Keywords
Cigarette smoking; Health; Adolescents
Introduction
Cigarette smoking is a very wide spread activity and consumption of cigarette has today reached the level of a global epidemic [1]. Every year 5,500 billion cigarettes are manufactured and 1.1 billion people smoke cigarette worldwide [1,2]. In Nigeria, about 93 million sticks of cigarette are produced annually, with every one of these cigarette sticks being consumed [3]. Cigarette smoking has been found to be associated with heart and chronic obstructive lung diseases. Lung and other cancers (bladder, pancreas, upper respiratory tract, oesophagus, stomach and leukemia) are increasingly being associated with cigarette smoking [1]. Millions of people suffer illness and disability due to cigarette smoking [2]. Cigarette smoking is associated with reduced life expectancy not only for active smokers but for passive smokers as well.
Many factors have been put forward for adolescents’ engagements in smoking. These include normal developmental changes, psychological factors, and social environment. Under normal developmental changes, influence of peers, the need to conform and direct craving for cigarettes use have been mentioned. For psychological factors, emotional problems such as low self-esteem, dissatisfaction with life, less social confidence, need for approval, anxiety, restlessness and antisocial factors have been identified. Considering social environment, family influences (having parents who are unstable and engage in cigarette smoking) role of the media (for instance advertisements for cigarettes, portraying people who smoke cigarettes as sophisticated, sexy, manly in movies) have also been mentioned [3].
It is projected that over the next 50 years close to 450 million deaths would be caused by tobacco use, and 70% of this death will come from developing countries, despite the fact that it is preventable cause of death [4]. Adolescent is the age group between 10-19 years [5]. The term “out-of-school adolescent” is used to define several groups of young people: those who have dropped out of school, those who never attended school, or those who participate in non-formal school programs [4]. Out-of-school adolescents may fail to acquire fundamentals of basic education and life skills 4 and may have little formal knowledge on health related risk of cigarette smoking compared with in-school-adolescents. Knowledge of health problems associated with smoking is a major reason for not smoking by never smoked adolescents, which means that awareness on health problems associated with cigarette smoking through health education and antismoking campaigns in schools may contribute to adolescents not smoking [4].
While it has been established that many smokers start before the age of 18 years, and that cigarette smoking is the first drug of choice to be use by adolescent in a sequel that may include alcohol marijuana and hard drugs, of serious concern, is the increasing trend in smoking prevalence amongst adolescents especially those that are out-of-school and the likelihood that many of these adolescents who begin to smoke at an early age, will continue to do so throughout adulthood.
This study was carried out due to the paucity of data regarding cigarette smoking among out-of-school adolescents in the country. Although studies examining smoking among youths have been documented in Nigeria, these are skewed towards describing pattern of use amongst in-school youths, and usually in urban areas [2]. However, negative attitude towards smoking initiation and persistence may be commoner amongst out-of-school youth because of their aggregation in areas lacking adult supervision. Understanding cigarette smoking among out of school adolescents would be important in designing intervention strategies for control of cigarette smoking among this population. It is against this background that this study becomes relevant coupled with the fact that no previous study on cigarette smoking has been conducted among out-of-school adolescents in sokoto. Findings from this study would also provide baseline data for future reference and intervention measures.
Materials and Methods
This was a descriptive cross-sectional study conducted among out-of-school adolescents in Sokoto metropolis. The study was conducted during school hours so as to capture adolescents who were not in school. Adolescents who were in enrolled in school, but found in the study sites (truants) were excluded from the study. Ever used of cigarette in this study referred to adolescents who had smoked cigarette at least once in their life time, while current smoking of cigarette referred to adolescent who had smoked cigarette within 30 days of the survey. A 2 stage sampling technique was used; 1 local government area (LGA) was selected through simple random sampling technique (balloting) from the 4 metropolitan LGAs in Sokoto metropolis. In the selected LGA, sites were out-of-school adolescents aggregate (such as the various motor parks, markets, busy roads etc.) were line listed, proportional allocation was used to determine the number of study participants to recruit from each site. Sample size of 223 was estimated using formula for estimating sample size for cross-sectional studies. Systematic sampling technique was used to recruit the respondents; 213 respondents consented giving a response rate of 95.5%. An interviewer administered questionnaire was used to obtain data from the respondents. The questionnaire comprised of three (3) sections; which assessed sociodemographic characteristics, knowledge of health hazards of cigarette smoking, cigarette smoking related practice of respondents. The data obtained was entered into and analysed using statistical package for social science (SPSS) version 21.0. Scoring and grading of responses on knowledge of health hazards of cigarette smoking was done, each correct knowledge response was scored 1 mark while zero was awarded to wrong answers and or no response. The respondents’ knowledge was graded as either good or poor. Scores of less than 50% and equal to or greater than 50% was adjudged poor and good knowledge respectively. At the end of the scoring, the mean knowledge scores of the respondents and also the proportion of the respondents with good and poor knowledge was determined. Inferential statistics was conducted, subsequently; binary logistic regression was performed to determine predictor of ever smoking cigarette. All tests were conducted using 2 tails and level of significance was set at 5%. Ethical approval for this study was obtained from the ethics review committee of Usmanu Danfodiyo University Teaching Hospital, Sokoto and permission to conduct the study was obtained from the Heads of adolescent aggregation areas like market places and motor parks. Verbal informed consent was obtained from individual respondents.
