Keywords
Circle of willis; Anatomical variants; Absence; Hipoplasia; Duplication; Fenestration
Background
The circle of Willis (CW) was originally defined by the English anatomist Thomas Willis who first described it completely and correctly in 1664, in his paper entitled Cerebrianatome: cui accessitnervorumdescriptioetusus [1], as an arterial anastomotic structure that exhibits complete symmetry in shape and its configuration [2].
Much later, in the literature appeared more and more articles reporting various variations from the original definition. Many authors reported, especially in the last two decades, a percentage higher than 50% of all PAWs they have analyzed as having significant asymmetries and variations [3-5].
Because CW provides the best collateral source of blood flow in arterial occlusive disorders, identifying anatomical variants that could be present at this level is especially essential in planning surgery for cerebral aneurysms [6].
Also, several studies have shown these anatomical variations of the CW play an important role in the development of cerebrovascular diseases (ischemic and hemorrhagic strokes) and even in psychiatric disorders [7-9].
The frequency of these anatomical variations of CW has not yet been sufficiently evaluated in the Romanian population, and in the North-Eastern region of the country there is no such research.
Given the fact that the hospital where this research was conducted is a regional health unit, where there are admitted patients with neurological and neurosurgical diseases living in the North-Eastern region of Romania, the purpose of our study was to identify the morphological features of the constituent vessels of fresh circles of Willis at the moment of the autopsy of the deceased patients in the Emergency Clinical Hospital „Prof. dr. N. Oblu” Ia?i, noting the presence or absence, variations of shape, position or trajectory of each arterial segment. In the end, our results were compared with those from literature in order to identify some particular pattern of this anastomotic structure in the population of the North-Eastern region of Romania.
Materials and Methods
Study design
The present research is a descriptive in-hospital observational study by assuming the principles of institutional ethics.
Selected population
The population included in this study consisted of 96 patients who died of various medical causes in the Emergency Clinical Hospital “Prof. dr. N. Oblu” Ia?i, in a period of 30 months (01.01.2014-30.06.2016), to whom an anatomo-clinical autopsy was performed in order to determine the cause of death. The sex and the age of the deceased were registered from the Register of necropsies of the Department of Pathology within the hospital.
Selection of the samples and measurements of the constituent arteries of the circle of willis
All the circles of Willis identified during the time of autopsy were studied, whether or not they had anatomical abnormalities.
The artery diameters of all the circles of Willis from this study were measured with a ruler on fresh specimens. The arteries examined were: anterior communicating artery (AComA), proximal segment (A1) of anterior cerebral arteries (ACAs), internal carotid arteries (ICAs), posterior communicating arteries (PComAs), and proximal segment (P1) of posterior cerebral arteries (PCAs).
Macroscopic examination of the willis polygon
The presence of any kind of anatomical variations of its constituent vessels was noted.
The following anatomical features were analyzed:
• If the arterial circle is complete or incomplete,
• If there were some of anatomical variants of its vessels: hypoplasia, absence, duplication, fenestration, difference in length and difference in origin and place of discharge, compared to opposite segments.
The ”hypoplasia” of an artery of the circle of Willis was defined as having an outer diameter of less than 1 mm, except for the communicating arteries, which were considered to be hypoplastic with an outer diameter of less than 0,5 mm [10].
We defined the posterior cerebral artery as ”fetal” (fACP) when it originates from the internal carotid artery, and maintains a small atresic connection with the basilar artery [11].
Photographing available specimens
The the circles of Willis used in the study were numbered and photographed with a Sony digital camera.
The statistical analysis
The results were collected in a database using Excel and then tabulated. The data obtained were used to calculate the mean, number and percentage, as well as to make the corresponding graphs.
Results
Identification of the study sample
Out of the total of 96 available human brains, 68 cases (70.83%) presented the classic shape of the circle of Willis, respectively it was complete and symmetrical. The remaining 28 cases (29.17%) were classified as ”atypical” as they expressed anatomical variants of the constituent vessels (Figure 1).
