Keywords
Obesity; Triglycerol; Adipose tissue; Kupffer cells; Endocannabinoid system; Cholecystokinin agonist
Introduction
According to the Faculty of Public Health, obesity is “an excess of body fat frequently resulting in a significant impairment of health and longevity” [1]. The global cause of obesity spread over worldwide rapidly because it is the major risk factor of metabolic diseases such as hyperlipidemia, hypertension, osteoarthritis, dyslipidemia, type 2 diabetes DM, arteriosclerosis, nutritional deficiency, obstructive sleep apnoea, musculoskeletal complications, cancer and obesity also related to imbalance in the glucose and lipid metabolism in Insulin resistance. Orthopaedic problems in children are also linked to obesity [2-5].
Obesity develops when energy gain from foodstuff and drink consumption, including alcohol, is larger than energy needs of the body’s metabolism over a prolonged period, resulting in the build up of excess body fat [6]. The percentage of body fat in women is higher than that of men it is about 25-30% in women and 15-20% in men [7]. Obesity increases the mortality and morbidity rate in developed and developing country not only in middle aged adults but also in young adults, pregnant women and in children. Obesity in pregnancy increases harmful effect on the pregnant women and also in developing foetus such as risk of miscarriage, fetal anomalies and mortality, higher rates of gestational hypertension, gestational diabetes and preeclampsia, and an increased risk of caesarean section and delivery allied complications [8,9].
When energy required to body adipose tissue that secrets triglycerol during excess food intake and releases free fatty acid FFA. It is recognized as an endocrine organ that synthesizes and secretes biologically active molecules called adipokines, which influence various homeostatic systems. In adipose tissue, lipid storage (i.e., lipogenesis) and utilization (i.e., lipolysis) are regulated by several hormones and by the nutritional state. These signals activate various transcription factors (e.g., sterol regulatory element-binding protein-1c and peroxisome proliferators-activated receptor -α/γ) and enzymes (e.g., fatty acid syntheses and carnitine palmitoyltransferase-1) to maintain lipid metabolism. Consequently, an imbalance in lipid metabolism leads to changes in adipose tissue mass. Disorders in lipid metabolism not only increase plasma FFA levels but also alter the production of adipokines, which contribute to the development of obesity-related pathologies, such as insulin resistance [4].
Etiology
Obesity is generally caused by excess energy consumption (dietary intake) as compare the energy expenditure (energy loss via metabolic and physical activity), the etiology of obesity is highly complex and includes genetic, physiologic, environmental, psychological, social, economic, and even political aspect that interact in varying degrees to promote the development of obesity [10-20].
New Targets
Deficiency of prolylcarboxypeptidase
As the hypothalamus play an vital role in food intake and metabolism it is considered as a new target in newer treatments. Identification of role of PRCP in the regulation of α-MSH in the brain may be a significant thing for knowing the mechanism of control of brain in food intake and body weight. Recently it is discovered in case of mice the eminent level of α- melanocyte-stimulating hormone (α-MSH) causes the deficiency of the enzyme prolylcarboxypeptidase PRCP which leads to weight loss and decreased food intake. It indicates that PRCP is an indigenous in activator of an appetite stimulant and α-MSH. The cardiovascular risk factors may be reduced by reducing weight loss so the pharmacotherapy of high-risk patients with obesity-related disorders may include the inhibitors of PRCP [21].
Inhibition of kupffer cells
The inhibition of Kupffer cell exerted antiobesity effects in obese. Fasting hyperglycaemia, insulin resistance and impaired glucose tolerance induced by high fat diet were improved through chronic administration of GdCl3. Interestingly; the inhibition of Kupffer cell exerted antiobesity effects in HF feeding, and lowered hepatic steatosis. Therefore, strategies targeting Kupffer cell functions could be a promising approach to counteract and related metabolic disorders [22].
Blocking citrate lyase
It is postulated that the pregnane glycosides and perhaps constituents in Standardized extract of Caralluma fimbriata prevent fat accumulation via blocking citrate lyase. Because standardized extract of Caralluma fimbriata is a competitive inhibitor of ATP-citrate lyase, an extra mitochondrial enzyme involved in the initial 25 steps of de novo lipogenesis. C. fimbriata also has hydroxycitrate HCA as active component. HCA has been reported to cause weight loss in humans without stimulating the central nervous system. Consequently, HCA reduces the transformation of citrate into acetyl coenzyme A, a step necessary for the formation of fatty acids in the liver. In addition to its effect on citrate lyase, the postulated blocking of malonyl coenzyme A by Standardized extract of Caralluma fimbriata could further lead to a decrease in fat formation in the metabolic pathway. New fat cells are formed as preadipocytes. Standardized extract of Caralluma fimbriata inhibit new fat cell formation by acting on malonyl coenzyme. Standardized extract of Caralluma fimbriata inhibits this hunger sensory mechanism of the hypothalamus [23].
