Key words
Decision support system, iodine diet ontology, ontology, personalized healthcare, SWRL
Introduction
In medical science, decision making is a complex task as it depends on variety of interrelated functions. [1] We are concentrating not only on the accuracy and prediction of the result, but also on the interoperability of the result from the physicians who use Decision Support System (DSS). Making the right decision at right time is the most important factor in healthcare systems, especially in medical diagnosis systems. [2]
The phenomenal growth of technological development in healthcare systems, forces the knowledge corresponding to the diagnosis and adaptation of treatment flow to be recorded by a variety of methods such as Clinical pathways, DSS, Guideline based DSS and so on. [3] The decision support system is one of the methods widely used in healthcare systems.
Classification plays a vital role in decision making. Decision trees are among the classification techniques that solve large complex problems by providing rules in an understandable form. [4] But the rules generated from decision trees do not work well with continuous attributes. Fuzzy logic system supports uncertain boundaries. [5] The main difficulty arises with a slight change in attribute values, which in turn changes the sensitivity of decision tree. Crisp set comprises a function with 0(false) and 1(true), whereas fuzzy set theory contains the elements with unsharp boundaries, that is, it handles uncertain information. [6] In order to handle the aforementioned issues, it is necessary to move to fuzzy decision trees.
Personalized treatment is an important factor in healthcare systems. The term personalization refers to the delivery of right diagnosis and treatment for every individual patient. [7] Traditional healthcare decision support systems do not provide reasoning and mainly focused on integration of data and knowledge. In order to improve knowledge representation and reasoning facility, the ontologies acts as a stepping stone to improve the healthcare systems.
Ontology is a combined approach of artificial intelligence and machine learning with sharing and reusability of knowledge. [8] A framework for healthcare systems was to be presented in this paper. The system includes a fuzzy rule generation and diagnosis environment, it handles the generation of rules using Fuzzy Decision Tree algorithm (FS-DT). The rules generated by fuzzy decision tree pave the way for proper decision making with respect to current status of the patient such as age and results of the clinical tests. Based on the diagnosis message, the system infers the SWRL rules that provide the treatment flow. The clinical area selected as a target area for implementing the CDSS is thyroid gland and obesity management.
In this paper the food composition database is used for finding how much iodine, carbohydrate, protein and fat presents in each and every food item. The database is constructed by Health Finland. [9] The iodine, carbohydrate, protein and fat level of each food item was collected and analyzed completely to construct the Food Composition Ontology (FCO). The use of proposed food composition ontology for iodine maintenance and obesity management would make the illustration of the framework clearer.
The rest of the paper is organized as follows, Section 2 devoted to the related work performed in the area of healthcare systems. Section 3 deals with the proposed architecture of healthcare systems. Section 4 provides the system performance evaluation results. Finally Section 5 is summation of findings along with suggestions for further research in this area.
Related work
Since a well-defined data model is important for the execution of treatment flow and for the success of semantic web technologies in healthcare systems, the ontology is used to construct the decision support systems. [10] The term ontology is taken from philosophy and it is the knowledge of formal explicit specification with a sharing facility of aggregation. [11] Ontology is constructed to define properties, attributes and restrictions corresponding to the concepts. Each and every entity can be called a class. An attribute of ontology refers to a characteristic of concept or relationships between concepts. An instance of ontology implies a case of concept.
The SWRL is one of the standard rule languages of semantic web, which contributes to the ability to write Horn-like rules with respect to Web Ontology Language (OWL) concepts. [12] SWRL rules make three-fold use of the vocabulary of ontology syntactically, semantically and inferentially. SWRL is a combination of RuleML and OWL ontology and at present it is one of the specifications of W3C. [13] The rules are used to derive new knowledge from OWL knowledge bases by using inference engine. The Java Expert System Shell (JESS) is a forward chaining inference engine developed under Java language at Sandia National Laboratories, New Mexico. JESS uses the very efficient Rete algorithm to match the SWRL rules. [14] It is also compatible with protégé through JESS-Tab plug-in. [15]
Papageorgiou [16] presents a framework, based on Fuzzy Cognitive Map (FCM) and fuzzy rule extraction techniques. This framework is a combined approach of fuzzy logic and neural networks, which make the system knowledgeable. But the inadequate information available and total dependence on the knowledge extraction techniques are the noticeable flaws in the systems which have to be satisfied.
