Keywords
Stroke; Motor skills; Physical therapy; Complementary therapies; Neurology; Geriatrics
Introduction
Stroke is a neurological syndrome with high prevalence in adults and elderly. It is one of the largest causes of death in the world and one of the main causes of hospitalizations [1]. Signs and symptoms are related to blood spillage or arteries obstruction of cerebral blood supply [2]. The main motor complications are muscle weakness, spasticity and atypical motor sensory patterns, such as hemiparesis in the contralateral side of the lesion. It can also present sensory and cognitive alterations, difficulty in speaking or understanding speech [3].
Among the sequels, the motor damage stands out by negatively interfering in individual's daily life activities. Difficulty in global and fine motor skills influences elderly independence in essential tasks such as eating, bathing, dressing and walking [4]. The effects can extend from three to six months after the stroke, considering that 55% to 75% of the patients still have deficits in the functions of grabbing, holding and handling objects [5].
In this context, aquatic physiotherapy is a specialty that stands out in the treatment of dysfunctions caused by strokes [6]. Exercises in aquatic ambience utilize the water´s physical properties and allow joint overload relief, spastic musculature relaxation, soft tissues flexibility and improvement of venous return [7]. Furthermore, group therapy in water stimulates socialization, self-confidence, self-esteem increase and the patients interest in continuing rehabilitation [8].
Psychomotricity can be included in the intervention to prevent and treat the worsening of symptoms [9]. Psychomotor therapy is a science that aims to increase the subject's ability to interact with the environment. Based on a biopsychosocial approach, it combines pedagogical and manual therapeutic experiences [10]. Therefore, functional improvements are expanded using the principles of psychomotricity in aquatic ambience [11].
In this way, the objective of this study was to verify the effects of aquatic psychomotricity in elderly people with strokes sequels.
Materials and Methods
A quantitative, cross-sectional and descriptive study developed in the State University of Pará. For inclusion in the study, the individuals should be aged between 60 and 75 and sequels after stroke. The exclusion criteria were: uncontrolled hypertension, dermatological changes, infected open wounds, acute disorders, severe respiratory failure, urinary infection and otitis.
The sample was selected systematically and composed for twenty four elderly people. Data were collected through an identification sheet created by the researchers and the Gerontopsychomotor Observation Scale, in order to trace the individuals’ psychomotor profile, before and after intervention.
Gerontopsychomotor Observation Scale encompasses aspects about psychomotricity, cognition, language, social affective relationship and autonomy in daily life activities. It is composed by items with score from 0 to 4 according to the elderly performance. 0-Behavior not observed or not applied; 1-Does not do/does not present, 2-Does with much difficulty/Rarely presents; 3-Does with some difficulty/Sometimes presents; 4-Does without difficulty/Presents frequently [12].
Intervention was executed in groups of four patients, during eight sessions of fifty minutes, twice a week. It was divided in ten minutes’ walk associated with breathing, two psychomotor dynamics of twenty minutes and ten minutes for global relaxation. The psychomotor elements contemplated in the twelve dynamics were: body scheme, tonus, balance, space-time organization, rhythm, laterality, breathing, global and fine motor skills. It was included individual tasks, in order to provide self-knowledge, and group dynamics to improve socialization. Materials used were hula hoops, boards, party balloon, balls, aquatube and dumbbells.
Data obtained were arranged in the software Excel® 2010 to made tables and figures, in addition to Real Statistics® for statistical analysis. Descriptive analyses of the variables were performed to test the normal distribution of data by the Shapiro-Wilk tests. To guarantee the significance of the data, the analysis was executed using the Mann-Whitney U test with 5% significance level (p ≤ 0.05).
This study was approved by the Research Ethics Committees of University of the State of Pará. Protocol number 3.300.397, in accordance with resolution n° 510/2016 of the National Health Council.
Results
Twenty-four individuals participated in the research but ten were excluded because they didn’t complete the eight sessions. Among the 14 participants, 6 (42.9%) were female and 8 (57.1%) were male, with mean age equal to 67.2 years. In respect of diagnosis, 11 (78.6%) individuals reported being affected by ischemic stroke, 2 (14.3%) hemorrhagic stroke and 1 (7.1%) both types of stroke.
Gerontopsychomotor Observation Scale items that constitute the global motor skills assessment are arranged in figure 1 and 2. First corresponding to the score achieved in the initial evaluation and the second is related to the final (Figure 1).
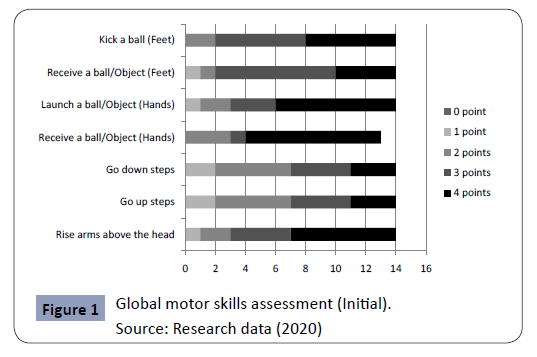
Figure 1: Global motor skills assessment (Initial).
