Keywords
Haemodialysis, concerns, chronic renal failure, quality of life, psychosocial disorders, psychological factors.
Introduction
Chronic Renal Failure (CRF) is an irreversible and progressive kidney failure, [1] where haemodialysis has been proved to be the most effective treatment modality, as it results in long survival rates and maintains patients’ life at a satisfactory level [2].
However, this treatment has a number of restrictions and modifications, which have a detrimental impact on the quality of patient’s life. More specifically, haemodialysis affects the professional and psychological well- being of these patients and their social and economic status, resulting in a large number of psychological disorders [3-13].
Allied to these areas of difficulty, in combination with the high prevalence of Chronic Renal Failure, there is a necessity for identification of the psychological concerns of patients undergoing haemodialysis [14,15].
Concerns of patients on dialysis
The most frequently reported psychological concerns of people undergoing haemodialysis are food and fluid restrictions, changes in marital role, financial concerns, changes in social and marital relationships, frequent hospitalisations, limitations in vacations, limitations in leisure activities, increased dependency on the artificial kidney machine, the medical staff and family environment, uncertainty about the future, sleep disturbances, physical fatigue, sexual problems, limitation in physical activities, unemployment and changes in body appearance [6,11,16-24].
Patients’ psychological condition is affected by the social and family support they receive. Patients with chronic disease, in their efforts to develop defence mechanisms, exhibit psychiatric disorders, refusal of treatment and disruption of interpersonal and family relationships [13,25].
Moreover, the psychosocial adjustment of patients to a program of periodic dialysis treatment is influenced positively or negatively by the personality of each patient, in combination with the support they receive by health professionals, their family and social environment. These patients exhibit personality disorders, such as alexithymia, neuroticism, introversion and psychotism [13,14].
It should be noted that depression is the most common psychological complication of haemodialysis, which has a negative impact on the quality of patients’ life and their caregivers, affecting negatively their social, economic and psychological well-being [26]. Depression includes high annual mortality, [27,28] frequency of hospitalization, reduced compliance to medications and decreased quality of life [29].
Compared to healthy people, patients with chronic kidney disease face many difficulties in participating in various fields of life, such as paid work, sports and social activities [30]. This has a negative impact on feelings of autonomy and self-esteem, due to reduced patients’ self -worth and their psychological mood [31,32].
Moreover, many patients on haemodialysis have anaemia which is the most common complication of the above therapy [33]. Anaemia occurs as fatigue or depression and affects negatively the quality of these patients’ life, [25,34] since it is responsible for the inadequate physical rehabilitation of patients [35].
Additionally, pain is the most common symptom of these patients which has a negative impact on the quality of their life. Pain is caused by multiple factors, such as the process of dialysis itself (i.e venipuncture, muscle cramps, headaches) or accompanying systemic diseases and painful syndromes [36].
It should be noted that patient’s compliance with the treatment process is very important, since it affects the prognosis of the disease and the quality of life of patients under chronic dialysis [37]. Reduced compliance can be caused by psychosocial factors (i.e poverty, long periodic dialysis, immigration, family dysfunction, frequent hospitalizations of patients and lifelong medication), [38,39] while it is associated with increased mortality [6,13].
A substantial number of patients on dialysis are troubled by the fact that they have poor nutrition, which is a major factor of poor quality of life because it increases the rate of morbidity and mortality [40]. Weight loss causes fatigue, discomfort and exhaustion to these patients and creates increased predisposition to infections, because of the reduced stocks of body proteins and fat [3].
Furthermore, sleep disorders are reported as a very common problem for patients on dialysis. The most common psychosocial concerns are the depression, the educational level, the employment and marital status, [41] the dependence of patients on the artificial kidney machine, the medical and nursing staff and their family and the loss of control of their physical function [42].
Moreover, sexual dysfunction is a frequent, common and multifactorial problem in patients with Chronic Renal Failure [43,44]. Sexual disorders significantly affect the quality of life of men and their partners, while they have a negative impact not only on their self esteem but also on their interpersonal relationships [43,45].
It has been asserted that physical activity improves the quality of life of patients on dialysis, provided that it is progressive and individualized according to patient's limitations (type of exercise, frequency, timing, intensity of exercise) and their pathophysiological condition [40,46].