Lee et al., [17] provide the fuzzy ontology that produces the Intelligent Diet Recommendation Agent (IDRA) for diabetic patients. It prescribes the required dinner allowance based on his/her metabolic rate. But the system provides diet for diabetic persons only. A balanced diet is one of the significant factors for humans. But in this system there is no inference mechanisms used for the dynamic updating of the ontology.
Proposed system
This work makes a sincere attempt to present, a personalized framework for healthcare application for decision making. Through the diagnosis process with the use of fuzzy decision tree algorithm, the diagnosis message is received. Based on the diagnostic message received, the SWRL rules are executed to produce the treatment flow. The framework consists of three environments such as Fuzzy rule generation and Diagnosis, Rule execution and Ontology construction. The framework of the proposed system is presented in figure 1. The three environments are described in detail.
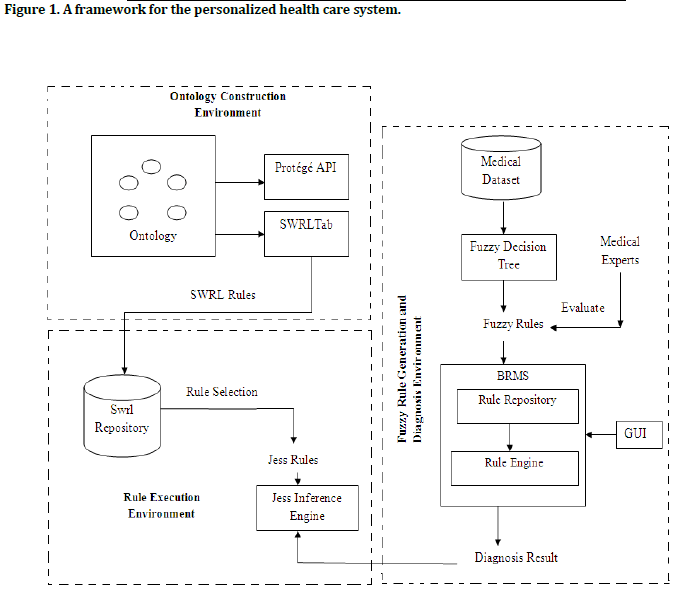
Figure 1: A framework for the personalized health care system.
Fuzzy rule generation and diagnosis environment
This environment deals with the generation of rules obtained from a medical dataset using fuzzy decision tree techniques. This study uses Fuzzy Supervised Learning In Quest (SLIQ) based Decision Tree (FS-DT) algorithm. [18] FS-DT algorithm is an extension of SLIQ decision tree algorithm with added facility of fuzzification.
The SLIQ based FS-DT algorithm works well on quantitative data as it has fuzzy boundaries instead of crisp boundaries. The size of the fuzzy decision tree is reduced while using FS-DT algorithm. The fuzzy boundaries and reduced size of the tree make its application in healthcare decision making process easy and useful. FS-DT uses Gini index as a splitting measure. [19] The membership function of the FS-DT algorithm produces the degree of fuzziness among the attribute values. The rules are derived from fuzzy decision tree. [20] Each path from the root node to leaf node represents a specific rule, for example R1, R2 upto Ri are derived from fuzzy decision tree. The Ri represents the fuzzy concept, that defines the conditions derived from the path from the root node to leaf node. In general, there are a large number of data pairs and the rules are generated using each pair, which naturally results in the emergence of few conflicting rules. In order to solve these problems, the rules are pruned using a post pruning algorithm. [21] The system provides nearly 30 rules for diagnosis. Medical experts are involved in analyzing the data pairs to find which pairs are useful and which are unlikely to occur and identify the rules that emerge due to measurement errors.
Every new derived rule is evaluated by the medical expert. Each attribute from a rule is represented in a fuzzy set as low, medium and high. The generated rules from fuzzy decision tree are stored into rule repository, which is constructed with the use of Business Rule Management System (BRMS). We use openrules BRMS [22] as a tool to construct the rule repository and the rule engine. During execution the rule engine collects all matched rules with respect to patient’s current status. The matched rules are executed by a rule engine and it produces a diagnosis result.
