Keywords
Perceived training needs; Resource generation; Inteprofessional training; International organizations
Introduction
The education and training of human resources for health (HRH) is an essential factor in the development of health systems. Well trained staffs provide quality services that meet the expectations and demands of the population and contribute to patient safety. Moreover it is one of the three parameters of human resources management, which are summarized as follows: "the properly trained professionals, in the right proportions, in the right positions and in a safe working environment” [1]. Education and training contribute to better responsiveness and performance of the employees [2,3].
Relevant policies of the executive management should be based on the respective population health needs assessment, in planning modern education and training activities so that health workforce meet current needs and future vision of the organizations [3]. Leadership is crucial in shaping the appropriate policy and establishing goals and strategies to achieve human resources development [4]. Key issues to be addressed to this direction is a detailed inventory of existing capacity (numbers and characteristics) of health workforce, the provision for future services, as well as improving the quality and skills, through such investments, including lifelong learning and education in new technologies. Research supports the findings that HRH want to participate in curriculum design as they have a strong opinion about their needs [5]. Studies showed that curricula based on trainees’ needs are more effective and popular [6,7].
Assessing health professionals’ perceived training needs contribute to a suitable course creation that will equip them with competencies to better cope with population needs. According to CDC, [2,3] all public health workers must demonstrate core competencies in: analytical reasoning, policy development/ programme planning, communication, cultural competency, community dimensions of practice, basic public health sciences, financial planning and management, leadership and systems thinking and, emergency preparedness. Core public health services should be taken into consideration in formulating such a course [8].
Hence preparing competent professionals for the 21st century equipped to address current and future population needs requires an interdisciplinary organisational framework, to develop scientific and technical competences and analytical skills for decision-making based on ethical standards and scientific evidence. At the same time, health professionals should be prepared to adopt a systemic approach of public health through training in management and leadership, cultural competencies and development of interdisciplinary communication skills [9]. The human resources should be equipped with intercultural and interpersonal skills to cope with, situations such as the increased population mobility due to leisure, economic and other reasons. Today, more and more people travel. There is also increasing migration flow in Europe, and we expect growth of health tourism and cross border health issue due to greater population mobility. Diseases that were exotic or unknown a few years ago now have made their appearance in Europe, i.e. the West Nile virus and malaria [10,11].
In Greece, public health has been neglected for many years. A number of agencies public, private and NGOs in the field in local, regional and national levels were poorly staffed and operated under an outdated framework.
In 2003, the first law concerning public health ever was voted (L 3172/2003), which was reformed, in 2005 (L 3370/2005). A few years later, Greece got its first Action Plan in Public Health 2007- 2013 [12]. Vision and priority statements for public health referred to improving population’s living conditions and quality of life. It also defined short and long-term targets, plans and interventions, determined the agencies, sectors and administration levels responsible for multisectoral and intersectoral implementation of this policy.
An urgent matter in public health was personnel training. This should be done in two directions, to educate all those already serving in modern roles and stay current and to educate sufficient numbers of health professionals who will move from other health services to staff public health. The training should be done in a short time frame to enable the implementation of the Action Plan in Public Health to provide tangible results of these reforms [8].
Other concerns included outdated curricula, lack of sufficient enrichment courses of field workers, the need for professional development and the need to create a pool of personnel prepared to perform essential public health services within an increasingly complex system, the lack of public health culture in the country, as well as the outdated organisation and management of health services.
The Ministry planned to train 4.000 employees of all cadres in public health competencies8 to staff public health services to ensure that competencies are in line with defined international standards and the needs of local populations [12]. The executive management of the Ministry asked for international support WHO/EURO and the Nordic School of Public Health, Sweden. These two Organizations agreed to offer 16 short courses on international health issues, based on perceived needs of the trainees. Furthermore, this type of courses was provided for the first time to a member state by WHO/EURO.
This initiative intended to provide knowledge and skills and create competent health professionals able to implement public health policy and programmes according to population needs of the respective district in which they live and work. While usually training curricula are planned by the institutes, this international curriculum was designed taking into consideration the trainees’ expectations. Literature on assessing training needs in order to formulate curricula through international partnerships is very limited especially in our country. The aim of this paper was to assess health professionals’ training needs in public health, across disciplines and health settings so that the respective training course matched their requirements. The research questions were as follows: What were health professionals perceived training needs? Did needs differ between health cadres? What factors were associated with needs?