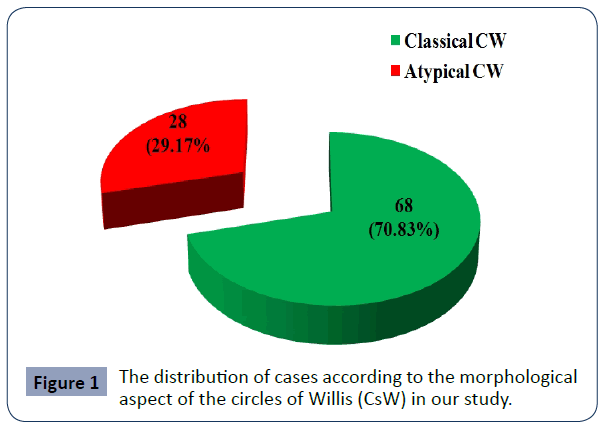
Figure 1 The distribution of cases according to the morphological aspect of the circles of Willis (CsW) in our study.
Demographic data of deceased patients with anatomical variants of circle of willis
Of the 28 deceased patients with atypical CW, 15 (53.57%) were male and 13 (46.42%) female, so that M: F ratio was 1.15 in the favour of male gender.
The average age of the entire group was 61.78 years. Female cases ranged in age from 39 to 86 years, with a mean age of 60.15 years, and male cases ranged in age from 40 to 85 years, with a mean age of 65.6 years.
Types of anatomical variants identified in circles of willis in our study
In the present study, out of the 28 circles of Willis we have analyzed, 19 (67.86%) presented multiple anatomical variants, and only 9 cases (32.14%) had a single anatomical variant (Table 1).
| Number of associated anatomical variants |
Number and percentage of CW with anatomical variants |
| one |
9 (32,14%) |
| two |
9 (32,14%) |
| three |
7 (25%) |
| four |
2 (7,14%) |
| five |
1 (3, 57%) |
Table 1 Type, number and percentage of anatomical variants of circles of Willis in our study.
Among multiple variants of the vessels of the circle of Willis, we identified the association of two (32.14%), three (25%), four (7.14%), or five (3,57%) anatomical variants of those seven constituent arteries (Table 1).
Eight types of variations of the constituent arteries of the circle of Willis were identified in the 28 cases we have analyzed (Figure 2), namely: absence of a vessel, partial fetal ACP, hypoplasia, duplication, fenestration, azygos, common trunk with another vessel at the origin, longer length with sinuous trajectory.
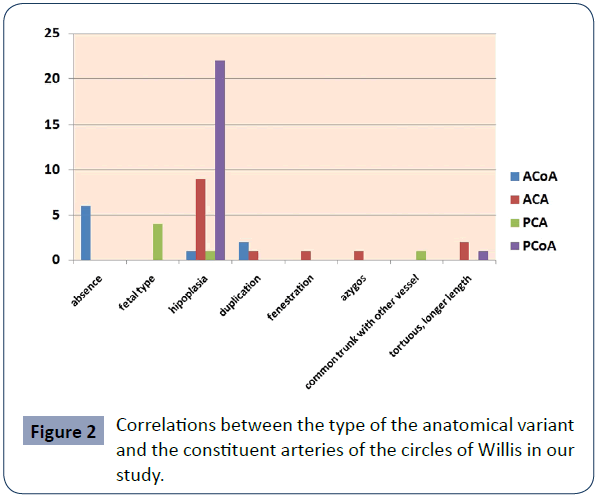
Figure 2 Correlations between the type of the anatomical variant and the constituent arteries of the circles of Willis in our study.
The most common morphological features was hypoplasia of a vessel (Figure 3), which was identified in almost any constituent vessel of CW, i.e. ACoP (22 cases, 78.57%), followed by ACA (9 cases, 32.14%); ACoA and AcoP were hypoplastic in only 2 (7.14%) cases each. Duplication was identified only in the case of ACoA (2 cases, 7.14%) and at the level of ACA (1 case, 3.57%). The longer length with sinuous trajectory was identified at the level of ACA and ACoP (one case (3.57%) for each vessel). Absence was identified only at the ACoA level (6 cases, 21.42%) (Figure 4), partial fetal artery was identified only at the ACP level (2 cases, 7.14%), fenestration and azygos artery only at the ACA level (1 case, 3.57%), and a common trunk with another vessel at the origin origin was identified in a single case (3.57%) in which the ACP originated in a common trunk with the superior cerebellar artery.