Rule execution environment
The main task of the rule execution component is to construct the SWRL rules and the rules are executed by JESS inference engine. The SWRL rules are selected with respect to a patient’s diagnosis message. The diagnosis message triggers the system and the matched SWRL rules with respect to diagnosis message are selected for execution. The JESS inference engine executes the matched SWRL rules, which provide the appropriate treatment flow. JESS inference engine produces the results in xml format, which is further utilized for the adaptation of results into hospital. The inferred knowledge returns by JESS is updated into the ontology as new instances.
Ontology construction environment
Ontology represented in OWL format is used to construct a knowledge base. [23] OWL may be divided into three sub languages i) Owl Full ii) Owl DL iii) Owl Lite. The three categories are formed on the basis of expressiveness. The proposed study uses the Owl DL to construct the food composition ontology. First with the assistance of a dietician, we collect and analyze the concepts and attributes with respect to the nutrition values of various food items. Three classes described in meta- ontology are represented as food categories, diagnosis result and patient profile information. For example food categories include six groups of sub classes: Grains and Starches, Fruits and Juices, Vegetables, Pulses, Fat or Oils and Meats. The diagnosis result class possesses nine concepts: the first three concepts for thyroid gland (hyperthyroid, hypothyroid and normal) and the remaining six concepts for obesity management (under nutrition, healthy weight, overweight, obesity- class I, obesity- class II and obesity- class III). Patient information class includes the details about patient’s clinical and personal information. Figure 2 presents the partial design of Food Composition Ontology (FCO) for thyroid gland management in which the diagnosis-message class possesses three individuals: hyperthyroid, hypothyroid, and normal. Figure 3 shows the part of the developed ontology for obesity management by using protégé-Jambalaya plug-in. [24]
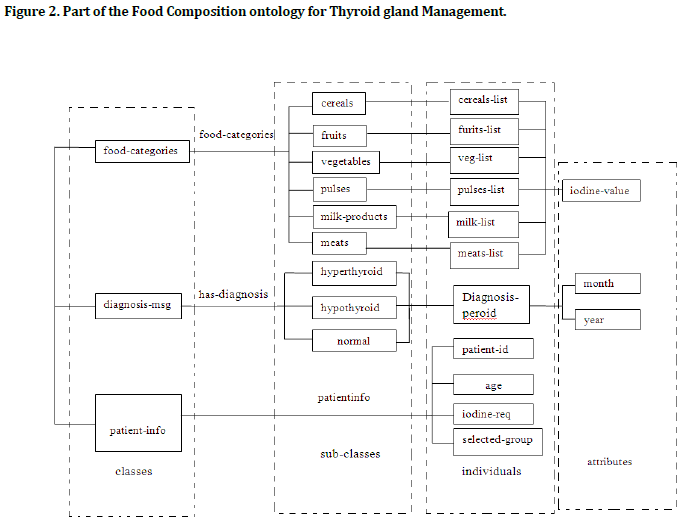
Figure 2: Part of the Food Composition ontology for Thyroid gland Management.
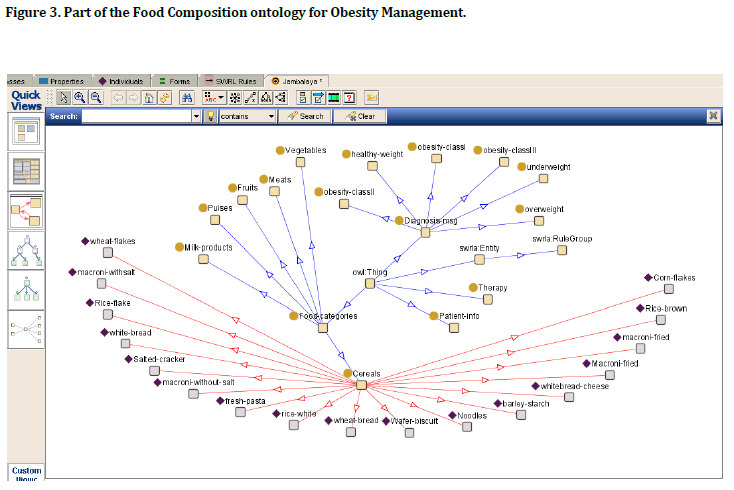
Figure 3: Part of the Food Composition ontology for Obesity Management.