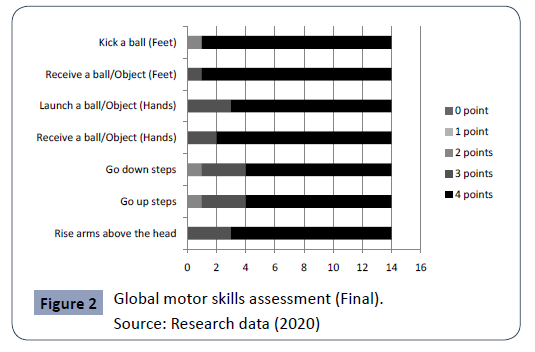
Figure 2: Global motor skills assessment (Final).
Comparing the initial and final scores, it is possible to observe the patient's progress. All items had an increase of individuals with the maximum score (4 points) in last session. Those who couldn't accomplish the proposed items (1 point), at the end of intervention were able to carry out with much difficulty (2 points) or some difficulty (3 points) (Figure 2).
The data related to the fine motor skills items are arranged in graphs 3 and 4, illustrating the initial and final evaluations, respectively. In the first moment (Figure 3), some users reached the maximum score, demonstrating good preservation of this psychomotor aspect (Figure 3).
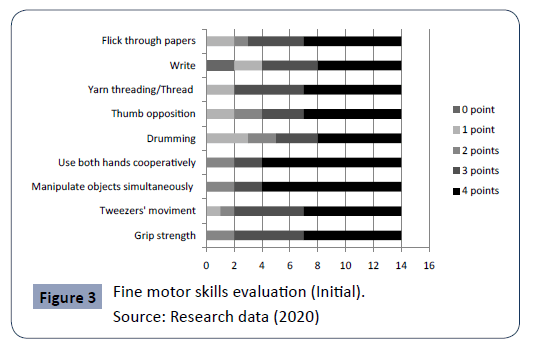
Figure 3: Fine motor skills evaluation (Initial).
Moreover, the individuals gain after psychomotor dynamics performance is evident by contrasting the data obtained in both graphs (3 and 4). Those who got the highest points remained with the same score and those with a lower score got one or more points. However, two elderly got 0 point on write item because they didn't know how to do (Figure 4).
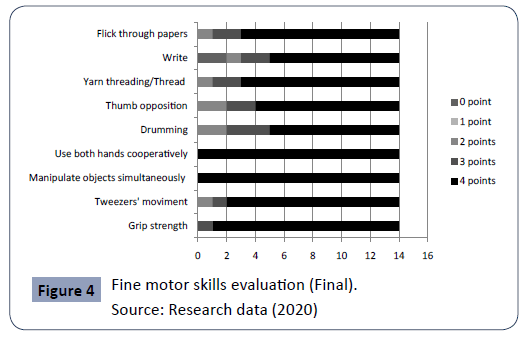
Figure 4: Fine motor skills evaluation (Final).
The statistical analysis exposed in Table 1 demonstrates that both motor skills obtained a significant result. However, global motor coordination achieved more significant results (p=0,001) (Table 1).
| |
|
Mean |
Median |
P-value |
| Global motor skill |
Initial |
21,5 |
22,5 |
0,001* |
| |
Final |
26,5 |
28 |
| Fine motor skill |
Initial |
28,71 |
32,5 |
0,046* |
| |
Final |
32,5 |
36 |
Source: Research data (2020)/ * statistically significant result (Mann-Whitney Test)
Table 1 Statistical analysis of Global and Fine motor skills.
Discussion
The majority of stroke patients evaluated was elderly males and affected by ischemic stroke. Regarding gender, Medeiros’ research contrasts the present result, which demonstrated that women have potentials to increase the chance of developing the disease (migraine, dyslipidemia). However, such divergence can be justified considering the low demand of man for health services, making them more susceptible to pathology. The predominant etiology of this study corroborates with the literature and is related to main risk factors, such as hypertension [13].
Psychomotor tasks performed in the aquatic ambience assist the execution of movements and body displacement. Consequently, it can improve the global motor coordination of lower limbs, such as gait, and of upper limbs, such as functional reach (dos Santos). In this research there was evolution in the global motricity score, mainly of the lower limbs items, to go up and down steps, kick and receive a ball. Santos et al also obtained positive results on the gait performance of elderly people who practiced aquatic psychomotricity, improving functionality.
Fine motor skills are the movement performed by hands and essential for holding, grasping and manipulating objects. It is a complex capacity that decline along the aging process and can be compromised by the stroke. One of the fine motricity characteristic most impaired after stroke is grip strength [14]. In this study it was observed that the item of grip strength was what the patients obtained the best results. Initially, only seven elderly reached four points and at the end, thirteen individuals reached the maximum score.