Endocannabinoid system
The endocannabinoid system consists of cannabinoid receptors, their endogenous ligands The energy expenditure, appetite, as well as lipid and glucose metabolism is regulated by The endocannabinoid system. The area of interest and research is inhibition of this pathway which leads to weight loss and reduction of cardio metabolic risk factor [24].
Cannabinoid receptors: CB1 and CB2
In rodent brain cells the High-affinity cannabinoid-binding sites were discovered and subsequently in humans two cannabinoid receptors were cloned. In 1991 the cloning of Cannabinoid receptor- 1 were done, which primarily modulates food intake and energy expenditure and in 1993 Cannabinoid receptor-2, which appears to influence immune function. The location of Cannabinoid receptors-1 are CNS and various peripheral tissues such as adipocytes, hepatocytes, skeletal muscles, endothelial cells, and the gastrointestinal tract. Cannabinoid receptors- 2 are found in the spleen, thymus, and tonsils and are not believed to be involved in regulation of food intake and energy homeostasis [24]. For example, Rimonabant is selective cannabinoid 1 receptor antagonist reduces the body weight.
Endogenous cannabinoid ligands
They primarily activate CB1 and/or CB2 receptors. This suggests that obese individuals may have higher circulating endocannabinoids because of reduced degradation enzymes available [25,26].
Inhibition of pancreatic lipase
For digestion and absorption of dietary fats pancreatic lipase exocrine enzymes of pancreatic juice is essential [27].
For example, Orlistat blocks fat absorption in the small intestine by inhibiting pancreatic lipase, preventing approximately 30% of consumed fat from being digested with considerable reductions in weight, BMI, total cholesterol, LDL cholesterol, fasting insulin, and fasting glucose and improvement in glucose tolerance and reduced progression to diabetes [28].
Inhibitors of intestinal microsomal triglyceride transfer protein
Microsomal triglyceride transfer protein is necessary chaperone for the assembly of apolipoprotein B. Hepatic steatosis induced by inhibition of the hepatic form of MTP because small molecule MTP inhibitors reduced plasma lipids. Enterocytic form of MTP is the characteristics of the Gut selective MTP inhibitors [27].
DGAT I inhibitors
DGAT is expressed in different tissues like liver and white adipose tissue. The last step of triacylglycerol synthesis is catalysed by Diacylglycerol O-acyltransferas. There are two types of isozymes of DGAT that is DGAT1 and DGAT2. DGAT2 increases role of steatosis activity as well as DGAT1 plays a important role in VLDL storage assembly. Increased plasma VLDL concentrations may promote obesity thus; DGAT1 is considered a potential therapeutic target for obesity control [27].
Inhibitors of low-affinity sodium-dependent glucose co-transporters
Competitive inhibition of SGLT2, leading to enhanced glucose and energy loss through the urine, was initially regarded a promising new therapeutic strategy for the treatment of hyperglycaemia in patients with type 1 or type 2 diabetes. The sodium-glucose co-transporter-2 SGLT2 is a low affinity transport system that is specifically expressed in the kidney and plays an important role in renal glucose reabsorption in the proximal tubule. This target characterizes a different potential approach for weight loss [27].
Cholecystokinin agonist
CCK agonists possibly useful in the therapeutic target in obesity. The first gut peptide to be definitely identified as having a role enhancing the satiety response to ingested foods was Cholecystokinin [29].
Glucagon-like peptide 1
GLP-1, and the related hormone GIP (initially known as ‘gastric inhibitory hormone’, but now referred to as ‘glucosedependent insulinotropic peptide’), are examples of incretins neural or humoral factors that enhance insulin secretion. Hence GIP and GLP 1 hormones are therapeutically involved in the body weight loss.
The combined GLP-1 and glucagon receptor agonism have a positive result for reducing the food intake and weight loss. synthesised chimerae of GLP-1 and glucagon and went on to show that these molecules had in vitro action at both receptors [29].
Amylin analogues
Amylin is a peptide of 37 amino acids which is secreted by the pancreas with insulin. Its primary sites of action are considered to be located in the brainstem. Amylin class were originally developed not only for restorative use in diabetes but also shown to reduce weight loss, for example in obese patients with type 2 diabetes [27].