Case 1: Thyroid gland
For normal thyroid function and for the production of thyroid hormones iodine is necessary. Balancing iodine is a complex task because insufficient iodine causes enlargement of the thyroid, spastic weakness, paralysis and mental retardation. Iodine is a very harmful mineral, because taking more than enough iodine can cause enlarged thyroid gland, thyroid cancer, burning of the mouth, and stomach. The thyroid dataset is taken from UCI machine learning repository. [25] The system provides nearly 30 rules for thyroid gland diagnosis. The matched rules are executed by a rule engine, which produces a diagnosis result such as hyperthyroidism, hypothyroidism and normal. Some example rules are presented below for hypothyroidism,
If (TSH) is high AND Total T4 is low then hypothyroidism
If Free T4 is low then hypothyroidism
If Total T3 is low then hypothyroidism
TSH : Thyroid Stimulating Hormone Test, Total T4 :
Total Thyroxine Test, Free T4 : Free Thyroxine
Test, Total T3 : Total Triiodothyronine Test.
The requirement of iodine differs from person to person. World Health Organization (WHO) recommends the following formula [26] for the easy and perfect calculation of requirement of iodine for each individual is represented below,
For age 0–12 months iodine requirement = 7.5 μg/kg/day. Kg stands for weight in Kilogram.
For age 1–10 years iodine requirement = 5.4 μg/kg/day.
For adolescents and adults iodine requirement = 2 μg/kg/day.
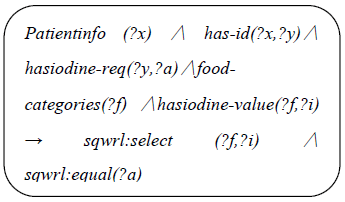
Collection and analysis of the entities and attributes corresponding to the diet for iodine maintenance is done with the help of a dietician, which ultimately leads to the construction of more than 25 SWRL rules for iodine maintenance. Some example SWRL rules related to iodine maintenance are presented below.
Rule 1: Rule 1 prescribes the food items related to his/her iodine requirement. The Rule 1 returns the food items with iodine value related to iodine requirement of patient.
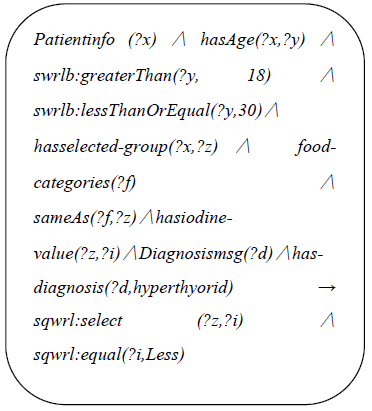
Rule 2: If patient is between 18 and 30 years and the diagnosis message is hyperthyroidism then the rule 2 returns the food items selected by the patient which have less iodine.
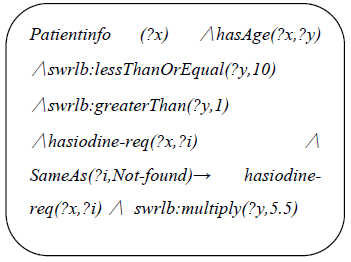
Rule 3: The Rule 3 calculates the patient’s iodine requirement. If patient is between 1 and 10 years of age and the iodine requirement according to ontology is nil, it can be calculated by multiplying the age of the person by 5.5. The inferred value (iodine requirement) is updated into OWL.