Results
Less than half 92 (43.2%) of the respondents were within the ages of 10 – 13 years. The mean age of the respondents was 14.7 ± 2.5 years. Majority 188 (88.3%) of the respondents were males, Muslim 208 (97.7%) Hausas 171 (80.3%). Majority 175 (82.2%) of the respondents had only Quranic education while only 3 (1.4%) had secondary school education. Almost 207 (97.2%) of the respondents were single while 4 (1.9%) of them were married. Almost half 92 (43.2%) of the respondents were begged for a living (Table 1).
Table 1 Socio demographic characteristics of respondents.
| Variables |
Frequency |
Percentage |
| |
n=213 |
(%) |
| Age Groups (in years) |
| Oct-13 |
92 |
43.2 |
| 14-16 |
74 |
34.7 |
| 17-19 |
47 |
22.1 |
| Mean±SD |
14.71±2.5 |
|
| Sex |
| Male |
188 |
88.3 |
| Female |
25 |
11.7 |
| Religion |
| Islam |
208 |
97.7 |
| Christianity |
5 |
2.3 |
| Ethnic Group |
| Hausa |
171 |
80.3 |
| Fulani |
24 |
11.3 |
| Yoruba |
6 |
2.8 |
| Highest Educational Status |
| None |
20 |
9.4 |
| Quranic |
175 |
82.2 |
| Primary |
15 |
7 |
| Secondary |
3 |
1.4 |
| Marital Status |
| Single |
207 |
97.2 |
| Married |
4 |
1.9 |
| Others |
2 |
0.9 |
| Occupational Status |
| Hawking |
37 |
17.4 |
| Apprenticeship |
11 |
5.2 |
| Car washing |
14 |
6.6 |
| Motor park attendant |
16 |
7.5 |
| Artisan |
6 |
2.8 |
| Food seller |
35 |
16.4 |
| Begging |
92 |
43.2 |
| Others |
2 |
0.9 |
| Mother’s educational status |
| None |
20 |
9.4 |
| Quranic |
183 |
85.9 |
| Primary |
3 |
1.4 |
| Secondary |
5 |
2.3 |
| Post-secondary |
2 |
0.9 |
| Father’s educational status |
| None |
11 |
5.2 |
| Quranic |
166 |
77.9 |
| Primary |
14 |
6.6 |
| Secondary |
13 |
6.1 |
| Post secondary |
2 |
0.9 |
Majority of the respondents knew that cigarette smoking could lead to lung cancer 176 (82.6%) and heart diseases 159 (74.6%). Less than half of the respondents knew that cigarette smoking could lead to PUD 115 (54.0%) and that pregnant women who smoke cigarette were likely to lose their pregnancy 114 (53.5%). Less than half 89 (41.8%) of the respondents knew that pregnant women who smoked cigarette may give birth to babies that is born with abnormal arms and legs. Majority of the respondents 172 (80.8%) knew that inhaling smoke from another person’s cigarette could lead to lung disease (Table 2).
