Keywords
Renal patients, dialysis, chronic kidney disease
Introduction
The major function of the kidney is the filtration and secretion of the final products of metabolism and the excess of electrolytes. Permanent failure of the kidney to accomplish its functions is called chronic kidney disease (CKD) and failure to sustain life, is called end stage renal disease (ESRD) [1,2].
The most frequent causes of CKD are diabetic nephropathy, hypertension, glomerulonephritides, interstitial nephritis, pyelonephritis, polycystic kidney disease, obstructive nephropathy. CKD can also be the final result of untreated acute kidney injury (AKI) caused by infections, medicines, toxic substances heavy metals including lead, cadmium, mercury and chromium [3-6].
The selection of the renal replacement therapy (RRT) modality depends on physical and socio-demographic characteristics of the patient. Renal transplantation (RT) is the best RRT option because it assures better quality of life and longer survival; nevertheless due to the scarcity of transplants, peritoneal dialysis (PD) and mainly hemodialysis (HD) are applied in most cases [1].
It is well known that patients on RRT are of greater risk for complications and worst prognosis in comparison to patients with the same co-morbidities but not on RRT. Many of these people have also other co-morbidities and often present non specific symptoms such as malaise and fatigue [4,6,7].
The complications of RRT vary according to the selected type of therapy. Patients on HD often experience hypotensive episodes, muscular cramps, itching, arrhythmias, and anaphylactic responses during the sessions. They also often develop infections and bacteraemia due to various interventions and the CKD associated immunosuppression. Finally, a high percentage of hospital admissions occurs due to vascular access dysfunction [1]. Patients on PD often experience episodes of peritonitis that may lead to dysfunction of the peritoneal membrane and eventually transfer of the patient to HD [8-12]. On the other hand, transplanted patients may face rejection episodes and increased rate of infections and cancers [13-16].
Aim of the study
The aim of the present study was to examine a) the major causes that lead to ESRD, b) the various causes of hospitalization in the dialysis population and c) the association of patients’ and treatment characteristics with mortality.
Patients and methods
The studied population consisted of all prevalent patients on PD or HD in the University Hospital of Heraklion between September 2009 and September 2010. Causes of morbidity and hospitalizations were examined for all dialysis patients with at least one admission in the renal ward during the same period, while mortality was investigated for a more extended period of 33 months (September 2009 to June 2012). The data were collected through the patients’ medical records.
The research protocol included the following parameters: sex, age, cause of ESRD, presence or not of diabetes mellitus, duration and type of dialysis, type of vascular access, number and causes of hospitalizations in the nephrology ward, length of stay in each admission, type of infections and the corresponding pathogens.
Data were analyzed with descriptive statistical analysis, t-test, Kaplan Maier analysis and Cox regression analysis, using the Statistical Package for Social Sciences (SPSS) version 17.0.
The protocol of the research and data collection was approved by the Hospital’s Ethics Committee. The data from medical records of each patient were used exclusively for the purpose of the study. During the study, all issues of confidentiality and anonymity were met.
Results
The patient population consisted of 123 patients with ESRD (55.3% men) with a mean age of 65.3±15.2 years (range 16-85 years). The majority of patients (62.6%) were on HD, while 37.4% were on PD. The mean dialysis vintage was 65.1±64.2 months (range 1-264 months). The major cause of ESRD was diabetic nephropathy (19.5%) followed by glomerulonephritides and ESRD of unknown etiology (18.7% each), hypertensive nephropathy (13.8%), chronic interstitial nephritis (11.4%), adult polycystic kidney disease (ADPKD) (8.9%), ischemic nephropathy (6.5%) and finally chronic allograft nephropathy (2.4%) (Figure 1).
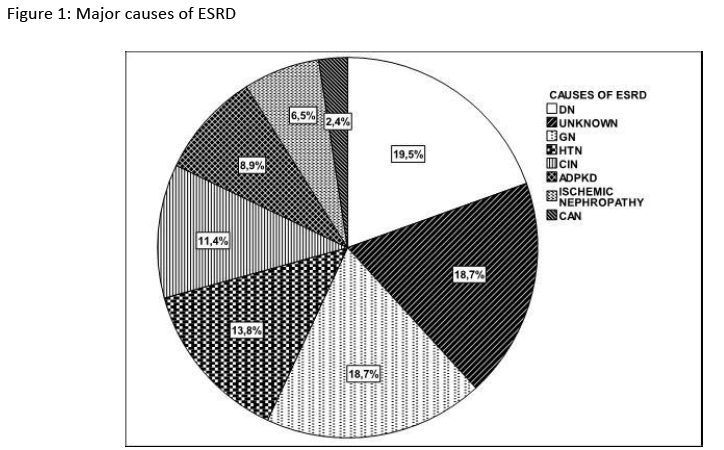
Figure 1: Major causes of ESRD
The vast majority of HD patients (75.3%) had a functioning arterial-venous fistula (AVF), 15.7% had an arterial-venous PTFE graft (AVG), 6.5% a permanent jugular catheter (PJC) and 2.5% a temporal jugular catheter at the time of assessment. Therefore more than 90% of the patients had a patent AV access for HD.