Case 2: Obesity management
Obesity is defined as an excessive amount of fat on a body. The main factors which cause obesity are changes in diet and reduced physical activity. [27] Increased urbanization, environmental changes are also the causes of obesity. BMI is the general measure to diagnose obese. Increased BMI can cause many problems such as Type 2 diabetes, heart diseases and some cancers like breast, endometrial cancer. [28] Managing overweight and obese is a main challenge to the world because even in the same country there is mal-nutrition as well as obese [29] , which necessitates computerized obesity management systems. The drastic changes in the food habits in the last few years are the root-cause of wide spread physical defects and deformities. Healthcare organizations try to increase the awareness of diet but still it is not sufficient and people eat readymade foods, which have high fat and low nutrition. [30] Some of the generated rules for obesity diagnosis are as follows,
If BMI is low AND WC is low AND Gender= Male then Underweight.
If BMI is medium AND WC is low && Gender= Male then Healthy weight.
If BMI is very high AND WC is high AND Gender= Male then obesity class III.
BMI: Body Mass Index and WC: Wrist Circumference.
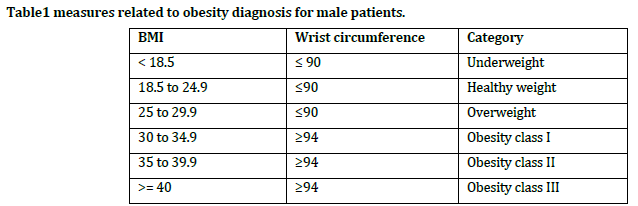
In general BMI is to be calculated as BMI = kg / meters2. That is weight in kilogram which is divided by height2 in meters. The measures related to obesity diagnosis for male patients, recommended by WHO are presented in Table 1.
-
Female patients with a high wrist circumference that is, ≥80 will have increased risk of obesity. The calorie requirement for each patient is calculated by Harris-Benedict Equation. [31] In general, 20 % -- 30% of fat is needed in total calorie requirement. The diagnosis result class possesses six concepts: under nutrition, healthy weight, overweight, obesity- class I, obesity- class II and obesity- class III. Some of the SWRL rules are given below for obesity management.
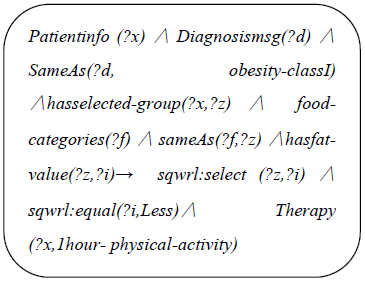
Rule 4: If diagnosis message is obesity class I, then the rule 4 prescribes the food items, with less fat value with respect to his/her selected food category. The rule also infers into Therapy as one hour physical activity like walking, jagging and so on.
Rule 5: If diagnosis message is obesity class III, then the rule 5 prescribes the selected fat-free food items. The rule also infers into Therapy of Undergo-surgery.
Results and Discussion
An extensive experimental evaluation to decide the efficiency of the system by comparing the IDRA with the proposed System is conducted. This framework is implemented using Java 1.6.0, Protégé 3.4.7, NetBeans IDE 7.0.1 in Pentium® Dual-Core 3.00 GHz with 1.93 GB RAM, running Windows XP.
Figure 4 represents the quality of the ontology in terms of Relationship Richness (RR), Attribute Richness (AR), Class Richness (CR) and Cohesion (Coh). [32] For a better understanding the aforementioned three values are converted into percentage. The Type 2 Fuzzy Ontology (T2FO) is based on the IDRA system and the FCO, which is analyzed in this paper.
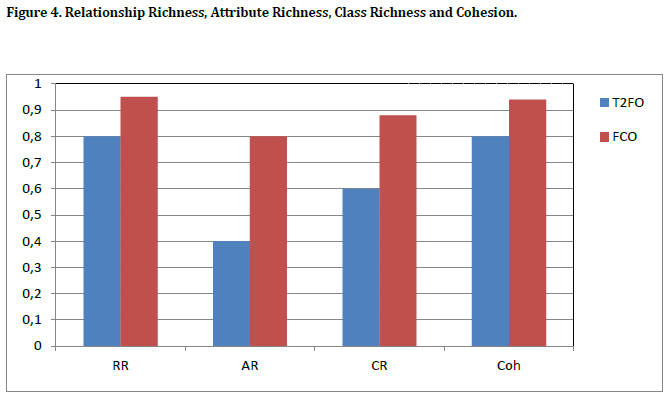
Figure 4: Relationship Richness, Attribute Richness, Class Richness and Cohesion.