Table 2 Cigarette smoking related knowledge of respondents.
| Variables |
Frequency |
Percentage |
| |
n=213 |
(%) |
| Can cigarette smoking lead to lung disease? |
|
|
| Correct response |
176 |
82.6 |
| In- correct response |
37 |
17.3 |
| Can cigarette smoking lead to heart disease? |
|
|
| Correct response |
159 |
74.6 |
| In- correct response |
54 |
25.4 |
| Can cigarette smoking lead to peptic ulcer disease? |
|
|
| Correct response |
115 |
54 |
| In- correct response |
98 |
46 |
| Can Smoking by a pregnant woman predispose that woman to losing her pregnancy? |
|
|
| Correct response |
114 |
53.5 |
| In- correct response |
99 |
46.4 |
| Can smoking by a pregnant woman predispose that woman to giving birth to a baby that is born with abnormal arms and legs? |
|
|
| Correct response |
89 |
41.8 |
| In- correct response |
124 |
58.2 |
| Can inhaling smoke from another person's cigarette lead to lung disease? |
|
|
| Correct response |
172 |
80.8 |
| In- correct response |
41 |
19.2 |
| Knowledge score |
|
|
| Poorknowledge |
44 |
20.7 |
| Good knowledge |
169 |
79.3 |
About a tenth of all respondents interviewed 24 (11.3%) had ever smoked cigarette, seven respondents (3.3%) were current cigarette smokers; however, almost half 101 (47.4%) of the respondents bought cigarette in the past 30 days. Almost a third of the respondents, 71 (31.0%) would allow cigarette smokers to smoke in their homes and majority of the respondents 147 (69.0%) would leave the place where people are smoking cigarette. Nine (4.2%) of the respondents smoked in the presence of non-smokers, although four (1.9%) of them had ever tried stopping to smoke out of which one (0.5%) of them succeeded. Seven (3.3%) respondents wish to stop smoking. Eleven (5.1%) of the respondents thought they would still smoke cigarette at any time during the next 12 months (Table 3). Most of the respondents 13 (61.9%) who reported cigarette smoking initiated this habit between the ages of 10 – 13 years (Figure 1).
Table 3 Cigarette smoking related practice of respondents.
| Variables |
Cigarette smoking related practice
(n=213) |
| |
Positive (%) |
Negative (%) |
| Have you ever smoked cigarette |
189 (88.7) |
24 (11.3) |
| Have you smoked cigarette in the past 30 days? |
206 (96.7) |
7 (3.3) |
| Have you bought cigarette in the past 30 days? |
112 (52.6) |
101 (47.4) |
| Do you allow cigarette smokers to smoke in your home? |
142 (69.0) |
71 (31.0) |
| If you go to a place where people are smoking cigarette, will you leave the place? |
147 (69.0) |
66 (31.0) |
| Do you smoke in the presences of none smokers? |
1 (0.5) |
9 (4.2) |
| Have you ever tried to stop smoking? |
4 (1.9) |
5 (2.3) |
| If ever, did you finally succeed? |
1 (0.5) |
4 (1.9) |
| Do you want to stop smoking now? |
7 (3.3) |
3 (1.4) |
| Do you think you will smoke cigarette at any time during the next 12 months? |
202 (94.9) |
11 (5.1) |
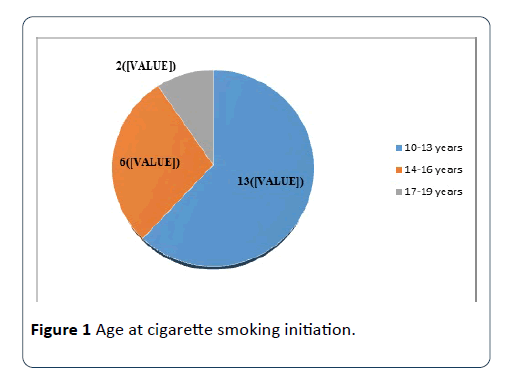
Figure 1: Age at cigarette smoking initiation.
Few of the respondents 5 (55.6%) smoke cigarette for more 10 days in a month, while 2 (22.2%) smoke for 6-10 days in a month (Figure 2). About a third of the respondents who smoke cigarette 3 (33.3%) smoke more than 10 sticks of cigarette per month, another 3 (33.3%) smoke 6-10 sticks of cigarette per month, while 1 (11.1%) of the respondents smoked 1 stick of cigarette in a month (Figure 3).