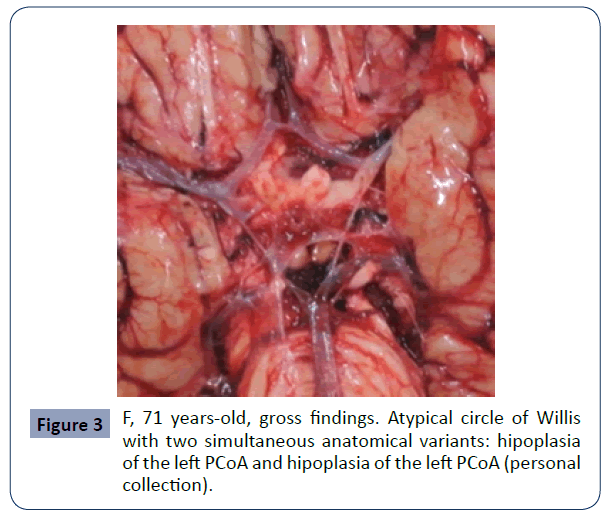
Figure 3 F, 71 years-old, gross findings. Atypical circle of Willis with two simultaneous anatomical variants: hipoplasia of the left PCoA and hipoplasia of the left PCoA (personal collection).
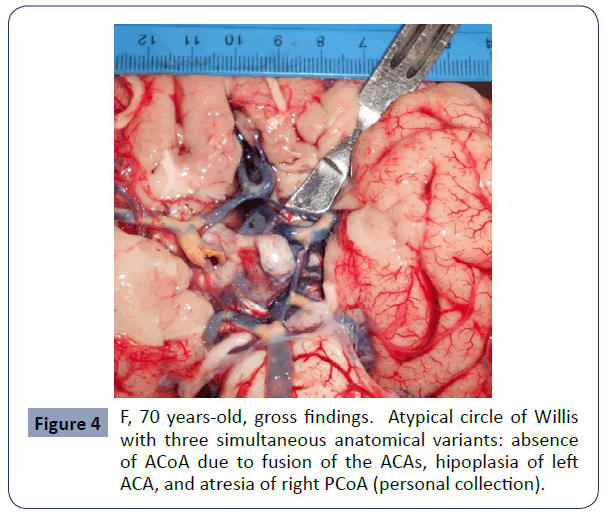
Figure 4 F, 70 years-old, gross findings. Atypical circle of Willis with three simultaneous anatomical variants: absence of ACoA due to fusion of the ACAs, hipoplasia of left ACA, and atresia of right PCoA (personal collection).
Discussions
The circle of Willis (CW) plays an important role in cerebral hemodynamics because its presence as an intact anastomotic canal facilitates much more efficient blood flow compared to situations in which it is deficient. But in the literature, even among normal individuals, a CW with a classical appearance, as described by Thomas Willis [1], seems to represent only a percentage with a wide variation, depending on the country, the method of study or the number of analyzed cases.
There are a relatively large number of studies that have analyzed the morphological appearance of CW by computed tomography (CT) or magnetic resonance imaging (MRI) angiograms. Siddiqi et al [12] in Lahore, Pakistan, performed a CT-angiographic study on 54 unselected patients with hemorrhagic stroke and found only 13% of them having a complete and symmetrical CW, the remaining cases (87%) presenting different anatomical variants. Similar percentages were obtained by Klimek-Piotrowska et al [4], from Poland, who also analyzed 250 patients by CT- angiography. In their study, 16.80% of the analyzed CsW had the classic appearance; the remaining 83.20% had different morphological variations. Cristea et al [13], in Romania, in an CT angiographic study combined with MRI angiograms, found even fewer CsW with a normal, classic appearance (only 8% of 50 patients they have investigated).
However, there are also angiographic studies that have identified only a few CsW with anatomical variations. In Sudan, Alawad et al [14] analyzed 143 patients by MRI angiography and found anatomical variations of the arteries of CsW in only 28% of cases. Also, Harizi (Shemsi) et al [15], in Albania, analyzed by CT angiograms 60 patients with stroke and 60 healthy subjects and identified in almost one-fifth of the cases for each group the presence of anatomical variants of CW, although the percentage was higher, of course, in the group of patients with strokes (23.3% vs. 16.7%, respectively). In Italy, Macchi et al. [16] obtained only a slightly higher percentage for cases with anatomical variations of CW.
