically, of whether they have tried even one or two puffs (trial), current frequency of smoking, currently smoking or not, even if occasionally, and number of cigarettes/day are shown for all three measurements in the intervention group and the control group, in Table 2.
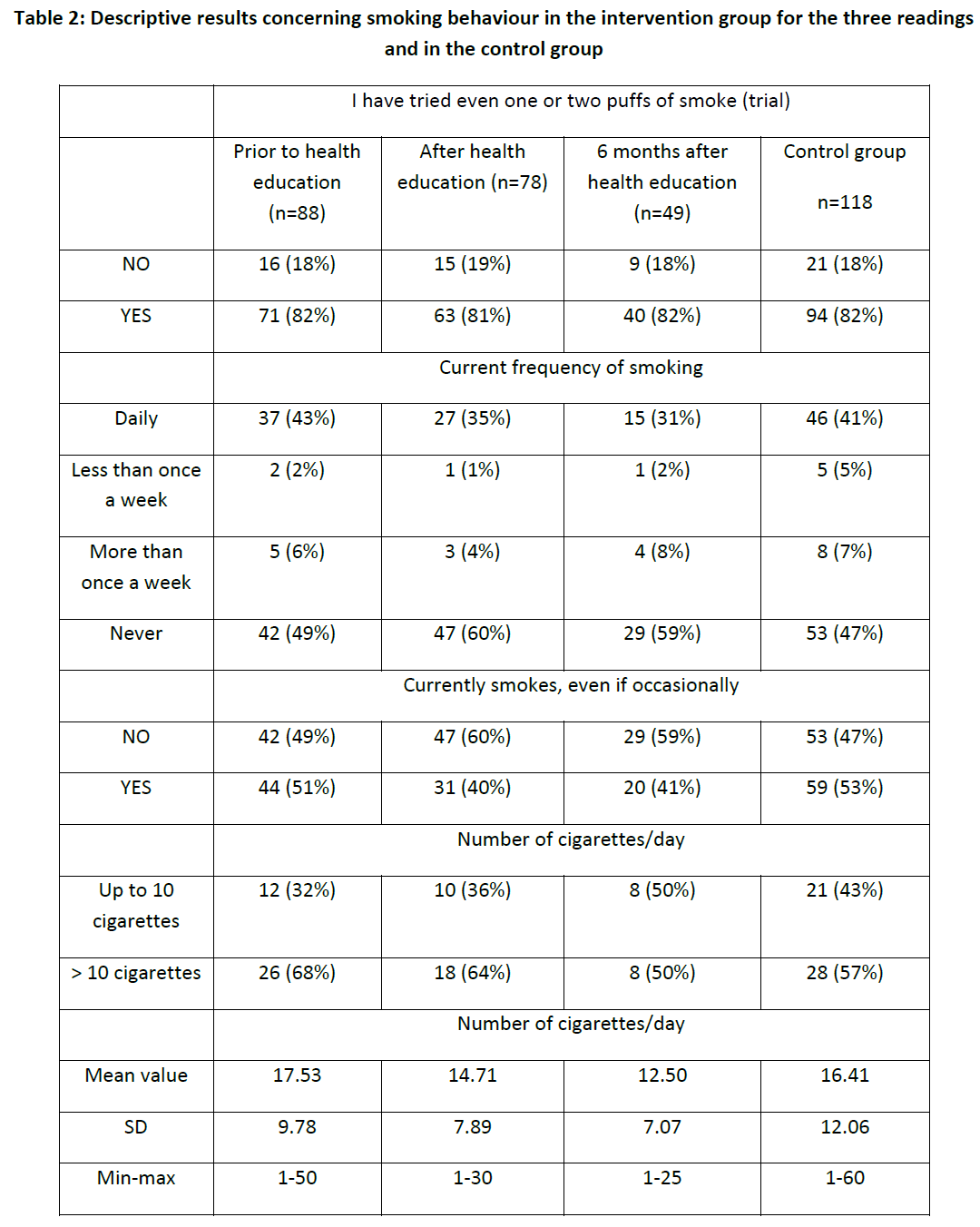
The chi-square test performed for all three measurements in the intervention group for the variables "has tried even one or two puffs", "currently smoking, even occasionally" and "number of cigarettes/day" did not show any statistically significant differences. The Wilcoxon paired test performed for the comparison of number of cigarettes in all three measurements showed a statistically significant difference only for the comparison prior to and after the Health Education (p=0.029).