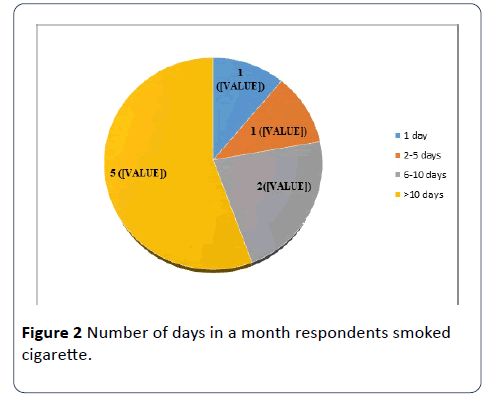
Figure 2: Number of days in a month respondents smoked cigarette.
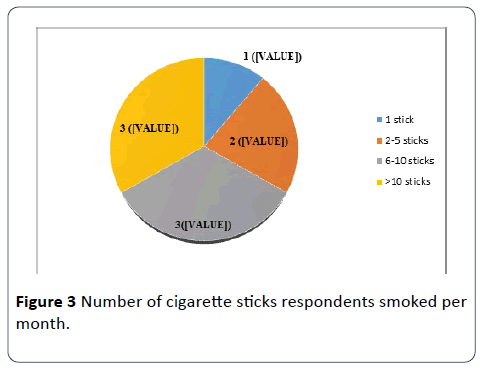
Figure 3: Number of cigarette sticks respondents smoked per month.
Almost all the respondents with no formal education had never smoked cigarette and this was statistically significant (X2=9.58, p=0.002, OR=0.203). Half, 12 (50%) of the respondents that had ever smoked were within the age range of 17 – 19 years and this was statistically significant (X2=17.55, p=<0.001). Respondents whose fathers smoked cigarette were 2.79 times more likely to have ever smoked cigarette and this was statistically significant (X2=5.66, P=0.017, OR=2.79). Likewise, respondents whose mothers smoked cigarette were 13.4 times more likely to have ever smoked and this was statistically significant (X2=7.68, p=0.006, OR=13.4).
Respondents who felt that cigarette should be sold to children <18 years were 8.93 time more likely to have ever smoked cigarette (X2 = 25.00, p ≤0.001, OR=8.93). Barely half, 11 (45.8%) of the respondents who had ever smoked felt that smokers do not have more friends that non- smokers (X2=7.616, p=0.022) and respondents who attested to the fact that smokers should be allowed to smoke in the public were 23.13 times more likely to have ever smoked (X2=39.04, p<0.001, OR=23.13) (Table 4).
Table 4 Determinants of respondents ever smoking cigarette.
| Variables |
Ever smoked cigarette |
Test of significance andp-value |
| |
Yes
n (%) |
No
n(%) |
|
| |
| Educational status |
| No formal |
18 (9.2) |
177 (90.8) |
X2=9.58 |
| Some formal |
6 (33.3) |
12 (66.7) |
p=0.002*, OR=0.203 |
| Age |
| Oct-13 |
2 (8.3) |
90
(47.6) |
X2=17.55 |
| 14-16 |
10 (41.7) |
64
(33.9) |
p=0.000** |
| 17-19 |
12 (50.0) |
35(18.5) |
|
| Father smokes cigarette |
| Yes |
11 (20.0) |
44
(80.0) |
X2=5.66, p=0.017*, OR=2.79 |
| No |
13 (8.2) |
145
(91.8) |
|
| Mother smokes cigarette |
| Yes |
3 (60.0)
2 (40.0) |
|
Fisher’s exact test = 7.68, |
| No |
21 (10.1) |
187 (89.9) |
p=0.006*, OR=13.36 |
| Bought cigarette in past 30 days |
| Yes |
13 (12.9) |
88(87.1) |
|
| No |
11 (9.8) |
101 (90.2) |
X2=0.494, p=0.482 |
| Cigarette should be sold to people <18 years |
| Yes |
10 (41.7) |
14 (58.3) |
X2=25.00,p=0.000**, |
| No |
14 (7.4) |
175 (92.6) |
OR=8.93 |
| Perception that smokers have more friends than non-smokers |
| Yes |
9 (37.5) |
28(14.8) |
LR=7.616, p=0.022* |
| No |
11 (45.8) |
137(72.5) |
| I don’t know |
4 (16.7) |
24(12.7) |
| Smokers should be allowed to smoke in public |
| Yes |
8 (66.7) |
4 (33.3) |
X2=39.04, p=0.000**, |
| No |
16 (8.0) |
185
(92.0) |
OR=23.13 |
| knowledge |
| poor |
4 (9.1)
(90.9) |
40 |
X2=0.263, p=0.608 |
| good |
20 (19.0)
(88.2) |
149 |
| |
|
|
|
*p <0.05; **p<0.001
Majority of respondents that currently smoke were within the age group of 17 – 19 years and this was statistically significant (X2=6.612, p=0.0317). Seventy five (97.4%) of respondents whose brothers smoked cigarette were less likely to have smoked within the past 30 days (X2=15.625, p ≤ 0.001, OR=0.059). Respondents who felt that cigarette should be sold to people less than 18 years were 69.17 times more likely to have smoked cigarette within the past 30 days (X2=29.86, p ≤ 0.001, OR=69.17). Four (57.1%) of the respondents who currently smoked cigarette felt that smokers had more friends than non-smokers (X2=16.27, p<0.001) and respondents who felt that smokers should be allowed to smoke in public were 213 times more likely to currently smoke cigarette (X2=41.9, p<0.001, OR=212.5) (Table 5).