The studies analyzing CsW obtained at autopsy, either anatomical-clinical or forensic, showed much more diverse anatomical variations. Poudel and Bhattarai [17], in Nepal, analyzed 35 formalized brains, obtained by anatomo-clinical autopsy, and reported the presence of classic CW in a very high percentage (91.4%), the remaining 8.6% showing various anatomical abnormalities. In West Bengal, India, a group of researchers analyzed 75 formalin fixed brain specimens and identified classical type of CW in 73.33% of cases. PCoA presented the highest number of anatomical variants (22%), being followed by ACoA that presented anatomical variations in 13.3% of cases, such as duplication, more common, hipoplasia and absence. In 9.3% of all circles of Willis these authors analyzed, ACA presented hipoplasia, plexiform pattern, or fusion with the contralateral ACA, and PCA presented anatomical variants in only 5.3% [18].
At the opposite pole there is a study realized by De Silva et al [5] in Sri Lanka, who reported the presence of classic PAWs in only 14.2% of the cases when they analyzed 225 formalized brains obtained at forensic autopsies. Prasad et al [19] from a teaching Hospital in Nepal, realized a CT angiographic study on 65 patients. A normal or classical circle of Willis was identified in only 35.4%, the most common variant of circle of Willis being the hipoplasticPCoA seen in more than a quarter of cases. However, these authors concluded that anatomical variation are more frequently encounter, at least on CT angiograms, in the posterior part of the circle of Willis because they identified not only a hipoplasic or absent PCoA, but also fetal origin of PCA in 13.8% of cases, but a hipoplasic or absent ACoA only in 12.3% of cases.
However, there are also studies that have identified almost similar values between classical CW and CW with various anatomical variations [10, 20-22].
Our study, performed on 28 fresh brains obtained at the anatomoclinical autopsy, identified a 2.5 times higher number of classical CsW compared to CsW that showed anatomical variations (70.83% vs. 29.17%), representing intermediate values among those reported in various studies performed on CsW obtained at autopsies. However, these values are close to those reported in the MRI-angiographic study conducted by Alawad et al [14] in Sudan (72%) and the CT angiographic study performed by Harizi (Shemsi) et al [15] in Albania (76.7%).
Some studies have shown a prevalence of anatomical variations of CW in male patients. Arjun and Chandan [23] analyzed the anatomical variants of CW in a population from the Southern region of India in which men accounted for 66% of the 300 participants. These authors found that a complete configuration of CW is slightly more common in women than in men. In our study, a male predominance was identified among our cases with CsW obtained at autopsy and presenting anatomical variants.
In Brazil, Suemoto et al [24] analyzed anatomical variations of arteries of CsW obtained at autopsy from 221 deceased patients and also found out a slight predominance of male gender.
Jin et al [25] analyzed the characteristics of CW in a population of 281 subjects in a region of China with a family history of stroke using CT angiography. The age of the patients varied between 24- 77 years, with an average age of 50.9 ± 10.5 years. Among those patients, the number of women were smaller (F: B = 0.83), but the authors did not find an age difference between the two sexes.
There are not many articles in the literature reporting association of multiple anatomical variations of the constituent arteries of the CW. Raghavendra et al [22], in India, found only unique and unilateral anatomical variations in their series. Also in India, in a study realized by Kapoor et al [20] on 1,000 brains taken during forensic autopsies, a percentage of only 7.4% of the analysed CsW had multiple morphological variations.
In Italy, of the 100 CsW of healthy subjects investigated by MRI angiography, Macchi et al [16] found multiple associations of anatomical variants in only 16% of cases. In 3% of cases, they identified the association between the absence of ACoA and the hypoplasia of the left ACoP (45), a configuration that we also have identified in our study in one case, representing 3.57% of all CsW we have studied, but in our study an ipsilateral ACA fenestration was added. Macchi et al [16] also reported in 2% of cases the absence of an ACoP associated with the origin of an ACP in the internal carotid artery (fetal ACP). In another 2% of cases, ACAs were partially fused, and in another 2% of cases hypoplasia of both ACAs and the two PCAs were identified. The remaining seven cases (7%), all different from each other, represented other combinations of the variants described above [16].
In a study similar to ours, Sinha et al [26] analyzed 80 fresh brains obtained at the forensic autopsy at the Department of Forensic Medicine in Calcutta, India. These authors found anatomical variations in 22.5% of the CsW they studied, but all showed only unique anatomical variations.
Unlike all the authors mentioned, in our study we identified 2 times more multiple association of anatomical variants than single anatomical variants in the CsW we have analyzed.