Comparison between the second measurement in the intervention and the control group for the variables "has tried even one or two puffs", "currently smoking, even occasionally" and "number of cigarettes/day" did not show any statistically significant differences. Similarly, comparison of the number of cigarettes between the second measurement in the intervention and the control group did not show any statistically significant difference (U=663, p=0.806).
Finally, correlation of the number of cigarettes with demographic data revealed a statistically significant difference between age (adults and minors) and trial of even one puff and occasional smoking (chi-square=11.702 p=0.01 and chi-square =8.716 p=0.03 respectively).
Evaluation of self-esteem
Wilcoxon test among the three measurements in the intervention group of the self-esteem score showed a statistically significant difference in the first two measurements (p=0.006 and p=0.021 respectively), while there was no difference in the third measurement. The change in the self-esteem score of the intervention group for the three measurements is illustrated in Figure 4. Comparing the self-esteem score after the Health Education with that in the control group, no statistically significant difference was found (U=4611, p=0.706). The mean value of the total self-esteem score after the health education was statistically higher for those who did not want to attend the health education in the future as compared to those who did (U=2910.5, p= 0.008).
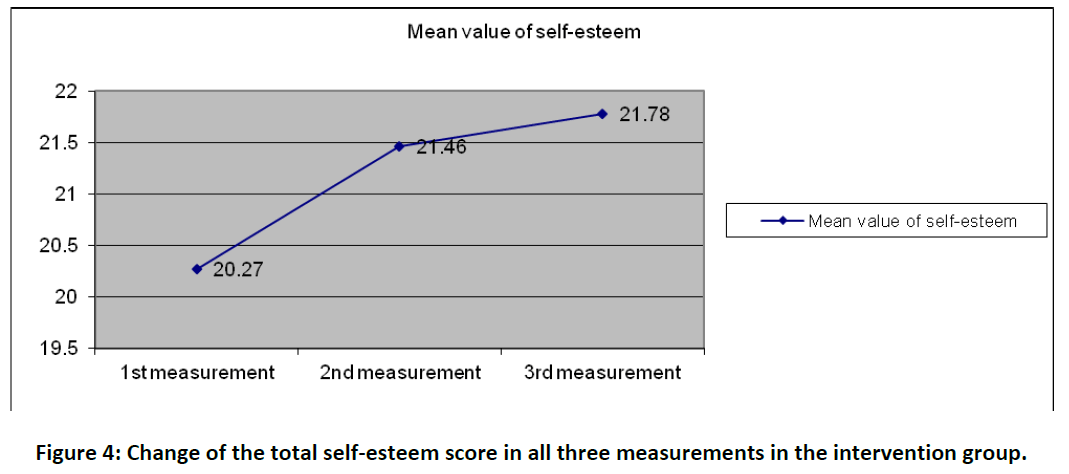
Figure 4: Change of the total self-esteem score in all three measurements in the intervention group.
Intent to smoke
Figure 5 shows that the most probable reason to start smoking in the future is the existence of problems, in a proportion of 18% and 32% for the intervention and the control groups, respectively.
Chi-square test did not show statistically significant difference (p=0.962) among those who stated that it was quite/very likely to smoke in all three measurements in the intervention group. Similarly, no statistically significant difference (p=0.453) was observed between those who stated that it was quite/very likely to smoke in the intervention group (second measurement) and the control group.