Table 5 Determinants of current cigarette smoking behaviour of respondents.
| Variables |
Currently smoking cigarette |
Test of significance and |
| |
Yes n (%) |
No n (%) |
p-value |
| Educational status |
| No formal |
5 (6.0) |
79
(94.0) |
Fisher’s exact test = 1.196 |
| Some formal |
2 (22.2) |
7 (77.8) |
p=0.274 |
| Age |
| Oct-13 |
0 (0.0) |
32
(37.2) |
X2=6.612 |
| 14-16 |
2 (28.5) |
30 (34.9) |
p=0.0317* |
| 17-19 |
5 (71.4) |
24
(27.9) |
|
| Brother smokes |
| Yes |
2 (2.6) |
75
(97.4) |
X2=15. 625, p=0.000**, |
| No |
5 (31.3) |
11
(68.8) |
OR=0.059 |
| Father smokes cigarette |
| Yes |
2 (5.4) |
35 (94.6) |
X2=0.397, p=0.528, |
| No |
5 (8.9) |
51 (91.9) |
|
| Mother smokes cigarette |
| Yes |
0 (0.0) |
1
(100.0) |
Fisher’s exact test=0.000, |
| No |
7 (7.6) |
85 (92.4) |
p=1.000 |
| Bought cigarette in past 30 days |
| Yes |
6 (10.0) |
54 (90.0) |
X2=1.44, p=0.223 |
| No |
1 (3.0) |
32 (97.0) |
| Cigarette should be sold to people <18 years |
| Yes |
5 (62.5) |
3 (37.5) |
Fisher’s exact test=29.86, p=0.000**, |
| No |
2 (2.4) |
83
(97.6) |
OR=69.17 |
| Perception that smokers have more friends than non-smokers |
| Yes |
4 (57.1) |
9 (10.5) |
LR=16.27, p=0.000** |
| No |
1 (14.3) |
74(86.0) |
| I don’t know |
2 (28.6) |
3 (3.5) |
| Smokers should be allowed to smoke in public |
| Yes |
5 (83.3) |
1 (16.7) |
Fisher’s exact test=41.9, p=0.000**, |
| No |
2 (2.3) |
85
(97.7) |
OR=212.5 |
| knowledge |
| poor |
1 (5.0) |
19
(95.0) |
X2 =0.234, p=0.629, |
| good |
6 (8.2) |
67
(91.8) |
*p <0.05; **p<0.001
Respondents within the age group of 17 – 19 years were 9 times more likely to have ever smoked cigarette and this was statistically significant after controlling for the effects of respondents’ educational status, fathers’ and mothers’ smoking status, whether to smoke in the public, and perception that smokers have more friends than non-smokers (OR=9.0, p=0.013, 95% CI [0.019 - 0.632]). Respondents who belief that smokers should be allowed to smoke in public were 17 times more likely to have ever smoked cigarette and this was statistically significant after controlling for the effects of respondents’ educational status and age, fathers’ and mothers’ smoking status, and perception that smokers have more friends than non-smokers (OR=17.0, p=0.002, 95% CI [2.820 – 102.807]). Similarly, respondents whose mothers smoked cigarette were 18.4 times more likely to have ever smoked cigarette and this was statistically significant after controlling for the effects of respondents’ educational status and age, fathers’ and mothers’ smoking status, whether to smoke in the public and perception that smokers have more friends than non-smokers (OR=18.4, p=0.011, 95% CI [1.943 – 173.385]) (Table 6).