Relationship Richness (RR): The variations of relationship presented in ontology are represented by the RR metric. Which plays a key role in indicating, how the ontology is potentially useful. If RR value is 1, the ontology gives more types of relationship including class-subclass relationships. The proposed FCO ontology returns RR as 0.95 and therefore most of the relationships are used.
Attribute Richness (AR): Use of more number of attributes (slots) enriches knowledge. The average number of attributes per class in the ontology is represented by the metric AR. If the AR value return is high then each class has a number of attributes at the average. When an AR value return is low, then the ontology provide less information for each class.
Class Richness (CR): The CR metric is used to determine the amount of knowledge gained by the ontology. It is evaluated by calculating the number of instances corresponding to a class in the ontology. If the CR value return is high then the data represent most of the knowledge in ontology schemas. The proposed FCO ontology defines more knowledge when compared to the existing T2FO ontology.
Cohesion (Coh) : Traditionally, cohesion defines the degree to which the elements in a module are connected. In ontology cohesion defines the degree of how the OWL classes are semantically related to each other through their properties. If ontology is considered as a graph then the node represents instances and the edge represents relationships. It is calculated through number of connected, individual components in the instances of the ontology. If a more semantic association is present in ontology and the Knowledge Base (KB) is fully connected, it returns the cohesion value is 1 or nearly one. The proposed FCO ontology returns 1 therefore the entities (elements) are strongly related. Therefore it is concluded that the proposed FCO ontology for iodine maintenance ensures good performance of RR, AR and CR and Coh.
The figure 5 shows the satisfaction degree about the diet recommendation of IDRA and the proposed FCO. Satisfaction degree is measured by three domain experts (DE) i.e., the domain experts evaluate the recommendations about iodine maintenance provided by the system and then give a feedback of the system. The satisfaction degree branches into very dissatisfied (0%--30%), dissatisfied (30%--60%), satisfied (60%--80%) and very satisfied (80%--100%). This figure shows that the user satisfaction level of FCO is effective when compared to IDRA.
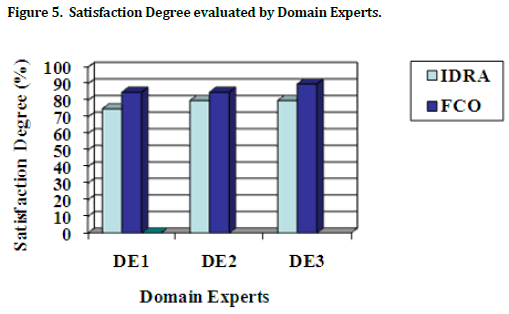
Figure 5: Satisfaction Degree evaluated by Domain Experts.
Figure 6 presents the accuracy of two algorithms Fuzzy ID3 and FS-DT for a thyroid dataset. The accuracy could be measured by the ratio of true positive and true negative in the dataset which makes it crystal clear that the FS-DT algorithm produces greater accuracy than a Fuzzy ID3 algorithm. Computer based healthcare applications increase day by day. There are still some areas where the healthcare system can be made the most efficient and reliable with the help of emerging computer technologies.
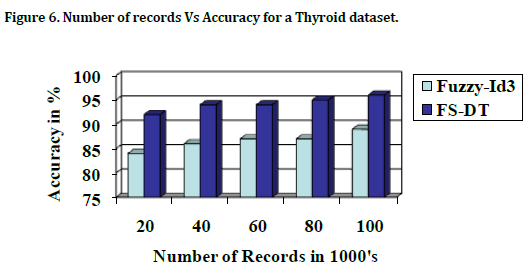
Figure 6: Number of records Vs Accuracy for a Thyroid dataset.
The main objective of this research is to design the framework, implementation and evaluation of the performance of the framework for treatment personalization. The implemented architecture ensures good performance with respect to accuracy and satisfaction degree. The proposed framework has the ability to automatically trigger the rules and also it offers the treatment recommendations. The practical difficulty of a patient in frequently meeting a dietician, to learn of his/her daily quota of iodine and of the food items with required quantity of iodine and fat is the motivational force behind the development of this system.