NPY analogues
The NPY family contains three members, pancreatic polypeptide-PP, and peptide tyrosine tyrosine-PYY, neuropeptide Y-NPY. The peptides of this family act at multiple receptors known as, Y1 Y2, Y4, Y5 and Y6. Members of a related receptor family contribute about half their amino acid sequence these receptor includes Y1, Y4, Y6, but the remaining two receptor subtypes are not linked to this group or to each other [29].
Exogenous NPY is an appetite stimulant it shows its efficiency and efficacy after its acute administration and its constant effects during chronic administration have led to the assumption that endogenous NPY could involved in the shortand long term regulation of energy balance. The antagonist NPY Y1 receptor or related receptor subtypes are primarily shown to responsible target. But later receptor subtype, Y5, appeared to be an even good applicant because Y5 receptor activation showed a similar order of potency for peptide agonists in vitro as for appetite stimulation in vivo. The antisense oligonucleotides and a selective Y5 receptor nonpeptide antagonist study shown that Y5-receptor-deficient showed no phenotype, and selective Y5 receptor antagonists had no effect on spontaneous feeding, Hence, the reduction in food intake observed in nonspecific actions to contributed in the earlier experiments [30].
PP located in the Islets of Langerhans to regulating pancreatic secretion.Y4 receptor is the major agonist of the PP [27]. Hence, it is found that the PP can reduce food intake [27].
PPY is released by the L cells lining the gut and mostly circulates as PYY3-36 for energy expenditure and fuel portioning [27,29].
Ghrelin and ghrelin receptor
Ghrelin and its receptor, play an important role in energy homeostasis the growth hormone secretagogue receptor GHSR, are believed to and appetite. Ghrelin is the first orexigenic hormone acting in the hypothalamus to stimulate food intake and has together with the GHS-R, and understood as a very accomplished anti-obesity target [31].
The research on Greline found that the efficacy of ghrelin antagonists and inhibitors of the enzyme ghrelin Oacyltransferase, which is essential to enable ghrelin to attach to its receptor as potential antiobesity therapy in weight loss. An effective treatment is yet to emerge from ghrelin blockade [32] (Figure 1).
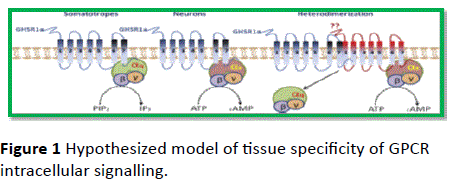
Figure 1: Hypothesized model of tissue specificity of GPCR intracellular signalling.
Melanocortin receptor
The melanocortin MC4 receptor present in all areas of brain along with hypothalamus. It integrates a cleavage of proopiomelanocortin (POMC), with an antagonist melanocortin produced by signal provided by agouti-related protein (AGRP) agonist which represents a signal provided by α-MSH. Evidence for a central function of α-MSH in the regulation of food intake comes from studies in MC4 receptor which is present in obese phenotype [31].
Leptin/Amylin
Leptin is an adipokine, which correlates between the serum concentrations positively with adipose tissue mass. Normally, leptin play an important role in negative feedback loop in the CNS to restrict food intake, and thus homeostatically the environment balance maintain a desirable degree of adiposity. Regular leptin shortage in humans is a rare form of severe early onset obesity, which is reversible with leptin therapy. However, serum leptin is elevated in obesity except in the rare instances of total leptin deficiency, and CNS resistance to leptin-mediated satiety have obese individuals. Thus, use of leptin as monotherapy for the treatment of obesity is generally ineffective. In an animal model of obesity, the simultanious utility of leptin with amylin resulted in significant weight loss. Leptin and amylin agonist Combination therapy is recently in the treatment of obesity [32].
Serotonin (5-HT)
Serotonin receptors are involved in neuroendocrine control of energy homeostasis, appetite, mood, & reward pathways and it is widely spread in the CNS. A few serotoninergic agents that were effective for weight loss [32]. The 5-HT1B, 5-HT2C and 5-HT6 receptors are of most interest for the weight management; these receptors are the subtype of 5-HT receptor [30].
These are classifying like 5-HT1A, 5-HT1B, 5-HT1D, 5-HT1E, 5-HT1F, 5-HT2A, 5-HT2B, 5-HT2C, 5-HT3, 5-HT4, 5-HT5A, 5- HT5B, 5- HT6 & 5-HT7.