Aim
The aim of this study was to investigate the psychological impact of dialysis on the quality of life of patients with End Stage Renal Failure.
Material and Method
Study sample
Following ethical approval and the appropriate license from hospitals in order to conduct the study, a total of 100 people undergoing chronic periodic hemodialysis in four hospitals in Athens (three in public sector and one in private sector) were invited to participate in the study. All potential participants were informed that their participation was completely voluntary and confidentiality was assured. Of the 103 patients, a consent form was obtained from the 100 patients who agreed to participate in the study.
To meet the inclusion criteria for participation, subjects needed to:
1. Be receiving chronic haemodialysis treatment
2. Be 20 years or older of either gender
3. Have no psychiatric disorders
4. Be able to speak, read, and write Greek.
5. Have a satisfactory level of cooperation and perceptual ability.
Data collection
The present research study was based on a combination of data from primary research and secondary sources of information. Primary data came from patients undergoing periodic haemodialysis, by completing a questionnaire which assessed the quality of their life. Secondary sources of information were published studies of international and Greek literature, the annual report of atlas of United States Renal Data System (USRDS), the data collection from global research and epidemiology through the National Centre for Documentation and a systematic review of data through electronic databases MEDLINE, CINAHL, SCOPUS, PUBMED and IATROTEK.
A questionnaire combining qualitative and quantitative approaches was utilised for the collection of data. The instrument was composed of two sections, the first of which concerned demographic information about each respondent. It included 11 questions (gender, marital status, level of academic education, time, length of time on dialysis, working status, age and current economic situation)
The second section was based on the KDQOL-SF questionnaire and was part of the health survey SF-36, which was the core of the questionnaire. The questionnaire used in the present study was slightly modified and adapted for the purposes of this study. It covered the quality of life through the dimensions of health and the specialized tool in nephropathy KDQOL-SF TM 1.3, (Greek version 1.2). It included 24 questions, which were categorized into eight topics (general health, physical functioning, physical role, bodily pain, vitality, social functioning, emotional role, mental health). The final questionnaire consisted of 35 questions.
In the main study, patients were asked to rate the extent they were troubled by each one of the psychological concerns on a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree), where higher numbers indicated greater severity of the impact of each factor on these patients.
Procedure
During their routine treatment, each participant was provided with a covering letter, a questionnaire and an envelope for returning the questionnaire after completing it.
Patients were first asked to tick (X) the answers regarding the demographic data and then to rate the extent to which they were troubled by each of the psychological concerns, by ticking the appropriate number from 1 to 5 provided below each question.
Description of Research Tool
The Greek SF-36 Health Survey is a general widespread tool, which is used in research in general population surveys, in the evaluation of health policies and in clinical practice in order to determine the psychometric properties during the comparison of health status between different population groups, different patients and healthy of different categories or between different therapeutic methods of a group of patients [47]. The widespread use of the SF-36 in studies about the Quality of Life of the general population or patient groups makes it a reliable instrument, which has a very good reliability and validity. The statistical tests of validity and reliability of the Greek SF-36 Health Survey, which were made on a representative sample of Greek urban population by Pappa et al., [48] had positive results.
Additionally, a study conducted by Kododimopoulos and Niakas concerning the use of KDQOL-SFTM for measuring health-related quality of life in Greek patients under hemodialysis, confirmed the validity and reliability of the Greek translation of the questionnaire Kidney Disease Quality Of Life Short Form (KDQOL-SFTM) [49].
Data Analysis
Quantitative data were analysed using SPSS-V17 (Statistical Package for Social Sciences-Version 17). Descriptive statistics, frequencies, tables, and graphs were used to present the results of the study.
Results
Demographic data
The overall response rate was 100, with 69 males and 31 females. The majority of the participants (69%) were between 50 and 59 years old. Sixty six (66%) patients were married, 14 (14%) were single, 8 (8%) were divorced, and 12 (12%) were widowed (Figure 1).