Figure 5: Possible reasons for initiating smoking
Correlation of the question about the likelihood to become a smoker with demographic data, smoking behaviour and the number of other important persons who smoke, showed that students more likely to smoke in the future are those who were already smoking, even occasionally, those who have tried even one or two puffs and those whose important people (parents, siblings, friends) were smokers.
Discussion
Although there were no statistically significant differences in demographical data between the intervention group and the control group, results cannot be extrapolated to all secondary education students as the study sample was neither representative nor random of the population under study. However, these findings are useful for the planning and evaluation of similar programmes in the future.
In terms of the first item of the knowledge scale, showing what students believe to be the reason to start smoking, the majority thinks that most people smoke because they see others doing so and this gives them a good social image. This finding suggests the need to raise awareness in the society for the complete prohibition of cigarette advertising. In countries that have adopted similar measures, a reduction was observed in the number of students stating to be smokers. [13]
With regard to knowledge, an increase was observed right after the intervention, which however decreased 6 months later, although it was still higher compared to prior knowledge in the intervention group. The knowledge score after the intervention was also higher that the control group. A similar increase was observed in the knowledge subscores related to the normative and informational social influence as well as in the consequences of smoking, and in comparison with the control group. These results lead to the conclusion that the short-term objective of increasing knowledge in the experimental group in relation to the control group was achieved. The higher knowledge score of students in normative social influence is consistent with Sussman’s study [14] showing that students assimilate better this kind of knowledge as opposed to other categories. In other words, schools and especially junior high schools should introduce Health Education as a mandatory assignment, while emphasis should be given to teaching tobacco refusal skills; also, smoking prevention programmes should not be limited to the consequences on the human body.
As for the attitude, it seems that in matters concerning advertising, the financial aspect of smoking, social image and maturity, there was no change in the intervention group following the intervention. It should be also noted that a similar study [13] carried out in junior high schools in Greece showed that among students who were already smoking, the increase of the anti-smoking attitude in the experimental group was not maintained until the next measurement.
Concerning smoking behaviour, the findings of the present study are consistent with other studies in the Greek population indicating that at the age of 17-18 years, the vast majority of adolescents have already smoked, while 43.5% smoke on a daily basis [4], while the prevalence of smoking in Greek students aged 16-19 years reaches 50%. [15] Frequency of smoking did not seem to be influenced by the intervention, although, the number of cigarettes was reduced after the intervention, returning to the same levels as prior to the intervention, six months later. Even though differences among the three measurements in the intervention group and between the second measurement in the intervention group and the control group were not statistically significant, there was a reduction in the percentage of students who declared smoking on a daily basis, occasionally, as well as in the average number of cigarettes as compared to the control group. These findings show a partial success as to the long-term objective of the programme that is to reduce daily use of cigarettes; the loss of students from the initial sample should also be taken into account. It would be useful to continue evaluating the programme for a longer period in the intervention and control groups so as to examine whether the change in behaviour is permanent or transient, as this was not possible within the limited timeline of the present study. It should also be taken into consideration that the students' smoking behaviour does not depend only on school based interventions. Smoking habits of the students' environment (parents, siblings, and friends) influence to a great extent the adoption or not of the anti-smoking behaviour. It would be useful therefore, to perform Health Education interventions for smoking prevention through the media and within the social environment the Greek student lives and acts.
In terms of self-esteem, in the intervention group there was an increment in the measurement after the Health Education in relation to the first one. Moreover, self-esteem remained high in the third measurement six months after the first one. Self-esteem is considered an important parameter in smoking prevention programmes. In interventions against smoking lead by peers performed in Greece [13] there was an assumption of an indirect increase of self-esteem in the target group through its participation in activities for the production of audiovisual materials and posters. This assumption was confirmed during the evaluation of the intervention. In the future, it would be interesting to carry out a study to examine whether a more rigorous self-esteem boosting intervention would influence alone the smoking behaviour.