Materials and Method
Settings
In 2004, the Hellenic Ministry of Health and Social Solidarity, the National School of Public Health (NSPH), the World Health Organization Regional Office for Europe (WHO/EURO) and the Nordic School of Public Health, Sweden, partnered to create a continuing education course in public health [13,14]. They signed a memorandum of understanding.
The training programme “Policies for the Development and Promotion of Public Health in National and International Level” based on international scientific bibliography was formulated by the NSPH. The curriculum lasted for 150 hours classroom or internet-based instruction [15] and skills demonstration. The curriculum was based on the international scientific bibliography as well as the proposals of the partner organizations. The courses were organized at the regional level (ex 17 Health Regions (HR) now merged and consolidated to 7). Each HR could choose between a classroom and an e-learning course.
The training programme was publically advertised via several means such as the press, scientific web pages and information letters to the public entities. In each interdisciplinary course 25 professionals from a range of governmental agencies participated. Furthermore, 3-5 more trainees, senior lecturers from the NSPH and executive managers from the Ministry attained in an observing capacity, as this was regarded an opportunity to broaden their knowledge in public health and stay current.
The National School of Public Health (NSPH) undertook the realization of training nationally.
It was formulated in 6 modules. NSPH provided the five modules while WHO the sixth module. The formulation of the programme aimed at updating trainees’ knowledge and providing new insights in public health (Table 1).
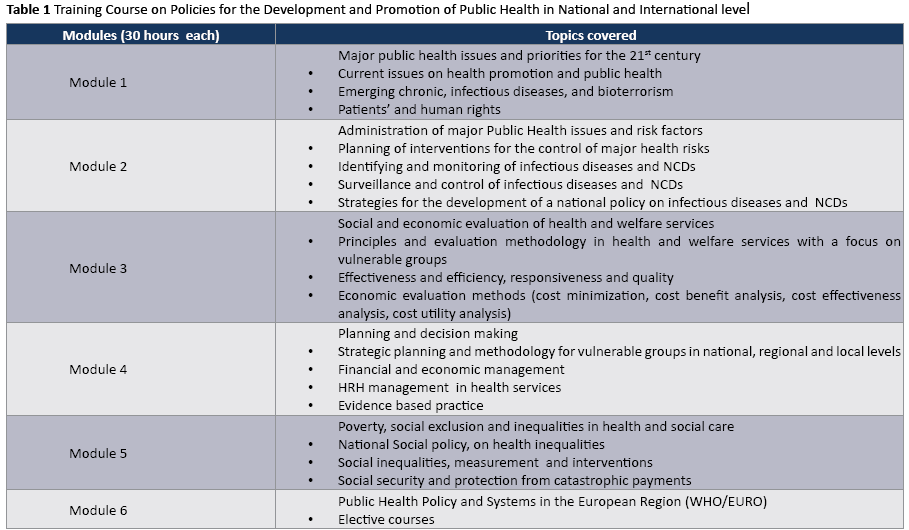
WHO/EURO provided training for 360 participants (12 courses, 30 hours per course) and the Nordic School of Public Health to 120 participants (4 courses, 30 hours per course). Here we draw on the training provided by WHO Regional Office for Europe Copenhagen, Denmark. Furthermore, each group with WHO/ EURO had the possibility to draw their own curriculum according to their needs by choosing among 22 suggested topics. These topics would help them develop the core competencies defined by the Public Health Functions Steering Committee in 2000 [8]. These were based on the ten essential public health functions provided to the population [16]. It was offered as a mixture of lectures, case studies and exercises within working groups [17]. Furthermore, they received a DVD with the presentations and discussions, training materials, exercises and group work for broader training in public health. The training took place from February 2006 until May 2007.