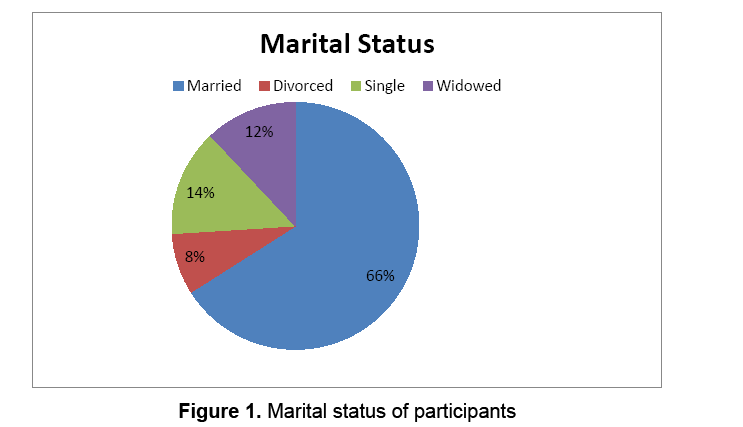
Figure 1: Marital status of participants
Regarding the level of academic education, 30 (30%) of the patients had finished primary school, 25 (25%) secondary and 22 (22%) high school. Moreover, 23 (23%) had a third level of education with 1 (1%) participant having completed a doctoral degree and another 1 (1%) participant having completed a master degree (Figure 2). The Greek educational system consists of primary, secondary and high school, third level and postgraduate education, each lasting 6, 3, 3, 2 to 5, and 1 to 3 years respectively.
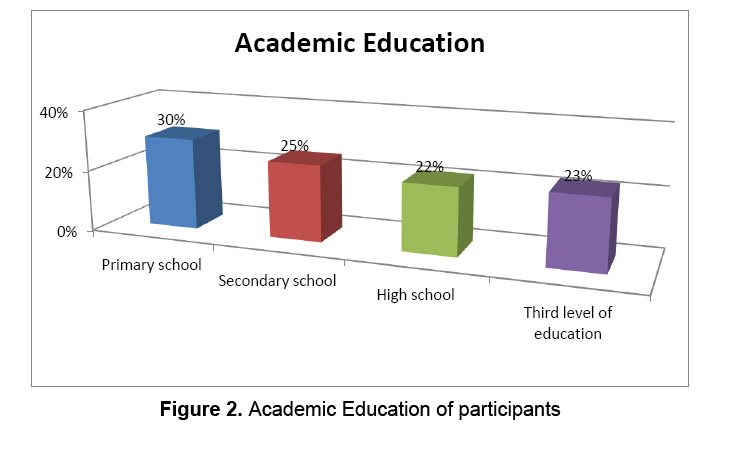
Figure 2: Academic Education of participants
Also, the majority of the participants 44 (44%) had been receiving dialysis for one to three years, while 28 (28%) four to eight years, 14 (14%) over eight years and 14 (14%) less than one year (Figure 3). Finally, 95 (95%) patients had to receive dialysis three times a week, each session lasting for four hours.
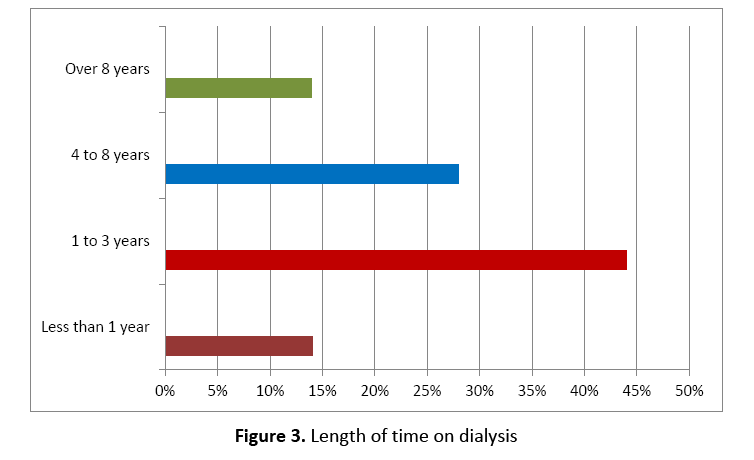
Figure 3: Length of time on dialysis
Health status of participants
1. Physical Role
In this study, 53.8% (n=50) of the participants reduced the time they used to spend on work and other activities after the beginning of haemodialysis while 51.6% (n=49) had difficulty in performing their work or other usual activities.