Like other researchers [5,10], we also found two, three, four or five associations of anatomical variations of the constituent arteries within the same CW. Among the multiple variations, the most common were those associating two vessels with anatomical variant, and the rarest was the association of five anatomical variants within CW (only one case out of the 28 analyzed, 3.57%). However, we have already published these cases, among which there was a patient with a giant ACoA aneurysm associating hipoplasia of right ACA, hipoplasia of right PCoA, hipoplasia of left PCoA, the later ending into an unnamed extraloop originating in the ipsilateral PCA and thus forming an extrasegment in the in the posterior boundary of CW [27].
Also, Iqbal [10], in India, found 28% of their 50 CsW as having multiple associated anatomical variants, of which 20% had two variants and 8% had more than two abnormalities. Among the multiple abnormalities were recorded the association of hypoplastic PCoA with fetal contralateral PCA, or the association of hypoplastic PCoA with a duplicate ACoA. We also found in our series the same association, but with a third one added, i.e. a fenestrated right ACA.
In a study similar to ours, but with a much larger number of cases, Ranil et al [5] found out that 56.4% of their CsW had multiple associated anatomical variants.
A seminal study on this topic was conducted by a group of researchers in Poland who examined 100 brains from deceased and autopsied patients. 27% of them presented the classic model of CW, but 73% presented various anatomical variants, due to atypical aspects especially at the level of PCoA (62%), often in the form of bilateral or unilateral hypoplasia, ACoA (22%), followed by ACA (14 %) and PCA (8%). These researchers identified a single anatomical variant in 27% of CW, but two or more associated variants in 44% of cases, with five variants being associated in 1% of cases [28].
However, the morphological aspects of CW obtained by us are very different from those obtained by Cristea et al [13], who are also Romanian authors investigating the morphology of CW in the population from the Southern region of Romania by CT angiographic combined with MRI- angiographic study. These significant differences between our study and that realized by Cristea et al [13] can be interpreted either due to the techniques used (CT and MRI angiographic study vs. autopsy), but also to some particularities of the population in the Southern region compared to that in the North-Eastern region of Romania.
In our study, the prevalence of anatomical variations of the CW was quite low because patients were not selected according to the criterion of a cerebrovascular pathology, but CsW were obtained at consecutive routine autopsies in the Department of Pathology performed on the patients who died during the hospitalization, to whom an autopsy was performed in order to determine the cause of death.
Conclusions
The present study, which was performed on 96 fresh brains obtained at the anatomo-clinical autopsy, identified a 2.5 times higher number of classic circles of Willis compared to atypical circles of Willis, i.e. presenting anatomical variants. Our results showed intermediate values between those reported in various studies performed on circles of Willis obtained at autopsies. These differences can be interpreted as possible peculiarities of the population in North-Eastern region of Romania. Unlike all other studies with which we compared the results obtained, in our research two thirds of cases with variations presented multiple anatomical variants, including five simultaneous variants.
The identification of these anatomical variations of the circle of Willis in a specific population can be of great importance in assessing cerebral vascular morbidity and it is especially necessary for neurosurgeons when planning surgery for intracranial aneurysms and ligation of the internal carotid artery, regarding the correct knowledge of hemodynamics of the cerebral circulation of a patient.
36549
References
- Willis T (1665/1666) Cerebri Anatome: cui access it nervorum descriptioetusus. Amstelodami: Gerbrandum Schagen.
- Dumitrescu AM, Costea CF, Cucu AI, Dumitrescu GF, Turliuc MD, et al. (2020) The discovery of the circle of Willis as a result of using the scientific method in anatomical dissection. Rom J Morphol Embryol 61: 959-965.
- Siddiqi H, Ansar T, Fasih S (2013) Variations in cerebral arterial circle of Willis in patients with hemorrhagic stroke: a computed tomography angiographic study. J Rawalpindi Med Coll 17:215-218.
- Klimek-Piotrowska W, Kopeć M, Kochana M, Krzyżewski RM, Tomaszewski KA, et al. (2013) Configurations of the circle of Willis: a computed tomography angiography based study on a Polish population. Folia Morphol 72: 293–299.
- De Silva KRD, Silva R, Gunasekera WSL, Jayesekera RW (2009) Prevalence of typical circle of Willis and the variation in the anterior communicating artery: a study of a Sri Lankan population. Ann Indian Acad Neurol 12: 157–161.
- Kayembe KN, Sasahara M, Hazama F (1984) Cerebral aneurysms and variations in the circle of Willis. Stroke 15:846-850.