Regarding intent to smoke in the future, no significant difference was revealed among those who stated it was quite/very likely to smoke and in the three measurements of the intervention group; also, no change was observed in the second measurement in the intervention group with the control group. It should be noted that the intent to smoke in the future was higher for those students who were already smoking, even occasionally, and for those whose important other people (parents, siblings, and friends) were smoking. So, it was observed that it is not easy to change intent in a sample of students, 41% of which smoke on a daily basis. A relevant study [16] on the psychosocial factors associated with the willingness of the non-smoking students to smoke in the future, showed that their intent is decreased as their attitude of not using smoke products becomes more positive, if they have friends who do not smoke and if they consider that it will be harder to quit smoking later. These findings should be considered by those responsible for the primary prevention of smoking who should constantly remind students of nicotine's highly addictive properties, as well as the pressure from their peers.
The weaknesses of the programme include the older age of the students, which means that many of them were already smoking, so a smoking cessation programme would be more suitable for them. In the future it would be interesting to repeat a similar study with a larger sample of students of a younger age, since as it was observed in this study, the age of onset of smoking is between 14 and 16 years of age.
In conclusion, implementation of this programme increased knowledge overall but also on the three individual scores in the intervention group regarding normative social influence, informational social influence and consequences of smoking, with the first being superior to the rest. Moreover, a transient decrease in the number of cigarettes and an increase in self-esteem were observed.
The adoption of a mandatory health education course against smoking seems to be necessary in junior high schools, while it is also necessary to have specialised and continuously trained professionals teaching it. These courses should be also repeated in high schools, and their success or failure should be verified.
3066
References
- Household survey 2004/2005 Cost and cigarette consumption. www.statistics.gr. Retrieved in 4/7/2007[Greek].
- Currie C, Hurrelmann K., Settertobulte W, Smith R and Todd J. Young people’s Health in Context: International Report from the HBSC 2001/2002 Survey. WHO Policy Series: Health Policy for Children and Adolescents, issue 4, WHO Regional Office for Europe, Copenhagen, 2004.
- Hibbel B, Anderson B, Bjarnason T, Ahlstrom S, Balakireva O, Kokkevi A, Morgan M. The ESPAD Report 2003- Alcohol and Other Drug Use among Students in 35 European Countries. The Swedish Council for Alcohol and Other Drugs (CAN).The Pompidou Group at the Council of Europe, 2004.
- Pontifakis G. Learn about smoking. Ignorance kills. Αthens: Parizianos 1988 [Greek]
- Hellenic Association of Tobacco Processing Industries. Cigarette Consumption, Greek Market Athens, 2003; 18(12): 30-31[Greek].
- McGuire J. The nature of attitude and attitude change. In G. Lindzay & E. Aronson (Eds), Handbook of social psychology. 2th edition, Vol.3. Reading, MA: Addison –Wesley, 1969, pp. 136-314.
- Flay R. Psychosocial approaches to smoking prevention: A review of findings. Health Psychology, 1985; 4: 449-488.
- Tobler S. Meta-analysis of 143 adolescent drug prevention programs: Quantitative outcomes results of program participants compared to a control or comparison group. Journal of Drug Issues, 1986; 16: 535-567.
- Sussman S, Dent C, Burton D, Stacy A, Flay B. Developing school-based tobacco use prevention and cessation programs. Sage Publications, 1995.
- Koumi Ι, Τsiantis J. Smoking trends in adolescence: report on a Greek school-based, peer led intervention aimed at prevention. Health Promotion International, 2001; 16: 65-72.
- Sussman S, Dent C, Stacy A, Hodgson C, Burton D, Flay B. Project towards No Tobacco Use: Implementation, process and post-test Knowledge evaluation. Health Education Research, 1993; 8: 109-123.
- Vardavas C, Kafatos A. Smoking policy and prevalence in Greece: an overview. European Journal of Public Health, 2007; 17: 211-213.
- Smith B, Bean M, Mitchell K, Speizer I, Fries E. Psychosocial factors associated with non-smoking adolescents intention to smoke. Health Education Research, 2007; 22: 238-247.