Participants
In the survey, we included all the participants in the courses from these health regions that chose the international training module. They were doctors, nurses, administrative personnel, social scientists, technicians and scientific non-medical employees. According to the Hellenic Statistical Authority [18] under the last category professionals such as, engineers, pharmacists and chemists are listed. The trainees worked with Ministries and Regional Health Authorities, hospitals, health centres and municipalities.
Measures
In 2006, the research team developed a questionnaire in Greek to assess the needs of health professionals towards training in public health. This was based on an international bibliography review. The questionnaire was structured in three (3) sections: the first one recorded demographic data, the second the motivation to participate in the course and expectations from it, while in the third part the elective topics were listed. We implemented a pilot survey to confirm its precision, sensitivity and responsiveness [19,20].
Before the training with WHO/EURO, we distributed the questionnaire to all the members of each group. The facilitator gave an oral presentation on the purpose of the training to each group of trainees as well as instructions on how to complete the questionnaire, emphasizing the protection of the participants’ anonymity.
We asked the trainees to choose ten of the 22 subjects and rank them from 1 to 10 (1=first preference, 10=last preference).
The questionnaire was filled out in the presence of researchers where possible. In the remaining cases (electronic courses), it was sent out through e-mail. In this case to facilitate their choice, the coordinator, conveyed a brief content description of each topic, as well.
Data collection
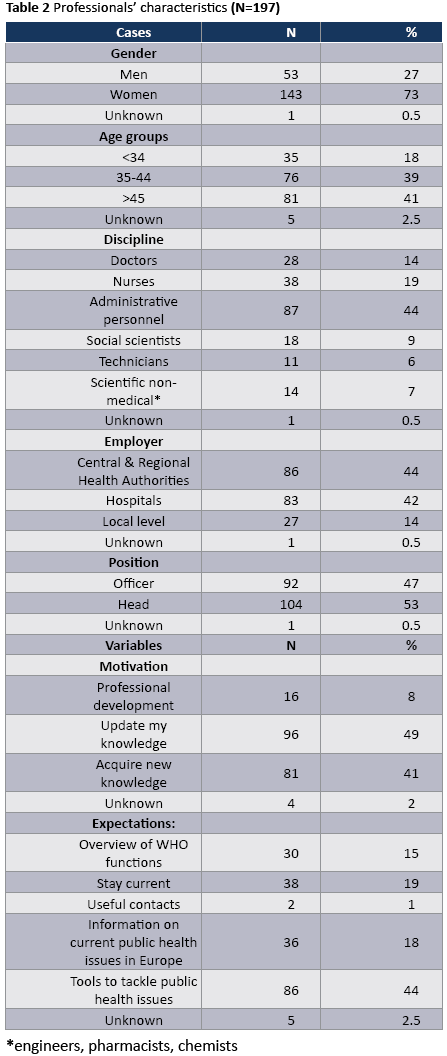
Data collection took place from 2006 to 2007 using the structured self-report questionnaire. We distributed 300 questionnaires to the 12 groups of trainees, before the training course. We received 235 completed questionnaires. A total 14 of the respondents (6%) did not answer all the questions and were excluded from this analysis. Furthermore, there were respondents who might not have understood the guidelines well so that the same person gave the same preference for different topics. Thus, the analysis was limited to 197 questionnaires (return rate 65.66%). In Table 2 we present the characteristics of the sample.
Statistical analysis
Statistical analysis was performed with the use of SPSS software, version 20.00. Descriptive statistics were used to estimate the frequencies of the study variables. A series of one way analysis of variance (ANOVA) between groups was performed to investigate whether individual characteristics of health professionals were associated with training topics. For all cases a p-value of less than α=0.05 confidence level was considered to indicate statistical significance.
The facilitator processed and mailed the results to WHO counterparts. In this way, the presenters were able to prepare the chosen topics in due time.
Results
Table 2 presents the demographic characteristics of 197 professionals. The majority of participants were women (n=143, 73%) and the rest men (n=53, 27%). With regards to age, 41% were more than 45 years old. Doctors were (n=28, 14%), nurses (n=38, 19%), administrative staff (n=87, 44%), social workers (n=18, 9%), technicians (n=11, 6%), scientific non-medical personnel (n=14, 7%). They worked mainly with Central and Regional Authorities (n=86, 44%). Senior officers were (n=104, 53%). As the main motivation pointed out the need to update their knowledge (n=96, 49%) and to acquire new knowledge (n=81, 41%). With regards to expectations from the course they underlined that they want to be equipped with tools to tackle public health issues (n=86, 44%) and stay current (n=38, 19%).