Table 6 Predictors of respondents ever smoking cigarette.
| Variables |
B (S.E) |
P Value |
OR |
95% CI for OR |
| |
|
|
|
Lower |
Upper |
| Respondents’ highest educational level |
-1.160 (0.733) |
0.113 |
0.313 |
0.075 |
1.317 |
| Perception that smokers have more friends than non-1smokers |
0.191 (0.712) |
0.789 |
1.21 |
0.3 |
4.887 |
| Cigarette should be sold to people less <18 year |
0.859 (0.757) |
0.257 |
2.361 |
0.535 |
10.413 |
| Belief that smokers should be allowed to smoke in public |
2.835 (0.917) |
0.002* |
17.026 |
2.82 |
102.807 |
| Father smoke cigarette |
0.713 (623) |
0.252 |
2.04 |
0.602 |
6.911 |
| Mother smoke cigarette |
2.910 (1.146) |
0.011* |
18.353 |
1.943 |
173.385 |
*p <.05
NB: The logistic regression for current smokers was not reported because it yielded an invalid result due to small sample (prevalence) of current smokers.
Discussion
Out-of-school adolescents are often neglected when planning for tobacco prevention programmes despite the fact that they are more vulnerable. Generally, adolescent is a period of identity forming and great pressure. As this period presents an opportunity for picking up bad habits, it also presents a golden opportunity for behaviour modification. Out-of-school adolescents are especially vulnerable to wrong information from sources that lack credibility [4]. Because they are outside a formal school system they also miss out of the opportunity for learning in conducive environments. It’s also surprising to note that there is a dearth of literature done among this cohort.
One-tenth of the respondents in this study have ever smoked cigarette. This is lower than 20.5% reported by Adebiyi in Oyo state, Southwestern Nigeria and much lower than 46% reported by Odukoya in Lagos state in the same region [4,6]. This finding is surprisingly similar to a prevalence of 10.6% among secondary school students in Oyo State, Nigeria [7] considering the fact that out-of-school adolescents often go through many stressful life events compared to their in-school counterparts. These events have been shown to be associated with increased risk for smoking and alcohol use [8].
The study further revealed the prevalence of current smokers among out-of-school adolescents to be a paltry of 3.3%. This suggests that about 8% had stopped smoking cigarette as at the time the study was done. It is surprisingly lower than 8.3% reported by Raji among school adolescent in Sokoto [9] and much lower than 11.6% and 32.5% reported from studies from southwestern Nigeria 4, 6 and among similarly vulnerable youth in more developed nations [10-12]. This finding may be due to information bias (underreporting) as some adolescent who smoke might not have revealed their smoking status even after being assured of their confidentiality.
Majority of the respondents in this study were light smokers, smoking six to over ten sticks of cigarette in a month. This is corroborated by findings done in the southwestern Nigeria by Ayo-Yusuf where majority of the adults were observed to be light smokers [13] and in other environments where youth were also more often light smokers [14-16]. This may be because they may not have the economic capacity to purchase many cigarettes [17] which is buttressed by the fact that almost half of the respondents in this study were beggars. However, it has been reported that being a ‘light’ smoker does not reduce potential for addiction [18].
Most of the respondents initiated cigarette smoke between the ages of 10-13 years. This contrast studies done in Sokoto North-west among school adolescents, 9 and Salawu in Borno, [19] North-east Nigeria were majority of smokers initiated smoking within the 15-19 years and 13-15 years respectively but consistent with 10-14 years reported in a study done by Adeyeye [20] in Lagos state, Southwestern Nigeria among senior secondary school students. These findings give cause for great concern because many youth-oriented tobacco prevention programs are targeted at youth within the formal school system often neglecting those out-of-schools, where environmental and personal factors may increase their vulnerability to tobacco use.
Many of the respondents were knowledgeable about some aspects of the health risks associated with tobacco use, despite their being outside of formal school settings. It is surprising that this did not translate into preventive practices, as we did not identify a significant relationship between knowledge and either ever smoked cigarette or current smokers. Hence youth tobacco prevention programs should go beyond the mere provision of knowledge and focus on other social and environmental factors that may promote tobacco use among youth.