5-HT5, 5-HT2 receptors exert inhibitory actions by reducing cAMP, while 5-HT2 receptors are excitatory, mediating their actions via phosphoinositol hydrolysis. All the other subtypes are exert excitatory actions by stimulating cAMP with the exception of the 5-HT3 receptor which forms an excitatory ligand gated Na+ and K+ cation channel. Three subtypes are currently deemed of particular interest in the control of body weight [29].
Oxyntomodulin
Oxyntodmoulin is cleaved from preproglucagon and released from intestinal L-cells in proportion to calories ingested. Oxyntomodulin inhibits food intake and increases energy expenditure in humans [32].
OXM consists of 37 amino acids of which 29 are in common with GLP-1. while OXM has a 50-fold lower affinity for binding at the GLP-1 receptor, it has an equal potency for reducing food intake. Studies have shown that OXM inhibits food intake and causes reduced weight gain [27].
Noradrenaline
Nordrenergic and adrenergic cell bodies are mostly found in the hind brain, predominantly in the locus coeruleus and project rostrally to the lateral and medial hypothalamus, hippocampus and cortex. Adrenergic receptors ARs are Gprotein coupled and have been classified into two broad classes (α and β) that are widely distributed in the central nervous system. Again αARs have been further sub-classified into α1 and α2 families, which upon activation produce functionally opposed effects as while α1ARs are thought to be located postsynaptically and coupled to cyclic AMP, α2ARs are located presynaptically and function as inhibitory auto receptors. The α1AR has three subtypes known as α1A, α1B and α1D and three α2ARs have also been characterised and are known as the α2AAR, α2BAR, and α2CAR. βARs are classified into three subtypes. β1 and β2 ARs are expressed in the central nervous system whereas the expression of β3 receptors expressed to the periphery, particularly to brown adipose tissue. Activation of β3ARs causes uncoupling of mitochondrial ATP production from oxidative metabolism and consequent release of energy as heat. This thermogenic response has received active consideration as an obesity treatment. β1 ARs are located postsynaptically and are widely expressed in the brain, the hypothalamus, that are relevant to feeding behaviour. β2ARs are located presynatically but, their activation by contrast with the α2 receptor, stimulates the release of noradrenalin from the synaptic terminals [29].
Dopamine
Dopamine is a second catecholaminergic neurotransmitter whose neuronal cell bodies are principally located in the substantia nigra pars compacta (A9) and ventral tegmental area VTA (A10).Dopamine receptors are classified into two subtype D1- like (D1 and D5) and D2-like (D2, D3 and D4) on the basis of pharmacological and structural similarities. Stimulation of D1 receptors with D1 selective agonists suppressed the food intake. Th Selective D2 receptor agonist, N-0437 reduced food intake, in a manner consistent with enhanced satiety [29].
Bariatric surgery
Now a day’s bariatric surgery is considered for those with class III obesity (BMI more than 40) & class II obesity (BMI more than 35) with comorbid conditions such as hypertension and type 2 diabetes.
Bariatric surgery procedures can be classified as malabsorptive, restrictive or combination of both malabsorptive and restrictive.
Intestinal microbiota as future target for weight management
Intestinal Microflora is a novel target for obesity. Traditionally Gordon and co-workers discovered that intestinal bacteria shows to have an important effect on body weight. In addition, certain antibiotics can increase body weight in rats and mice, and human data indicate that the combination of vancomycin plus gentamycin is accompanied by a significant weight gain. Several mechanisms have been suggested, including the phenomenon of “energy harvesting” by the micro flora, production of specific short-chain fatty acids interacting with certain receptors including GPR41 and GPR43, and changes in the pro /anti-inflammatory balance in the gut [27].
Conclusion
It is concluded that the management of obesity have various target as receptor because receptor gives response to the any class of drug mechanism of action. Traditionally various therapies were developed for the obesity management but recently the new types of targets are improved to reduce the risk of obesity that is the greline, leptin, amyline, MC4 etc. These are some newly invented targets within last five years. Receptor play the important role in the body mechanism hence in this review we focused obesity target as receptor.
9883
References
- Third Report of Session 2003–04, obesity, published by House of Commons Health Committee, Volume I.
- Dennedy MC, Dunne F (2010) The maternal and fetal impacts of obesity and gestational diabetes on pregnancy outcome. Best Pract Res ClinEndocrinolMetab 24: 573-589.
- Powell AG, Apovian CM, Aronne LJ (2011) New drug targets for the treatment of obesity. ClinPharmacolTher 90: 40-51.
- Lee YS, Cha BY, Choi SS, Choi BK, Yonezawa T, et al. (2012) Nobiletin improves obesity and insulin resistance in high-fat diet-induced obese mice. J NutrBiochem 24: 156-162.