Table 3 presents the percentage of participants who ranked the 22 topics.
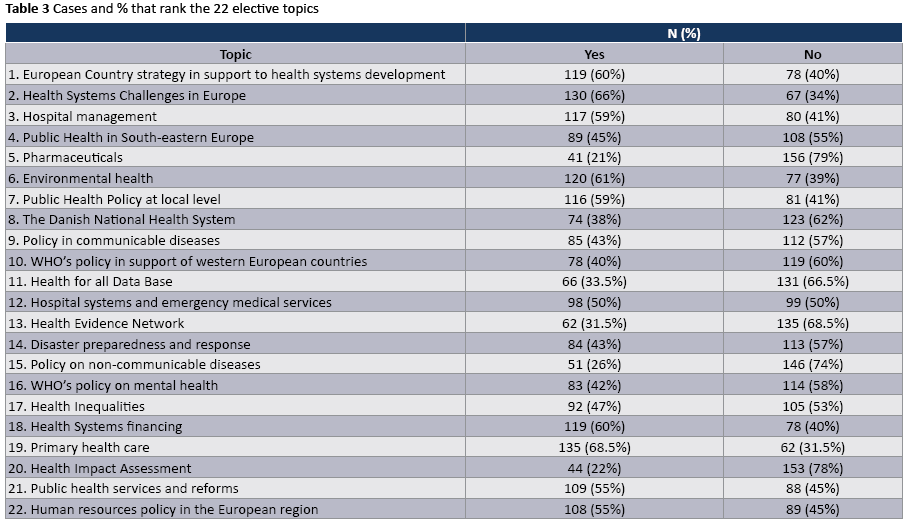
Table 4 shows preferences between the 197 respondents who selected and ranked in order of preference the first 10 out of the 22 subjects. All the 22 topics were presented in descending order of selection for classification.
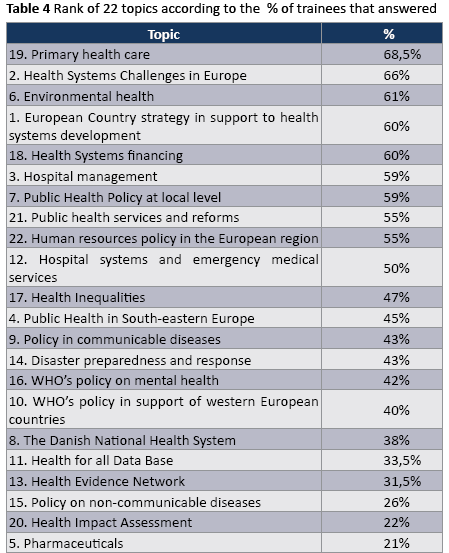
Their first preference was 19. Primary health care (68.5%), followed by 2. Health Systems Challenges in Europe (66%) while 5. Pharmaceutical (21%) was ranked last.
Table 5 shows their choice in other words how they ranked the 22 elective topics (1=first preference, 10= last preference).