The study reported no statistically significant association between respondents overall knowledge of cigarette smoking, whether they bought cigarette within the past 30 days and whether they have ever smoked or not. But it revealed that almost all the respondents with no formal education had never smoked cigarette and this was statistically significant. This contradicts findings from studies done among in-school adolescent that revealed that the academic performance of students was significantly associated with the smoking status of the students (smokers had poor academic performance than non-smokers) [21].
Half of the respondents that had ever smoked were within the age range of 17 – 19 years and this was statistically significant. This is not surprising since most of respondents that smoked were within the age group of 17 – 19 years.
Respondents whose fathers and mothers smoked cigarette were more likely to have ever smoked cigarette and this were statistically significant. This is concurred by findings among school adolescents in Sri Lanka and East Timor-Leste that revealed that peer and parental factors that include having peers or parents who smoked were significantly associated with a higher chance of the child being a smoker [22]. The association between having a parent who is a smoker and adolescent’s own smoking may be an indication of parental tolerance to smoking or easy availability, acceptability and accessibility of cigarettes within the home [23].
Respondents who felt that cigarette should be sold to children <18 years were more likely to have ever smoked cigarette and to have smoked cigarette within the past 30 days. This means that majority of the respondents that continued to smoke were within this age group.
The study reported no statistically significant association between respondents’ educational status, parents’ smoking status, buying cigarette in the past 30 days, overall knowledge of cigarette smoking and current cigarette smoking status. However, the study showed that majority of respondents that currently smoke were within the age group of 17 – 19 years and this was statistically significant having dominated the population that had ever smoked.
Over half of the respondents who currently smoked cigarette felt that smokers had more friends than nonsmokers, which may be due to the peer influence, they exert on others. Respondents who felt that smokers should be allowed to smoke in public were more likely to have smoked cigarette within the past 30 days buttressing the fact that they themselves smoke cigarette.
The result of multivariate analysis revealed that respondent’s late adolescents who believe that smokers should be allowed to smoke in public and respondents whose mothers smoke cigarette were key predictors of cigarette smoking behaviors of respondents (ever smoked). This finding is consistent with a study by Olumide et al. that reported that age was a predictor of cigarette (and alcohol) use in Baltimore with older adolescents being more likely to be using these substances. It is possible, therefore, that given the low-income status of most study respondents; older adolescents may be more responsible for assisting with earning income for the family. As a result, increased age and financial stresses may be contributing to substance use in this population, as shown in previous studies of adolescents [24].
With regard parental influences on adolescents’ smoking habits, the finding in this study concurred with a study among in-school adolescents that revealed students whose family members were tobacco users had higher risk of tobacco use relative to those with no family members using tobacco [25-28]. It is apparent from this study that good knowledge alone may not result in positive smoking behavior. There need to be other interventions that include supportive environment, strong policy support and community participation. It is highly imperative to educate parents that their children are more likely to smoke if they also smoke. This, in addition with public policies against smoking, will discourage parents from smoking. Perhaps, interventions to reduce and prevent cigarette smoking among adolescents should target adolescents early and focus on keeping them in school during their adolescent years. Poverty could account for the reason why most adolescent are out-of-school leading them to be involved in smoking and perhaps other deviant social vices. The government needs to play a key role in rendering to this cohort free education or skill acquisition and other vocational training programmes for them to be able to earn a living.
Conclusion
The study was carried out among adolescents, which is a life changing and life shaping time in anybody’s life, 11.3% had ever smoked cigarette and 3.3% were current cigarette smokers. Most had good knowledge of health hazards of cigarette smoking. Main predictor of respondents ever smoking was the perception that people should be allowed to smoke in public. Sustained campaigns targeting out-of-school adolescents may go a long way in reducing cigarette use among these groups of adolescents.
19566
References
- Can G, Topbas M, Oztuna F, Ozgun S, Can E (2009) Factors contributing to regular smoking in adolescents in Turkey. J School Health 79:93-97.
- Adebiyi AO, Faseru B, Sangowawa AO, Owoaje ET (2010) Tobacco use amongst out of school adolescents in a local Government area in Nigeria. Subst Abuse Treat Prev Policy. 5: 24.
- Odukoya OO, Dada MR, Olubodun T, Igwilo UA, Ayo-Yusuf OA (2016) Risk perception and correlates of tobacco use among young people outside of formal school settings in lagosstate, Nigeria. Asian Pac J Cancer Prev17:2833-2839.
