Raghav Kapoor*, Sumeet Swapan Roy, Goel Nikita, and Rahul Saini
Department of Medicine, Jawahar Medical Foundation’s Annasaheb Chudaman Patil Memorial Medical College, Dhule, Maharashtra, India
- *Corresponding Author:
- Raghav Kapoor
Department of Medicine
Jawahar Medical Foundation’s Annasaheb Chudaman Patil Memorial Medical College
Dhule, Maharashtra, India.
Tel: 08928648644
E-mail: raghavsmart07@gmail.com
Received Date: June 22, 2021; Accepted Date: August 24, 2021; Published Date: August 31, 2021
Citation: Kapoor R, Roy SS, Nikita G, Saini R (2021) Cheiro-Oral syndrome due to Acute Lacunar Thalamic Infarct. J Neurol Neurosci Vol.12 No.8:386.
Introduction
The Diagnosis of Cheiro- Oral Syndrome is difficult by clinical examination alone. The involvement of perioral area and ipsilateral distal fingers gives a clue to diagnosis [1]. We are reporting a case of a 46-year-old who was admitted with complaints of peri-oral numbness on right side associated with the weakness in right upper limb and lower limb. Cheiro-Oral Syndrome can arise from an involvement of the spinothalamocortical and trigeminothalamocortical tract between pons and sensory cortex [2]. The area of involvement corresponds to the area involved in the brain. The syndrome can also be accompanied by deficits in other cranial nerves, the ipsilateral lower extremity, and/or including ipsilateral ataxia. Often the deficits include incomplete involvement of the face or extremities, making this diagnosis easily missed in the acute setting [3] (Figures 1 and 2).
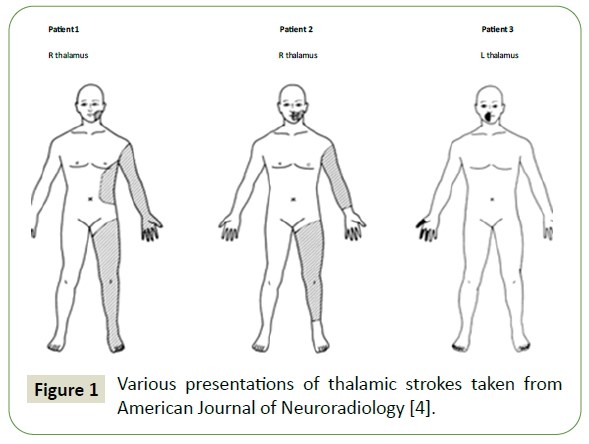
Figure 1: Various presentations of thalamic strokes taken from American Journal of Neuroradiology [4].
Figure 2: MRI of our case report.
Case Report
A 46-year-old male presented with acute onset weakness of right upper and lower limb with right perioral numbness since one day. The symptoms were associated with vertigo. Patient was conscious; alert, following commands, plantar withdrawal, Deep tendon reflexes were normal. Muscle tone was normal, and power on left upper and lower limb was 5/5 while in the right upper and lower limb it was 4/5. Pupils bilaterally equally reacting to light, no nystagmus. Patient had perioral numbness, hot cold sensations were normal. With vitals normal, blood pressure was 140/ 90 mmHg. Pulse of 90/min. The patient has no history of trauma, seizure or loss of consciousness. MRI Brain was done which was suggestive of acute lacunar infarct in left thalamic region with few small chronic ischemic foci in supratentorial white matter. CTA showed focal stenosis in bilateral V4 segment of vertebral arteries. Intervention neurology opinion was taken who advised for DSA which showed critical stenosis in bilateral vertebral artery V4 segment. He was started on dual antiplatelet and other supportive treatment. Patient was managed conservatively with dual antiplatelet, antivertigo, antidiabetic medications, daily physiotherapy and responded well to the given treatment.
Discussion
Cheiro-Oral Syndrome is reported in literature as having a number of variants, Including lower extremity sensory loss, ataxic hemiparesis, and oculomotor deficits. Our case presents with perioral numbness on the right side with ipsilateral weakness with involvement of left thalamic region with critical stenosis in bilateral vertebral artery V4 segment.