In terms of hospitalizations, 54% of all dialysis patients were admitted in the renal ward at least once during the observation period (overall 124 admissions or 1.008±1.5 admissions per patient per year, Figure 2). One patient with ADPKD was admitted 12 times due to recurrent cholangitis secondary to bile duct lithiasis and boosts of pancreatitis. The mean duration of hospitalization was 6.1±6 days (range 1-28) with the vast majority of patients (66%) staying in hospital for less than 6 days (Figure 2). The major causes of hospitalization were infections (37.9%), vascular access dysfunction or repair (15.3%), heart problems (11.3%), gastrointestinal hemorrhage (7.5%), various interventions such as repositioning of a catheter, parathyroid ablation etc. (2.4%), cerebrovascular accident (1.9%) and other causes (23.7%). Infections included bacteraemia due to central catheter infection (40.4%), peritonitis in PD patients (19.1%), gastroenteritis (12.8%), respiratory tract infections (12.8%), urinary tract infections (6.4%) and other infections (such as cholangitis, skin infections etc) 8.5%.
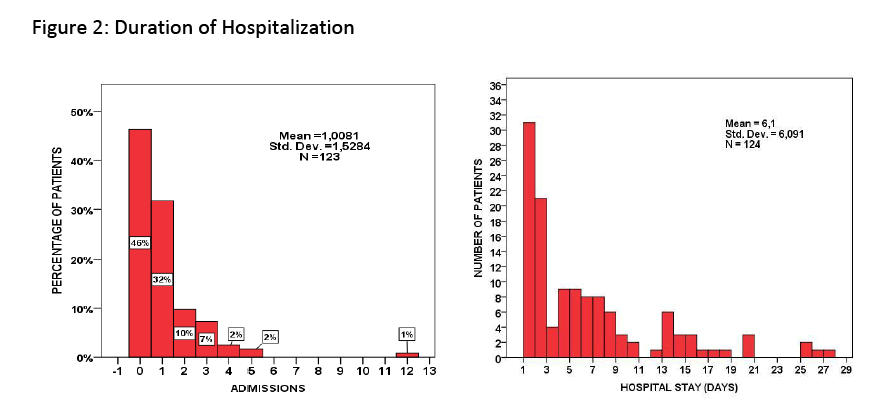
Figure 2: Duration of Hospitalization
Isolation of the pathogenic microorganism was not possible in 47% of admissions due to infections while in the remaining cases the isolated microorganisms included Staphylococcus Aureus (10.6%), Escherichia Coli (6.4%), Staphylococcus Epidermidis (4.3%), Enterococcus species (8.5%), Proteus Mirabilis (4.3%) klebsiella Pneumoniae (2.1%), H1N1 (2.1%) and other species with a lower frequency.
Cardiac problems as a reason for hospitalization included pulmonary edema (57.1%), faint episodes, pulmonary embolism, decompensated heart failure and myocardial infarction (7.1% each). In terms of hospital admissions and duration of hospitalization there was no significant difference between genders, mode of dialysis, type of vascular access and even the presence or not of diabetes.
Patients relatively new on dialysis (i.e. vintage ≤45 months) had more admissions (1.15±1 vs. 0.68±1.2 admissions per patient-year; p=0.03) and longer stay (7.1±8 vs. 3.2±7 days; p=0.007) than patients having been on dialysis for more than 45 months. Contrary to dialysis vintage, advanced age (above the median of 68 years) was as expected associated with increased morbidity in terms of admissions and length of hospital stay (1.15 vs. 0.7 admissions and 6.8 vs. 3.6 days respectively; p=0.03 for both comparisons).
Thirty two percent of patients died during the observation period (40 deaths in 33 months) and 0.8% was offered a kidney graft. The crude Cox regression analysis showed that there was no significant difference regarding survival between the two genders (p=0.33) and between patients with or without hospital admission (p=0.52). Age, diabetes and mode of dialysis were significant determinants of survival but in the multivariate analysis only age and mode of dialysis retained their significance (Table 1). In particular HD was associated with a 46% reduced risk for death as compared with PD (p=0.046, Figure 3) and each year of age with an additional risk for death of 3.6% (p=0.018).