2. Physical Functioning
The majority of the participants (29.9% (n=29) reported that their health condition did not allow them to do any strenuous activities or activities of a moderate intensity. Fifty nine respondents (62.8%) performed less activities than they would like, while 52.6% (n=50) did their work or other activities more carefully than they usually did.
3. Social Functioning
Physical health and emotional problems affected social relationships and activities for 21.6% (n=21) and 12.4% (n=12) of the participants respectively.
4. Body Pain
Regarding physical pain in the last 4 weeks, only a percentage 12% (n=12) of the participants reported severe pain, while 7% (n=7) referred very severe bodily pain. Additionally, 20.4% (n=20) of the respondents reported that the pain affected enough their usual work.
5. Mental Health- Vitality
Regarding mental health status, 37.5% (n=36) of the respondents answered that few times they used to behave with frustration and irritability to people around them. Additionally, 43.8% (n=42) answered that few times they used to feel calm and serenity, while 31.9% (n=30) many times felt energy. Also, 35.4% (n=34) of the participants answered that few times they felt depressed, while 41.1% (n=39) referred that few times they felt happy. Finally, 41.8% (n=41) of the patients stated that many times they felt tired.
6. Effects of renal disease
The largest percentage of the respondents 41.7% (n=40) agreed that renal failure affected negatively the quality of their life, while 45.3% (n=43) used to spend too much time trying to cope with nephropathy. Finally, 46.9% (n=45) of the participants were often feeling frustrated and angry with their renal insufficiency, while 36.7% (n=36) of them were feeling burden on their family.
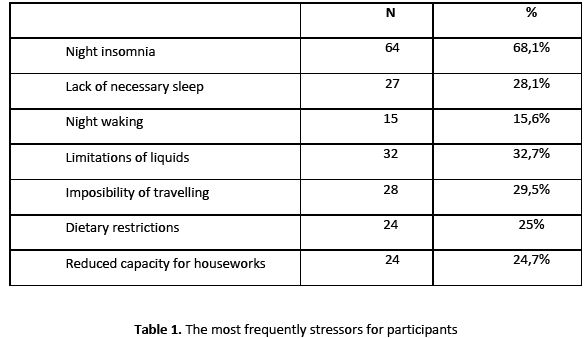
7. Stressors
The most frequently experienced stressors affecting patients’ daily lives were sleep disorders and especially problems with insomnia at night, the limitations in fluids, the impossibility of travelling, the lack of necessary sleep, dietary restrictions, the reduced capacity for houseworks, and night waking (Table 1).
However, the least stressful factors for the participants were their sexual life, their body and their dependence on medical and nursing staff (Table 2).

8. Symptoms of renal disease
Regarding the symptoms of kidney failure in the past 4 weeks, muscle pain, dizziness, lack of appetite, numbness of hands, nausea or stomach upsets and their problems in puncture site caused no discomfort to the participants. (Table 3)
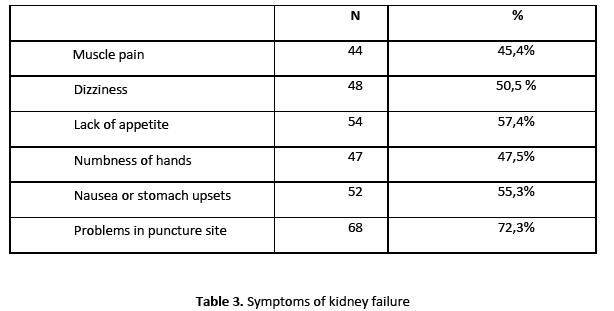
On the other hand, 25.8% (n=25) and 20% (n=19) of the participants had moderate irritation due to muscle cramps and itching respectively.
Discussion
The analysis of the KDQOL-SF scale showed that 41.7% of the participants perceived renal failure as a heavy burden in their life and they believed that nephropathy affected negatively their lives. This follows from the fact that 46.9% of the respondents were feeling frustrated, while 27.4% were often feeling irritated trying to cope with their disease and 45.3% used to spend a lot of time on each dialysis session.
In a research study conducted by Ekonomidou et al, [50] concerning depression in patients with CRF, 60% of the participants were feeling frustrated, since they were not as functional as they were before the initiation of dialysis.