- Yisa I, Lawoyin T, Fatiregun A, Emelumadu O (2009) Pattern of substance use among senior students of command secondary schools in Ibadan, Nigeria. Niger J Med 18:98-102.
- Simantov E, Schoen C, KleinJ (2000) Health - compromising behaviours: why do adolescents smoke or drink. Arch PediatrAdolesc Med 154:1025-1033.
- Raji MO, Abubakar IS, Oche MO, Kaoje AU (2013) Prevalence oadeterminants of cigarette smoking among in school adolescents in sokoto metropolis, North West Nigeria. International J TropMed 8:81-86.
- Embleton L, Mwang A, Vreeman R (2013)The epidemiology of substance use among street children in resource-constrained settings: a systematic review and meta- analysis Addict. Addiction 108:1722-1733.
- Tucker J, Shadel W, Golinelli D (2014) Alternative tobacco product use and smoking cessation among homeless youth in Los Angeles County. Nicotine Tob Res 16:1522-1526.
- Tucker J, Shadel W, Golinelli D (2015) Sniping and other high-risk smoking practices among homeless youth. Drug Alcohol Depend 154:105-110.
- Ayo-Yusuf O, Odukoya O, Olutola B (2014) Sociodemographic correlates of exclusive and concurrent use of smokeless and smoked tobacco products among Nigerian men. Nicotine Tobacco Res 16:641-646.
- Fawibe A, Shittu A (2011) Prevalence and characteristics of cigarette smokers among undergraduates of the University of Ilorin, Nigeria. Niger J ClinPract 14:201-205.
- Odukoya O, Odeyemi K, Oyeyemi A (2013) Determinants of smoking initiation and susceptibility to future smoking among school-going adolescents in Lagos state, Nigeria. Asian Pac J Cancer Prev 14:1747-1753.
- Global youth tobacco survey collaborative group (2002) Tobacco use among youth: a cross country comparison. Tob Control11:252.
- World Health Organisationtobacco free initiative (2004) Tobacco and poverty: a vicious circle.
- DiFranza J (2009) Tobacco dependence in light smokers. Nicotine Tob Res 11:1122-1123.
- Salawu FK, Danburam A, Desalu OO, Olokoba AB, Agbo J, et al. (2009) Cigarette smoking habits among adolescents in Noertheast Nigeria. Mera: Afr J Respir Med.
- Adeyeye OO (2011) Cigarette smoking habits among senior secondary students in Lagos, Southwest Nigeria. Int J Med Res 2: 1047-1050.
- Al-Naggar RA, Jawad AA, Bobryshev YV (2012) Prevalence of cigarette smoking and associated factors among secondary school teachers in malaysia. Asian Pacific J Cancer Prev13:5539-5543.
- Katulanda P, Liyanage IK, Wickramasinghe K, Piyadigama I, Karunathilake IM, et al. (2015) Tobacco smoking among school children in colombo district, Sri Lanka. Asia Pac J Public Health 27: 2.
- Sizita S, Muula AS, Rudatsikira E (2008) Prevalence and correlates of current cigarette smoking among adolescents in east timor-leste. Indian Pediatrics.
- Olumide AO, Robinson AC, Levy PA, Mashimbye L, Brahmbhatt H, et al. (2014) Predictors of substance use among vulnerable adolescents in five cities: Findings from the Well-being of Adolescents in vulnerable environments study. J Adolesc Health 55: 60.
- Bhaskar RK, Sah MN, Gaurav K, Bhaskar SC, Singh R, et al. Prevalence and correlates of tobacco use among adolescents in the schools of Kalaiya, Nepal: a cross-sectional questionnaire based study. Tobacco Induced Diseases 14: 11.
- Pradhan P, Niraula S, Ghimire A (2013) Tobacco use and associated factors among adolescent students in Dharan, Eastern Nepal: a cross- sectional questionnaire survey. BMJ.
- Dereje N, Abazinab S, Girma A,Dereje N, Abazinab S, et al. (2014) Prevalence and predictors of cigarette smoking among adolescents of Ethiopia: school based cross-sectional study.J Child AdolescBehav3: 1.
- Kasiulevicius V, Sapkota V, Filipaviciute R,Kasiulevicius V, Sapkota V, et al. (2006) Sample size calculation in epidemiological studies.Gerontologija 7:225-231.