The results obtained in assessment of global and fine motor skills were statistically significant (p=0,001 e 0,046), emphasizing aquatic psychomotricity positive effects in the rehabilitation of these aspects. The benefits of exercise in water are ratified by the Saquetto' meta-analysis [15], which indicates greater effectiveness when compared with land exercise for improve muscle strength, balance and mobility in post stroke people. Moreover, combine both exercises was more effective in improving mobility, gait, functional reach and quality of life. In addition, the intervention of this research was carried out in group, as it promotes socialization and the expansion of interpersonal relationships. It improves communication and motivation for learning, making rehabilitation more effective and pleasant [16]. In this way, psychomotor practices ensure the body's experience in integrating the dimensions: motorinstrumental, emotional-affective and practical-cognitive, helping to maintain and improve motor skills [17].
As a limitation of the study, the sample was reduced due to current pandemic scenario. However, even with limited data, the research shows positive results with respect to global and fine motor skills of elderly with stroke sequels.
Conclusion
Based on the interpretation of the data obtained in the present study, it appears that the application of psychomotor dynamics in aquatic environment corroborates for a significant improvement in the global and fine motor skills of elderly people with stroke sequels, mainly in the lower limbs, such as, improved gait, balance and postural control. In addition to developing better coordination, manipulation and visual-motor skills, thus directly optimizing the functionality in the daily activities.
32675
References
- Silva PLN, Santos LS, Ribeiro DDD, Guimarães HDG, Esteves KAF, et al. (2018) Analysis of the prevalence of stroke in patients assisted by a hospital Análisis de la prevalencia de accidente vascular encefálico en pacientes asistidos por un hospital. J Manag Prim Health Care 9: e4.
- Botelho TS, Neto CDM, Araújo FLC, Assis SC (2016) Epidemiology of stroke in Brazil. Health Topics 16: 361-377.
- Vaz RA (2016) Physiotherapy Practice in acute stroke treatment - Systematic review. Physiopedia.
- Rosa TSM, Bastilha GR, Hoffmann CF, Bastilha GR, Cielo CA (2015) Speech therapy and physiotherapy intervention in a woman after ischemic stroke. Sci Med 25.
- Belchior ACS, Araújo LS, Assis SC (2018) Evaluation of the functionality of patients with stroke sequel using the MIF Scale. Fisioterapia Brasil 19: 208-217.
- Bezerra MVA, Vasconcelos TB, Câmara TMS, Sousa CT, Macena RHM, et al. (2016) Benefits of the hydrotherapy in the stroke patient with sequel: a review of the literature. Saúde 7-14.
- Matsumoto S, Uema T, Ikeda K, Miyara I, Nishi T, et al. (2016) Effect of underwater exercise on lower-extremity function and quality of life in post-stroke patients: a pilot controlled clinical trial. J Altern Complement Med 22: 635-641.
- Costa MRDV, Lima RC, Lopes CP, Shirahige L, Albuquerque PL (2016) Effect of hydrotherapy on the endurance and quality of life in stroke survivors. Con Scientiae Saude 16: 259-265.
- Navarro GIA, Fonseca C (2018) Psychomotor intervention on eldelry with osteoarticular problems. J Aging & Innovation 7: 184 -192.
- Ingwersen KG, Vobbe JW, Pedersen LL, Sørensen L, Wedderkopp N (2019) Effect of psychomotricity in combination with 3 months of active shoulder exercises in patients with chronic shoulder pain: Primary results from an investigator-blinded, randomised, controlled trial. Arch Phys Med Rehabil 100: 2136-2143.
- Santos SL, Soares MJGO, Ravagni E, Costa MML, Fernandes MGM (2014) Walking performance of elderly practitioners of psychomotricity. Rev Bras Enferm 67: 617-622.
- Freitas MM (2017) A psicomotricidade no Campus Neurológico Sénior-implementação de um programa psicomotor nas doenças neurodegenerativas. Ulisboa.
- Medeiros CSP, Silva OAP, Araújo UB, Souza DE, Cacho EWA, et al. (2017) Social and Functional Profile of Userswith Stroke Assisted by the Family Heealth Strategy. Rev Bras Science health 21: 211-220.
- Allgöwer K, Hermsdörfer J (2017) Fine motor skills predict performance in the Jebsen Taylor Hand Function Test after stroke. Clin Neurophysiol 128: 1858–1871.
- Saquetto MB, Silva CM, Martinez BP, Sena CC, Pontes SS, et al. (2019) Water-Based Exercise on Functioning and Quality of Life in Poststroke Persons: A Systematic Review and Meta-Analysis. J Stroke Cerebrovasc Dis 28: 104341.
- Silva FMMF (2017) Psychomotor intervention in gerontopsychiatry at Casa de Saúde da Idanha. Ulisboa.
- Santos SL, Soares MJGO, Ravagni E, Costa MML, Fernandes MGM (2014) Walking performance of elderly practitioners of psychomotricity. Rev Bras Enferm 67: 617-622.