- Mason HN, Crabtree V, Caudill P, Topp R (2008) Childhood obesity: a transtheoretical case management approach. J PediatrNurs 23: 337-344.
- Scotland's obesity strategy (2010) Preventing overweight and obesity in Scotland, Published by the Scottish Government.
- Katsilambros N (2000) New developments in obesity. Eur J Intern Med 11: 65-74.
- Chao CY, Shih CC, Wang CJ, Wu JS, Lu FH, et al. (2012) Low socioeconomic status may increase the risk of central obesity in incoming university students in Taiwan, Obes Res ClinPract8: e212-e219.
- Couch SC,Deckelbaum RJ Obesity and Pregnancy, Nutrition and Health: Handbook of Nutrition and Pregnancy.
- Wright SM, Aronne LJ (2012) Causes of obesity. Abdom Imaging 37: 730-732.
- González Jiménez E (2011) [Genes and obesity: a cause and effect relationship]. EndocrinolNutr 58: 492-496.
- Marta GC, Arantxa RC (2011) Dietary phytochemicals and their potential effects on obesity: A review.Pharm Res 64:438-455.
- Beechy L, Galpern J, Petrone A, Das SK (2012) Assessment tools in obesity - psychological measures, diet, activity, and body composition. PhysiolBehav 107: 154-171.
- Hinney A, Vogel CI, Hebebrand J (2010) From monogenic to polygenic obesity: recent advances. Eur Child Adolesc Psychiatry 19: 297-310.
- Sabin MA, Werther GA, Kiess W(2011) Genetics of obesity and overgrowth syndromes.Best Pract Res ClinEndocrinolMetab25:207-220.
- Puhl RM, Heuer CA (2009) The stigma of obesity: a review and update. Obesity (Silver Spring) 17: 941-964.
- Phelan S (2010) Pregnancy: a "teachable moment" for weight control and obesity prevention. Am J ObstetGynecol 202: 135.
- Prieto-Hontoria PL, Pérez-Matute P, Fernández-Galilea M, Bustos M, Martínez JA, et al. (2011) Role of obesity-associated dysfunctional adipose tissue in cancer: a molecular nutrition approach. BiochimBiophysActa 1807: 664-678.
- La Rocca JD, PA-C RN (2009) Childhood obesity: Is parentral Nurturing to blame? IJAHSP.
- Shariat-Madar B, KolteD, Verlangieri A, Shariat-Madar Z(2010) Prolylcarboxypeptidase (PRCP) as a new target for obesity treatment.Diabetes MetabSyndrObes Target Ther3:67-78.
- Neyrinck AM, Cani PD, Dewulf EM, De Backer F, Bindels LB, et al. (2009) Critical role of Kupffer cells in the management of diet-induced diabetes and obesity. BiochemBiophys Res Commun 385: 351-356.
- Saboo B, Zaveri H (2011) Recent update in management of obesity and overweight patients: standardized extract of carallumafimbriata safe and effective therapy, IJCCI. 2: 5-9.
- Isoldi KK, Aronne LJ (2008) The challenge of treating obesity: The endocannabinoidsystem as apotential target.J Am Diet Assoc108: 823-831.
- Scheen AJ, Paquot N (2009) Use of cannabinoid CB1 receptor antagonists for the treatment of metabolic disorders.Best Pract Res ClinEndocrinolMetab 23:103-116.
- Mallat A, Lotersztajn S (2010)Endocannabinoids in the pathophysiology of obesity - The liver.Drug Discov Today Dis Mech 7:3-4.
- Witkamp RF (2011) Current and future drug targets in weight management. Pharm Res 28: 1792-1818.
- Anti-obesity drugs (2003) A report of the Nutrition Committee of the Royal College of Physicians of London.
- Kennett GA, Clifton PG (2010) New approaches to the pharmacological treatment of obesity: can they break through the efficacy barrier? PharmacolBiochemBehav 97: 63-83.
- Chiesi M, Huppertz C,Hofbauer KG (2001) Pharmacotherapy of obesity: targets and perspectives.Trends PharmacolSci22: 5.
- Schellekens H, Dinan TG, Cryan JF (2010) Lean mean fat reducing "ghrelin" machine: hypothalamic ghrelin and ghrelin receptors as therapeutic targets in obesity. Neuropharmacology 58: 2-16.
- Hussain SS, Bloom SR (2011) The pharmacological treatment and management of obesity.Postgrad Med J 123: 1.