In the proposed framework is used the knowledge acquired from medical experts for the construction of SWRL rules. Whereas most of the healthcare decision support systems focus either on diagnosis or on treatment adaptation. The proposed framework deals with both diagnosis and treatment adaptation.
Conclusion
This framework first diagnoses the malady based on which recommendation for the diet is prescribed. As the constructed framework is fully automated via semantic web technologies, it ensures personalized treatment with less intervention from domain experts and the framework may be disease-independent.
Besides arriving at an acceptable decision, this framework paves the way for minimal use of time. The fuzzy rule-based techniques are employed to generate the rules, which in turn are executed by rule engine that provides a diagnosis. The protégé is used to construct the food composition ontology to keep the thyroid gland and obesity management. Then SWRL is used to build the association rules. Based on the diagnosis, the SWRL rules are executed by inference engine, which in turn produces proper food items related to patient’s requirement. Every time the system reasons over the rules and the OWL receives the feedback from the collected knowledge.
2736
References
- Dhar V and Stein R. Intelligent decision support methods: The science of knowledge work. 4th Edition. Upper Saddle River, NJ, Prentice-hall ,1997.
- Rung-Ching Chen and Cho-Tsan bau. Development of anti-diabetic drugs Ontology for Guideline based Clinical drugs recommend System using Owl and SWRL, In: James Bezdek, Bor-Sen Chen (Editors). Fuzzy Systems [FUZZ] IEEE International Conference on Communication, Networking & Broadcasting , Computing & Processing ;18-23 July 2010, Barcelona. Spain.
- Abbasi MM , Kashiyarndi S: Clinical Decision Support Systems: A discussion on different methodologies used in Health Care [Internet] ; 2010 [cited:2012 August 23] .Available from:https://www.idt.mdh.se/kurser/ct3340/ht10/FinalPapers/15-abbasi_kashiyarndi.pdf
- López-Vallverdú JA, Riano D , Bohada J. Improving medical decision trees by combining relevant health-care criteria, Expert Systems with Applications 2012; 39(14): 11782–11791.
- Khosravi, R. Hossein. FCM-fuzzy rule base: A new rule extraction mechanism. In: Eyad H Abed and Wyatt Hume (Editors). IEEE International Conference on Innovations in Information Technology (IIT); 25-27 April 2011, Abu Dhabi: IEEE Computer Society.
- Levashenko, Vitaly G. Fuzzy Decision Trees in medical decision Making Support System. In: Denisiuk, Aleksander (Editors), Federated
- Conference on Computer Science and Information Systems (FedCSIS), IEEE; 9-12 September. 2012, Wroclaw, Poland, IEEE Computer Society .
- Alexandrou D, Skitsas I, Mentzas G. A Holistic Environment for the Design and Execution Self-Adaptive Clinical Pathways, IEEE Trans on Information Technology in Biomedicine 2011; 15(1): 108-118. doi : 10.1109/TITB.2010.2074205.
- Noy NF and Mcguinness DL: Ontology development 101: A guide to creating your first ontology, Stanford University, Stanford, 2001, Available from: https://protege.stanford.edu/publications/ontology_development/ontology101.pdf.
- Fineli ® - Finnish Food Composition Database [Internet] . Finland: National Institute for Health and Welfare;2003 [updated 2013, December 9;cited 2013 January 12] . Available from: https://www.fineli.fi/index.php?lang=en.
- Hu Z, Li JS, Zhou TS, Yu HY, Suzuki M, Araki K. Ontology-based clinical pathways with semantic rules.J Med Syst 2012 ;36(4):2203-12.
- Kaushal Giri. Role of Ontology in Semantic Web, DESIDOC Journal of Library and Information Technology (DJLIT) 2011; 31(2): 116-120.
- Muthuraman Thangaraj and Sankaran Gnanambal. A new architectural framework for rule based healthcare system using semantic web technologies, Internation Journal of Computers in Healthcare. Inderscience. Forthcoming March 2014.
- Bamidis. P, Kehagias. D.D, Kaimakamis. E, Maglaveras. N. Dynamic Composition of Semantic Pathways for Medical Computational Problem Solving by Means of Semantic Rules, IEEE Transactions on Information Technology in Biomedicine, 2011; 15(2):334-343.