- Blackburn IW (1907) Anomalies of the encephalic arteries among the insane. A study of the arteries at the base of the encephalon in two hundred and twenty consecutive cases of mental disease, with special reference to anomalies of the circle of Willis. J Comp Neurol Psychol 17:493–517.
- Hoksbergen AWJ, Fülesdi B, Legemate DA, Csiba L (2000) Collateral configuration of the circle of Willis, transcranial color-coded duplex ultrasonography and comparison with postmortem anatomy. Stroke 31: 1346-1351.
- Riggs HE, Rupp C (1963) Variation in form of circle of Willis. The relation of the variations to collateral circulation: anatomic analysis. Arch Neurol 8:8-14.
- Iqbal S (2013) A comprehensive study of the anatomical variations of the circle of Willis in adult human brains. J Clin Diagn Res 7: 2423-2427.
- Shaban A, Albright KC, Boehme AK, Martin-Schild S (2013) Circle of Willis variants: fetal PCA. Stroke Res Treat 2013: 105937.
- Siddiqi H, Ansar T, Fasih S (2013) Variations in cerebral arterial circle of Willis in patients with hemorrhagic stroke: a computed tomography angiographic study. J Rawalpindi Med Coll 17:215-218.
- Cristea BM, Filipoiu F, Lupu G, Stroica L, Diaconescu B, et al. (2013) Study regarding the variability of the cerebral arterial circle of willis through imagistic studies. Rev Rom Anatfunctclin macro- micro antropol 12:165-167.
- Alawad AHM, Hussein MA, Hassan MA (2009) Morphology and normal variations of the cerebral arterial circle “of Willis” in Khartoum Diagnostic Centre. Khartoum Med J 2:215-219.
- Harizi (Shemsi) E, Rroji A, Gabrani S (2014) Anatomical variations of the circle of Willis in adult human brains: a case-control study in Albania. Management in Health 18:33-35.
- Macchi C, Catini C, Federico C, Gulisano M, Pacini P, et al. (1996) Magnetic resonance angiographic evaluation of circulus arteriosus cerebri (circle of Willis): a morphologic study in 100 human healthy subjects. Ital J Anat Embryol 101:115-123.
- Poudel PP, Bhattarai C (2010) Anomalous formation of the circulus arteriosus and its clinico-anatomical significance. Nepal Med Coll J 12: 72-75.
- Singh R, Kannabathula AB, Sunam H, Deka D (2017) Anatomical variations of circle of Willis – a cadaveric study. Int Surg J 4:1249-1258.
- Prasad VN, Chhetri PK, Poudel A (2017) Normal variants of the circle of Willis in patients undergoing CT angiography. JCMS-Nepal 13:190-192.
- Kapoor K, Singh B, Dewan IJ (2008) Variations in the configuration of the circle of Willis. Anat Sci Int 83:96-106.
- Nordon DG, Rodrigues Júnior OF (2012) Variations in the brain circulation – the circle of Willis. J Morphol Sci 29:243-247.
- Raghavendra DR, Shirol VS, Daksha D, Reddy AK, Desai SP (2014) Circle of Willis and its variations; morphometric study in adult human cadavers. Int J Med Res Health Sci 3:394-400.
- 23. Arjun B, Chandan G (2015) Anatomical Variants of Circle of Willis in South Indian Population: A Study by Using Magnetic Resonance Angiography. IJSR 4:1077-1080.
- Suemoto CK, Grinberg LT, Aparecida MSS, Filho J, Pasqualucci CA (2008) Anatomical variations of circle of Willis in an autopsy study in the city of São Paulo. Braz J Morphol Sci 25:157-214.
- Jin Z, Dong W, Cai X, Zhang Z, Zhang L, et al. (2016) CTA characteristics of the circle of Willis and intracranial aneurysm in a Chinese crowd with family history of stroke. Bio Med Res Int.
- Sinha I, Ghosal AK, Basu R, Dutta I (2014) Variation in the pattern of circle of willis in human brain –A morphological study and review. Al Ameen J Med Sci 7:13-19.
- Dumitrescu AM, Anca S, Costea CF, Dobrin N, Furnică C, et al. (2020) Aneurysm of the anterior communicating artery associated with multiple anatomical variants of the circle of Willis. A case report and literature review. Rev rom anatfunctclin macro micro antropol 21:192-202.
- Klimek-Piotrowska W, Rybicka M, Wojnarska A, Hołda MK (2016) A multitude of variations in the configuration of the circle of Willis: an autopsy study. Anatomical SciInt 91:325–333.