According to a study conducted by Gerogianni, [11] the time spent on dialysis was among the five highest rated stressors for the participants. This is because most of the patients receive haemodialysis three times a week and the majority of them spend four hours for each dialysis session. This adds up to approximately 12 hours a week for dialysis, which is a significant amount of time for these patients.
Additionally, in this study, renal failure had a negative impact on the quality of patients’ life, affecting their mental health, their physical function, as well as their personal and family life. Many patients usually leave their job, their family or their home due to long-term treatment because they have to be near to the dialysis centre or they may be hospitalized for some days. Concerning their interpersonal relationships, these patients are combative, anxious and nervous to their carers and to the staff who provide them with the appropriate care. 1, 51, 52
Concerning anxiety due to their kidney failure, a large percentage of patients (50.5%) (n=48) had moderate to too much anxiety. The most frequent causes of stress are the fear of imminent death and the uncertainty about the future, [53] as well as their fear of the possibility that their arteriovenous fistula will become non-functional [54]. Additionally, a significant stressor for patients on dialysis is the possibility of getting infected, the complications of the disease and their physical health [1].
Physical Functioning
Concerning physical functionality of the participants, men had higher scores (higher levels of quality of life) compared to women who proved statistically significant (p <0.05) for those aged under 75 years. Due to their physical health, most of the participants are forced to reduce the time spent on routine activities, to perform fewer activities than they would like and to perform their activities less carefully. The impairment of physical strength is also caused by the physical pain experienced in each dialysis session and the day after dialysis.
Body pain
The results of the present study showed that 38% the participants did not experience any physical pain, while 27% of them experienced moderate bodily pain. This shows that physical pain does not have any significant effect on the quality of their life, while the reduction of pain may be due to the use of puncture materials of advanced technology and the specialization of health professionals in pain treatment. These findings contrast with those of a previous study, where pain was the most frequent symptom, which caused significant disorders in the quality of life and emotional, social and economic disruptions to patients receiving dialysis [36].
Symptoms of the disease
It should be noted that patients receiving dialysis do not usually have muscle pain, cramps, dizziness, lack of appetite, numbness of hands, nausea, stomach upsets and problems with venipuncture. As a result of this, the above symptoms do not usually cause stress to these patients. This may be due to the adequacy of dialysis which is achieved by all technological and medical advances in the field of dialysis, as well as patients’ compliance with the appropriate diet which needs to be low in phosphorus [11].
Regarding the symptoms of the disease, women of all ages, with the exception of the age of over 75 years, showed higher scores on the symptoms of the disease, compared to men of the same ages. Women of young age experience more intense symptoms of kidney failure compared to men. This may be happen because they are in the process of adjustment to the replacement therapy and relates to the psychological condition of women, the restriction in social activities and their difficulty in accepting their condition [40].
Stressors
Regarding the restrictions of ESRD, fluid and food restriction is a major source of stress for these patients. The results of the present study agree with those of a previous research study, where fluid and food restrictions were the most stressful factors for the participants [11]. It should be stressed that compliance with fluid restriction is particularly difficult during hot periods of the year, when patients have an increased thirst [55].
Among the most common stressors for the participants in this study was the inability to go on holiday, which is consistent with the results of other studies [6,11,18-22]. Many of the participants reported that they had difficulty in accessing other dialysis units during summer months, which prevented them from going on holiday to places they would like. According to Gabriel, [55] during summer months dialysis units accept a limited number of patients because of the reduced staff due to summer permissions. However, patients on dialysis have multiple additional problems that do not allow them to go on holiday [22]. This, makes them feel depressed and nervous towards their family, social and friendly environment.
Also, the majority of the participants had a reduced capacity for work in this study, which bothered them a lot. A previous research study conducted by Kaitelidou et al, [23] had the same results, where 39.4 % of the respondents reported that the disease prevented them from being able to work. According to Levy, [56] the reduced capacity for work leads to intense anxiety and sexual problems, since work affects positively the psychological status and libido of spouses. Additionally, unemployment is associated with physical and psychological problems of patients, such as anxiety, depression, sexual dysfunction and loss of self-esteem [9]. At the same time, the reduced ability to work leads to social and financial changes in patients’ lives, with the loss of income and deterioration of their living [51].