Many recent and past studies that are done have involvement of the posterior limb of the internal capsule, corona radiata, thalamus and brainstem [4-8]. Tongue involvement is often seen in some patient where lingual nerve of trigeminal nerve is involved affecting 2/3rd of the tongue. These variable clinical presentations make lacunar infarcts far less likely when sorting out exact diagnosis. The suspicion can be concreted with a history of sudden onset of symptoms and in a setting of numerous vascular risk factors. A cardiac workup and DSA is required to achieve an exact pathology.
A small infarct or small hemorrhage was found to be the leading cause of Cheiro-Oral Syndrome while other causes include Tumor, vascular malformation, atherosclerotic stenosis, myocardial ischemia, atrial fibrillation and multiple site infraction. Our patient had critical stenosis in bilateral vertebral artery V4 segment and management was started accordingly [9].
The location of the lesion in most cases arises from the pons, thalamus, cortex, or medullary oblongata. The spine may be the location of another possible unusual lesion seen in previous literature [10].
Since some of the infarcts are preventable, the primary goal is to manage its risk factors. Counseling the patient about the risk factors and ways to prevent them which include smoking cessation, statin and antiplatelet therapies, exercise and stress reducing practices could further minimize its recurrence rate. A close follow-up also reduces the risk of future stroke.
Conclusion
We demonstrate Cheiro-Oral Syndrome associated with thalamic stroke to highlight the neurological implications of this syndrome. It is of prime importance for doctors to identify the symptoms and do a full stroke workup including a cardiological workup which can prevent recurrent strokes and further complications.
39692
References
- Satpute S, Bergquist J, Cole JW (2013) Cheiro-Oral syndrome secondary to thalamic infarction: a case report and literature review. The neurologist 1: 22.
- Wu YH, Liu KT, Yeh IJ, Chang CW (2018) Cheiro-Oral syndrome caused by thalamus hemorrhage: A case report. Medicine.
- Shintani S, Tsuruoka S, Shiigai T (2000) pure sensory stroke caused by a cerebral hemorrhage: clinical-radiologic correlations in seven patients. American journal of neuroradiology 1: 515-20.
- Ikeda K, Iwasaki Y, Kishi H, Imai K, Kinoshita M (1995) Brain stem cheiro-oral syndrome: neurological signs for brain stem lesions. Clinical neurology and neurosurgery 1: 192-194.
- Hotta M, Yasaka M, Moriyasu H, Oita J, Yamaguchi T (1994) Ataxic hemiparesis with ipsilateral cheiro-oral syndrome due to a single lacunar infarct at the border between the posterior limb of the internal capsule and the corona radiata. Rinsho shinkeigaku= Clinical neurology 1: 163-166.
- Igarashi O, Iguchi H, Ogura N, Ichikawa Y, Kiyozuka T, Kawabe K, Maruyama M, Fujioka T, Ikeda K, Iwasaki Y, et al. (2006) Cheiro-oral-pedal syndrome due to brainstem hemorrhage. Clinical neurology and neurosurgery 1: 507-510.
- Yasuda Y, Watanabe T, Tanaka H, Akiguchi I, Kimura J, Kameyama M, et al. (1997) Unusual sensory disturbance in the thoracic region after stroke: Relationship to cheiro-oral and cheiro-oral-pedal syndrome. Journal of the neurological sciences 9: 68-75.
- Omae T, Tsuchiya T, Yamaguchi T (1992) Cheiro-oral syndrome due to lesions in the corona radiata. Stroke 23: 599-601.
- Chen WH, (2009) Cheiro-oral syndrome: A clinical analysis and review of literature. Yonsei medical journal 50: 777-783.
- Lin HS, Yin HL, Lui CC, Chen WH (2011) Spinal cheiro-oral syndrome: A common neurological entity in an unusual site. Neurologiai neurochirurgia polska 45: 583-589.