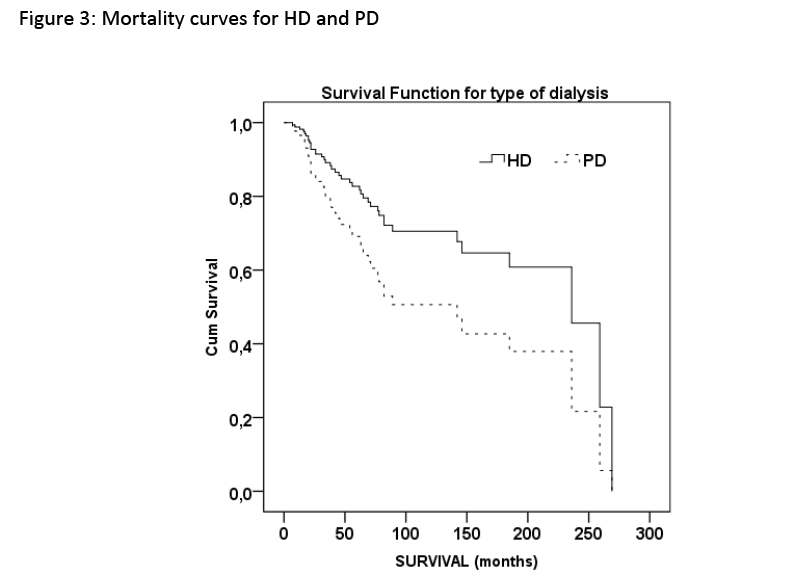
Figure 3: Mortality curves for HD and PD
Discussion
In the present study 123 patients with ESRD were followed up for one year to evaluate co-morbidities that required hospitalization in association with epidemiological characteristics such as gender, age, diabetes, mode of dialysis and admissions in the hospital (a marker of overall morbidities or well being). The mortality in the same cohort was evaluated during a longer period of 33 months.
The percent rates for the major causes of ESRD in our prevalent population in 2009 was very similar to the average rates reported for the whole of Europe by the ERA/EDTA registry 2009 annual report [17]. In particular, the major cause of ESRD was diabetic nephropathy (19.5%), a percentage that is much lower than that reported (33%) for the United States [18]. It is of interest that a much higher proportion of patients are receiving PD in our center (37.4%) as compared to the rest of Greece (8.6%) as well as several other European countries (4-14%). This finding may be related to the mountain terrain of our island that impedes easy approach to the hospital based hemodialysis units of the urban areas.
In our prevalent HD patients, 75.3% had a functioning AVF, 15.7% a functioning AVG and only 9% carried a jugular catheter which is in accordance to the European standards [19]. Despite the low percentage of central catheters in our population, catheter related infections comprised a major cause of hospital admissions. This finding indicates the need for further reduction in catheter usage with a careful surveillance and early repair of problematic fistulas. Another major cause of hospital admissions was related to cardiac morbidity, in particular pulmonary edema. Therefore a more careful assessment of patients’ dry weight could substantially reduce admission rates and morbidity.
Admission rates and hospital stay length in our cohort appear improved than other centers, a finding that is difficult to interpret especially when considering our population’s relatively advanced age and long dialysis vintage [20,21]. Interestingly, patients with longer dialysis vintage had fewer hospitalizations and shorter hospital stay compared to patients who are new on dialysis. This finding implies that patients may need some time for their medical condition to stabilize after starting dialysis as well as for several associated problems, such as anemia and hypertension, to subside. An alternative explanation could be that during the first years of dialysis the patients with severe co-morbidities (and highest hospitalization rates) die, while healthier patients with fewer hospitalizations survive longer [22]. In support of this statement, the mortality curves shown in figure 3, for both HD and PD, were steeper during the first 50 months than afterwards. Therefore early years on dialysis are burdened with a greater morbidity and mortality risk. Another worth mentioning finding of this study concerns the mortality difference between HD and PD. It was apparent that after the first 2 years the two curves deviate in favor of HD. This finding should be seen with caution though, since some co-morbidities were not taken into account in this study. For example in our center, patients with severe heart failure are usually treated with PD rather than HD, a practice that could negatively affect the survival rates in our PD group. Finally, the study population consisted of patients on PD or HD treated in one hospital, therefore the findings of the study should be viewed under this limitation.