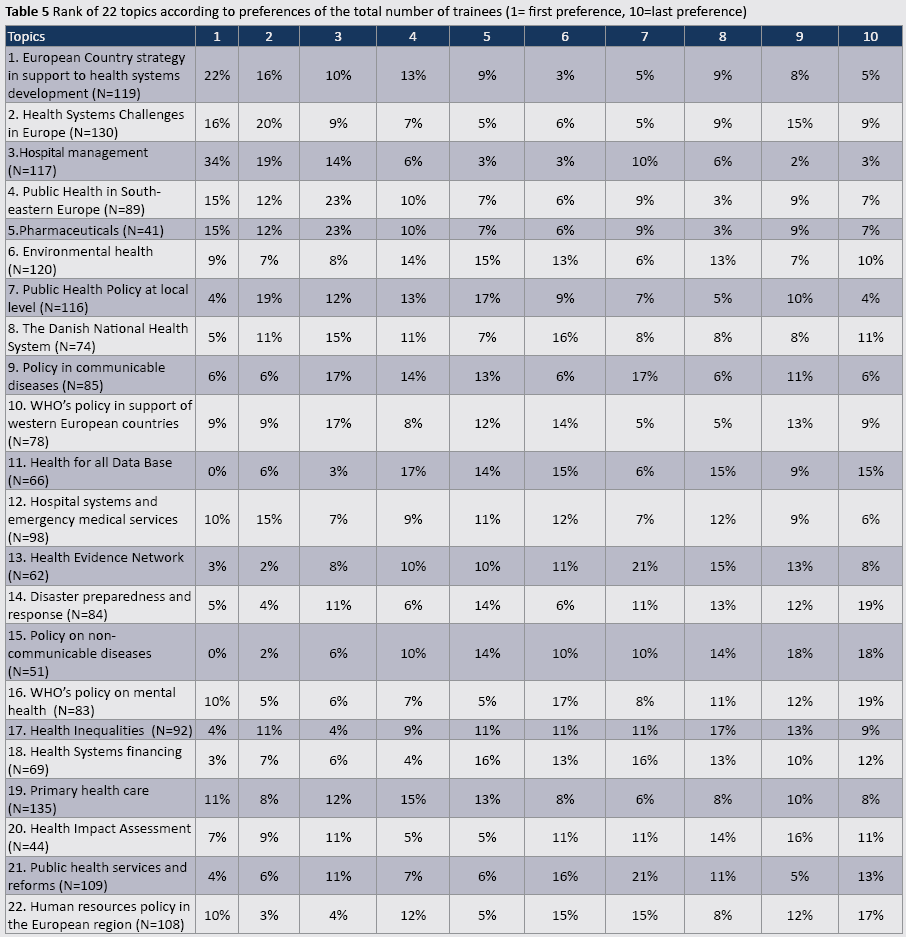
We then calculated the mean score for each topic. Using ANOVA we compared mean scores between the variables gender, age, position, profession, and employer.
In general, preferences did not differentiate according to gender. However, statistically significant differences in the order of preferences occurred in relation to the items 3 and 22. Men rated higher 3. Hospital Management (mean score for men=8.31 vs women=7.21, p=0.036), while women 22. Human resources policies in the European region (mean score for women 5.29 vs mean score for men 3.51 p=0.002).
Depending on the occupation, statistically significant differences were observed for topics 2, 10, 16 and 22. The mean score 2. Health Systems Challenges in Europe was (doctors 7.31, nurses 5.82, administrative personnel 6.70, social workers 5.50, technicians 4.33, scientific non-medical 3.80 (p=0.026). With respect to subject 10. WHO's policy in support of western European countries, the mean score was: doctors 4.06, nurses, 5.00, administrative personnel 6.19, social workers 7.50, technicians 6.67, scientific non-medical 5.00 (p=0.048). Topic 16 WHO’s policy on mental health showed mean score for doctors 2.41, nurses 4.33, administrative personnel 4.33, social workers 6.00 technicians, 6.50 scientific non-medical 7.83 (p=0.02). Furthermore, human resources policy in the European region was also statistically significantly different among the different occupations (doctors nurses, 3.14 administrative personnel 5.33, social workers 4.25, technicians 5.40, scientific non-medical 5.86 (p=0.048).
The ranking did not depend on age (p>0.05 in all cases). According to position there was statistically significant difference towards 10. WHO’s policy in support of western European countries with supervisors achieving higher mean score (6.38) in comparison with officers (4.86), p=0.018.
There was no statistically significant difference in the ranking of preferences in relation to the reason of choosing this training program (a) professional development, (b) expand/ update of knowledge (c) facilitating the exercise of my duties (p>0.05 in all cases).
No statistically significant difference occurred in terms of expectations (a) overview of WHO functions (b) stay current (c) networking (e) be informed on current public health issues in Europe (f) tools to tackle public health issues (p>0.05 in all cases).