- Ernest Friedman-Hill. Jess the Rule Engine for the JavaTM Platform, Sandia National Laboratories, California: Sandia Corporation, 2008 [cited 2012 June 10] Available from: https://herzberg.ca.sandia.gov/
- Henrik Eriksson.Using JessTab to integrate protégé and jess, Intelligent information processing, IEEE 2003;18(2):43-50.
- Papageorgiou Elpiniki I. A new methodology for decisions in medical informatics using fuzzy cognitive maps based on fuzzy rule-extraction techniques, Applied soft computing journal, Elsevier, 2010; 12(12): 3798-3809.
- Chang-Shing Lee, Mei-Hui Wang and Hani Hagras. A Fuzzy Expert System for Diabetes Decision Support Applications, IEEE Transactions On Fuzzy Systems; 2011; 41(1) : 139-153.
- Chandra B and Paul Varghese P. Fuzzy SLIQ decision tree algorithm. IEEE transactions on systems, man and cybernetics 2008; 38(5): 1294 - 1301
- Kantardzic, M. Data Mining: Concepts, Models, Methods, and Algorithms. Second edition; Wiley-IEEE Press.2011.
- Myung Won Kim, Joong Geun Lee, Changwoo Min. Efficient fuzzy rule generation based on fuzzy decision tree for data mining, Fuzzy Systems Conference Proceedings, 1999. FUZZ-IEEE '99. 1999 IEEE International Computers Society, 22-25 Aug. 1999, Seoul, South Korea, vol(3), 1223 – 1228.
- Xiaodong L,Xinghua F,Witold P. Extraction of fuzzy rules from fuzzy decision trees: An axiomatic fuzzy sets (AFS) approach. Data & Knowledge Engineering 2013; 84:1-25.
- OpenRules BRMS [Internet] :OpenRules Inc.2009 May 12 [cited July 2012] .Available from:https://www. openrules.com/
- Welty C and Jenkins J. An ontology for subject. International journal of knowledge and data engineering 1999; 31(2):155-182.
- Jambalaya [Internet] :Standford: Stanford University; 2004 [Updated 2008 June 27; cited 2012 July 21] . Available from: https://protegewiki.stanford.edu/wiki/Jambalaya_2.6.0
- Arthur Asuncion and David Newman, Rexa.info. UCI Machine Learning Repository [cited 2012 June 21] Available from: https://archive.ics.uci.edu/ml/datasets/Thyroid+Disease
- FAO/WHO Human vitamin and mineral requirements. Bangkok, Thailand: world health organization food and agriculture organization of the united nations Rome , Report of a Joint FAO/WHO Expert Consultation, Rome, 2002; 181-194. Report no.:2809e00.
- Walker CG, Zariwala MG, Holness MJ, Sugden MC. Diet, obesity and diabetes: a current update.Clin Sci (Lond) 2007;112(2):93-111.
- White House Task Force on Childhood Obesity Report to the President , Solving the Problem of Childhood Obesity within a Generation, Executive Office of the president of United States, 2010.
- Misra A, Chowbey P, Makkar BM, Vikram NK, Wasir JS, Chadha D, et al. Consensus statement for diagnosis of obesity, abdominal obesity and the metabolic syndrome for Asian Indians and recommendations for physical activity, medical and surgical management.J Assoc Physicians India 2009;57:163-70.
- Maya Sappelli. An adaptive recipe recommendation system for people with Diabetes type 2, Master's Thesis in Artificial Intelligence, Radboud University Nijmegen,2011.
- Frankenfield, DC, Muth ER ,Rowe WA. The Harris-Benedict studies of Human basal metabolism history and Limitations. Journal of American Dietetic Association 1998; 98 (4): 439-445.
- Samir Tartir, I Budak Arpinar, Michael Moore, Amit P Sheth, Boanerges Aleman-Meza. OntoQA: Metric-Based Ontology QualityAnalysis, 2006 [cited 2012 June 12] Available from: https://lsdis.cs.uga.edu/library/download/OntoQA.pdf.