Conclusions
Identification of the major causes of morbidity in dialysis patients can lead to improving strategies for reduction of complication rates, improvement of quality of life and sparing of resources. Two major causes of hospitalization emerged in this study: catheter related infections and pulmonary edema. Therefore two simple measures such as the vigorous assessment of the dry weight and avoidance of central catheters could substantially reduce morbidity and hospitalization rates. Caution must also be exercised in patients who are new on dialysis since they comprise the most vulnerable group in terms of morbidity and mortality.
The conduct of similar studies in each nephrology centre and the exchange of their experience would be beneficial for better allocation of resources and for the provision of advanced medical and nursing care to patients with ESRD.
2656
References
- Thomas N. Renal Nursing. University Studio Press, Thessaloniki, 2003. (In Greek)
- Vlahogiannis I. Clinical nephrology and hypertension. Ed., Paschalidis, Athens, 2009. (In Greek)
- Zirogiannis P, Pieridis A, Diamantopoulos A. Clinical nephrology, volume B. Technogramma Publications, Athens, 2005. (In Greek)
- Ioannidis I. Clinical Nephrology. Rotonda Publications, Thessaloniki, 2007. (In Greek)
- Matziou-Megapanou V. Nephrology Nursing. Ed., Lagos, Athens, 2009. (In Greek)
- Lemone P, Burke K. Medical and Surgical Nursing 3rd edition, volume B’. Ed. Lagos, Athens, 2006. (In Greek)
- Sahini-Kardasi A, Panou M. Medical and Surgical Nursing, 2nd edition, volume A. Beta Publications, Athens, 1997. (In Greek)
- Harris SA, Lamping DL, Brown EA, Constantinovici N. Clinical outcomes and quality of life in elderly patients on peritoneal dialysis versus hemodialysis. Perit Dial Int 2002; 22: 463–470.
- Mehrotra R. Peritoneal dialysis in adult patients without end-stage renal disease. AdvPerit Dial 2000; 16:67-72.
- Barretti P, Moraes TM, Camargo CH, Caramori JC, Mondelli AL, Montelli AC, et al. Peritoneal dialysis-related peritonitis due to Staphylococcus aureus: a single-center experience over 15 years. PLoS One 2012; 7(2):e31780.
- Thirugnanasambathan T, Hawley CM, Badve SV, McDonald SP, Brown FG, Boudville N, et al. Repeated peritoneal dialysis-associated peritonitis: a multicenter registry study. Am J Kidney Dis 2012; 59(1):84-91.
- Ghali JR, Bannister KM, Brown FG, Rosman JB, Wiggins KJ, Johnson DW, et al. Microbiology and outcomes of peritonitis in Australian peritoneal dialysis patients. Perit Dial Int 2011;31(6):651-62.
- Zirogiannis P, Pieridis A, Diamantopoulos A. Clinical nephrology, volume D. Technogramma Publications, Athens, 2005. (In Greek)
- Zirogiannis P, Pieridis A, Diamantopoulos A. Clinical nephrology, volume C. Technogramma Publications, Athens, 2005. (In Greek)
- Anantharaman P, Schmidt RJ. Sexual Function in Chronic Kidney Disease. National Kidney Foundation 2007; 14(2): 119-125.
- Takahiro Itai, Hideaki Amayasu, MichitoKuribayashi, Naoko Kawamura., Motohiro Okada, AkishiMomose, et al. Psychological effects of aromatherapy on chronic hemodialysis patients. Psychiatry and Clinical Neurosciences 2000; (54)4: 393-397.
- ERA-EDTA Registry. ERA-EDTA Registry Annual Report 2009. Academic Medical Center, Department of Medical Informatics 2011; Amsterdam, The Netherlands.
- Luke RG, Strom TB. Chronic renal failure. In Stein JH (ed). International medicine 4th ed. 1994; St Louis, Mosby.
- Pisoni RL, Young EW, Dykstra DM, Greenwood RN, Hecking E, Gillespie B, et al. Vascular access use in Europe and the United States: results from the DOPPS. Kidney Int 2002; 61(1):305-16.
- Sun Y, Kassam H, Adeniyi M, Martinez M, Agaba EI, Onime A, et al. Hospital admissions in elderly patients on chronic hemodialysis. IntUrolNephrol 2011; 43(4):1229-36.
- Li PK, Chow KM. Infectious complications in dialysis--epidemiology and outcomes. Nat Rev Nephrol 2011; 8(2):77-88.
- Chaudhary K. Peritoneal Dialysis Drop-out: Causes and Prevention Strategies. Int J Nephrol 2011; (2011), Article ID 434608, 7 pages.