We recoded the professionals depending on whether they provide personal or non-personal care in accordance with the definition of WHO [1].
The trainees prioritized educational needs in the same way on most issues. Statistically significant differences were found in subjects 2, 17, and 22. The topic 2. Health Systems Challenges in Europe was ranked differently by professionals who provide non-personal care mean score 6.70 compared with those who provide personal care mean score 5.55, (p=0.042). Furthermore, the topic 17. Health Inequalities was prioritised significantly different mean score personal care 5.50, non-personal care 4.31 (p=0.034). Moreover, topic 22. Human resources policy in the European region was ranked differently non personal care 5.33, personal care 4.14 (p=0.029).
With regards to employer, topic 17. Health Inequalities, showed statistically significant differences between professionals. Mean score for professionals employed in hospitals, 5.84, primary health care 4.85 central and regional authorities 4.24 (p=0.031).
Discussion
Education and training of health professionals is a fundamental part of management and a prerequisite to improve access, quality and efficiency of services to meet the growing and changing needs of the population. As life expectancies increase and epidemiological profiles change with chronic diseases dominance, people live longer with ill-health and need more complex services. Country profile analysis, provide the framework for designing appropriate policies and interventions that improve population health. Furthermore, it should take into consideration biomedical technology, knowledge update and international health [21]. Targeted training courses are more effective and help updating health workforce knowledge and professional development. The need for continuing development of a knowledge base for defining competency and for establishing the workforce contribution to an effective public health infrastructure was the main driver for the establishment of this programme.
The programme drew on core functions in public health [21-23] to develop the core competencies health professionals should demonstrate in daily practice to meet the expectations of the population in a changing environment.
These training courses were very popular (intake rate 1:10) among the Greek professionals. They considered themselves privileged to receive training by WHO staff. WHO/Europe’s technical experts provided the groups of trainees with a general overview of the most important aspects of public health policies and systems, by giving them the best and state-of-the-art knowledge.
The majority of trainees were women, as many more women serve the Greek public sector than men. Traditionally, women choose to work in the public sector, where applied incentives to support the family, such as maternity leave and parenting exist, despite the fact that the salaries there are often lower than those of the private sector. Furthermore, professional development is based on seniority/years of service. Based on years of service they eventually become supervisors and thus there is the need for a solid knowledge in human resources for health policies and management. However, men are usually offered the executive director post in hospitals and other health settings and this may explain their preference in hospital management.
In general, men and women pointed out the need to acquire new skills aiming to be more efficient as the main motivation reason to participate in the course, while in terms of expectations they pointed out the need to acquire tools on best practices. Primary health care, health systems and environmental health were underlined as knowledge priorities. Doctors pointed out their need for a deeper knowledge in health systems while the type of employer influences their needs as expected.
Furthermore they perceived Primary Health Care as their first priority and this has been underlined as the main reason of population dissatisfaction in our country. The lack of primary care networks has been identified by the scientific community in a variety of work so far [24]. It has been constantly coming up by the scientific community, and the general public. According to Kyriopoulos et al. [25], the major weaknesses of primary health care system referred to (a) access to services due to both the geographic morphology of our country (islands and mountainous areas) and the increased demand especially during the tourist season, staff maldistribution and shortages (b) quality and (c) responsiveness to population needs in terms of services offered and (d) underfunding in relation to the other forms of care. The reorganization of the system towards effectiveness and efficiency is essential. They are aware that the reforms in the National Health System should start with this issue. Primary health care has been a key component of all efforts towards health system reforms over the past 30 years. But despite the favourable conditions as reflected in legislation and relevant reports, the legal documents remained largely inactive [26].
After about 30 years of the NHS, there is a need to evaluate and reorganise it. Last year a reform in primary health care was introduced aiming at rationalising the provision of services increasing access to care and cost containment. The establishment of the Health Information System was a fundamental issue in the country. This mechanism will allow the collection of data on the organisation, operation and financing of the system and allow the evaluation based on scientific evidence and therefore the development of a strategy for priorities and interventions [27]. These weaknesses have led to an increased pressure in hospitals generated both in out-patients and inpatients departments [28]. The lack of staff in primary health care prevents from the provision of high quality of care, in terms of among others disease and patient management, mobilising local partnerships, empowering people, prevention and health education. Especially regarding vulnerable groups, they usually do not use such services because they either cannot afford to pay or they are not informed. As a result they consume more costly hospital services. Complimentary are their second and third choices Health Systems Challenges in Europe and Environmental Health. These expressed the need of pressing reforms in the National Health System and concerns on issues affecting population health [29].
Furthermore, the second choice suggests the desire to learn the characteristics in terms of organisation, management and financing of health systems in Member States. Also they want to learn the similarities and differences with the National Health System of our country to be able to make comparisons on individual characteristics, apply similar techniques, and learn about WHO policies to support the development of countries’ health systems in the Region.
With regards to the above doctors gave higher grade on Health Systems Challenges compared to other professionals because they may want to be informed about the concerns in other countries. As they lack the relevant knowledge in their academic curricula there is a pressing need to acquire certain knowledge. They may want to develop the respective skills to cope with similar situations due probably to large numbers of immigrants both legal and illegal in our country [30-33].
Moreover, those who work in the hospitals, listed “Health Inequalities” higher, mostly because, due to the lack of a developed primary health care all population in need end up in hospitals to receive such services.
They highlighted topic 5. Pharmaceuticals at the bottom. This is a highly specialized matter and difficult to handle in terms of pricing and prescribing. This rather involves professionals who provide direct health care services and mainly physicians who prescribe and nurses who provide relevant guidance to patients on their use. So it seemed that the interprofessional nature of the programme may not allow the emergence of the issue to a higher preference. It would be interesting to see the doctors' prescribing patterns in a subsequent follow up study.
Finally the choice of 20. Health Impact Assessment in the penultimate position shows that they do not have relevant organisational culture for such topics. The relative ignorance of the professionals in its content and the lack of similar culture in our country, might not give it a higher position on the list. Possibly deeper knowledge of the subject would have raised it higher since it is interconected with topic 6. Environmental health. However we should underline that after the completion of the respective training with WHO, the health professionals did realise the importance of these issues. In their post course evaluation they highly rank them (but this assessment goes beyond the scope of this study and will be the subject of another article).
This course was the first of this type provided to a member state by WHO. In spite of preliminary concerns referring to the limited training capacities of WHO staff, the course became a successful model that combined academic expertise in curriculum development and teaching technologies with practical expertise in course content and audience needs. Furthermore, WHO may draw on this training material to provide such courses to other requesting member states. Moreover this curriculum urged three organizations to formulate a partnership and placed our country in the European public health scene as a key stakeholder. Targeted training programmes are more efficient and valuable tools for the management of health workforce, because they create competent professionals, contribute to patient safety and overall experience and lead to workforce job satisfaction and retention. To compliment this, the relationship among trainees’ individual competencies, organizational performance and health outcomes should be evaluated. By combining this type of projects with performance assessment, we will be able to understand the added value of the training and how this helped improve knowledge and efficiency.
5187
References
- Parfitt B (2009) Health reform: the human resource challenges for Central Asian Commonwealth of Independent States (CIS) countries. Collegian 16: 35-40.
- CDC (2004) Core Functions, Essential Services, and Core Competencies, Part One.
- CDC (2004) Core Functions, Essential Services, and Core Competencies, Part Two.
- Rouiller J, Goldstein IL (1993) The Relationship Between Organizational Transfer Climate and Positive Transfer of Training. Human Resource Development Quarterly 4: 377-390.
- Overstreet KM, Eidsvoog KE, Orsetti RF, et al. (2006) Educational interventions and outcomes – a literature review of CME regarding Institute of Medicine (IOM) competencies. CE Meas 1: 17–26.
- Ewert EG, Baldwin-Ragaven L, London L (2011) Training Trainers in health and human rights: Implementing curriculum change in South African health sciences institutions. BMC Med Educ 11: 47.
- Farris KB, Demb A, Janke KK, Kelley K, Scott SA (2009) Assessment to transform competency-based curricula. Am J Pharm Educ 73: 158.
- Public Health Functions Steering Committee (2000) Public Health in America.
- Frenk J, Zulfiqar LC, Bhutta A, Cohen J, Crisp N, et al. (2010) Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. The Lancet 1923–58.
- Gebbie K, Merrill J, Tilson HH (2002) The public health workforce. Health Aff (Millwood) 21: 57-67.
- Institute of Medicine of the National Academies (2008) Retooling for an Aging America: Building the Health Care Workforce. National Academies Press. Washington, DC.
- Ministry of Health and Social Solidarity (2008) Public Health Action Plan. Ministry of Health, Athens.
- Lichtveld MY, Cioffi JP, Baker EL Jr, Bailey SB, Gebbie K, et al. (2001) Partnership for front-line success: a call for a national action agenda on workforce development. J Public Health Manag Pract 7: 1-7.
- Alexander LK, Dail J, Horney MV, Davis JW, Wallace J et al. (2008) Partnering to Meet Training Needs: A Communicable-Disease Continuing Education Course for Public Health Nurses in North Carolina. Public Health Rep 123: 36-43.
- Alexander L, Horney J, Markiewicz M, MacDonald P (2010) 10 Guiding Principles of a Comprehensive Internet-Based Public Health Preparedness Training and Education Program. Public Health Rep 51-60.
- Interprofessional Education Collaborative Expert Panel (2011) Core competencies for interprofessional collaborative practice: Report of an expert panel, Washington, D.C.
- World Health Organization (2007) Training in Public Health. Regional Office for Europe, Copenhagen.
- Hellenic Statistical Authority (2008) Household Budget Survey 2008. Population and Labor Market Statistics Division, Greece.
- Burns R (2000) Introduction to Research Methods. (4th edn), SAGE Publications, USA.
- Bradburn N, Sudman S, Wansink B (2004) Asking Questions: The Definitive Guide to Questionnaire Design for Market Research, Political Polls, and Social and Health Questionnaires, Inc. Revised Edition, John Wiley & Sons, USA.
- HM Government (2010) Healthy Lives, Healthy People: Our strategy for public health in England. Majesty Press, UK.
- Michigan Public Health Training Center (2001) Training Needs Survey. Research Results, Michigan.
- Joint Task Group on Public Health Human Resources (2005) Building the Public Health Workforce for the 21st Century. A Pan-Canadian Framework for Public Health Human Resources Planning.
- Lapao LV, Dussault G (2011) PACES: a national leadership programme in support of primary-care reform in Portugal. Leadership in Health Services 24: 295-307.
- Kyriopoulos J, Lionis Ch, Demoliatis J, Merkouris B-P, Economou Ch (2000) Primary Health Care: a cornerstone in health reforms. Primary Health Care 12: 169-188.
- Mossialos E, Allin S, Davaki K (2005) Analysing the Greek health system: a tale of fragmentation and inertia. Health Econ 14: S151-168.
- Despena A (2009) Healthcare delivery services in Greece. World Hosp Health Serv 45: 35-37.
- Kaitelidou D, Kouli E (2012) Greece: the health system in a time of crisis. Eurohealth 18: 12-14.
- Andrioti, Altanis P, Merakou K, Skitsou A, Charalambous G et al. (2010) Can World’s Health Organization model “matching services to new needs be applied in our country? Primary Health Care 22: 29-39.
- Atreja A, Menta NB, Jain AK, Harris AK, Ishwaran H, et al. (2008) Satisfaction with web-based training in an integrated healthcare delivery network: do age, education, computer competencies and attitudes matter? BMC Med Educ 8: 48.
- Drexel C, Jacobson A, Hanania NA, Whitfield B, Katz J, et al. (2011) Measuring the impact of a live case-based, multiformat, interactive continuing medical education programme on improving clinician knowledge and competency in evidence-based COPD care. Int J Chron Obstruct Pulmon Dis 6: 297–307.
- Lockyer J (2003) Multisource feedback in the assessment of physician competencies. J Contin Educ Health Prof 23: 4-12.
- Swick S, Hall S, Beresin E (2006) Assessing the ACGME Competencies in Psychiatry Training programs. Acad Psychiatry 30: 330-351.