Regarding the dependence of patients on medical and nursing staff, the majority of the respondents in this study did not feel dependent on the staff of dialysis unit (49%). However, in a previous study, patients undergoing peritoneal dialysis were depended on health professionals [18]. This is because patients on dialysis depend on the medical instructions they have to follow, as well as the training about their treatment that the Nephrology Nurse will provide them [18].
Concerning their sexual life, the majority of the respondents (59.8%, n=58) did not report any discomfort in their sexual life. According to previous studies, sexual dysfunction was a frequent, common and multifactorial problem for patients with ESRD, since 50% of men and 55% of women undergoing hemodialysis reported difficulty in achieving orgasm and sexual dysfunction [43,44].
The results of this study disagree with those of previous studies, which reflect a better quality in their sex life. This may happen because the largest percentage of the sample in the present study is over 55 years old and is not in the reproductive age where the sexual desire is developed. Additionally, the low percentage of people who have no discomfort in their sexual life is probably due to the fact that the male population does not accept any reduction in their sexuality, even if they suffer from depression, stopping of urination and mood swings.
In the present study, body appearance did not bother the study population (57.7%, n=56). However, in previous studies, body appearance was one of the most stressful factors for people on dialysis. It should be noted that any change in body image after the initiation of dialysis (weight loss, muscle wasting, change of skin colour, apparent signs of venous puncture) is a stressor which has a negative affect on sexual mood of patients [11,24]. In the present study, body appearance is not a significant stressor for the participants. This may happened because the majority of the participants were chronically ill and they had possibly accepted their body image.
Regarding the level of academic education, 30 (30%) of the patients had finished primary school, 25 (25%) secondary and 22 (22%) high school. Moreover, 23 (23%) had a third level of education. The results of this study show that the relationship between the level of academic education and the quality of life is statistically significant. More specifically, people with higher level of academic education have higher level of quality of life (p <0.05). This is because people with higher level of academic education may have quality in their daily life, good health, good job, participation in leisure activities and a comfortable standard of living that gives them satisfaction and wellness [57].
The appropriate training of patients before the initiation of dialysis helps them to choose effectively the treatment modality of renal replacement therapy they will follow. Additionally, it helps patients to continue to work after the initiation of dialysis. Moreover, health professionals with the appropriate training have the ability to effectively inform patients in order to delay disease progression and prevent any other multiple additional problems [58].
In the present study, psychological disorders affected the participants at a large extent. The results of this study showed that a large proportion of the participants had lost their calm, had fatigue, frustration and intense anxiety about the future, while they used to feel unhappy and irritable. Additionally, a large percentage of the respondents were suffering from sleep disorders. More specifically, they used to wake up a lot of times during the night due to insomnia, while most of them remained awake during the day.
It should be noted that findings of the present study are consistent with those of similar studies, showing that patients with renal failure and especially old patients, have low levels of physical well-being and high levels of depression, poor sleep quality and appearance of various psychosocial factors [4,41,42,50,59].
Moreover, extensive randomized studies have shown that patients with uraemia under periodic hemodialysis exhibit reduction in indicators of brain function compared to indicators prior the initiation of dialysis [60]. The results of this study agree with previous studies, indicating that the brain function and the ability of attention and concentration seems to get improved after the initiation of periodic dialysis. This may happen because electrolyte disturbances due to chronic disease get improved after dialysis [61-64].
Limitations of the present study
In the present research study the results cannot be generalized to the entire number of patients with kidney disease because the participants were constituted a small clinical sample. Another limitation of this study is the fact that there may not be a confidence in self-reports of patients about their problems and especially their economic and psychological problems. For this reason, there is a necessity for further investigation of the research theme at a larger sample of patients with chronic renal failure.
Conclusions
The influence of symptoms of ESRD on patients’ quality of life, the frequency of periodic dialysis, the compliance of patients with treatment regimen and the negative effects of the disease on patients are the strongest dependency rates, which affect significantly the physical and psychosocial dimension of health. The process of dialysis itself, the education, the age and the gender seem to affect patients’ ability to work and the psychosocial health disorders, which affect negatively their health-related quality of life.
The literature is referred to the importance and the necessity of socialization, education and psychological support of patients, their families and their caregivers, according to the needs of patients. At the same time, there is a need of reassessment of the whole therapeutic and supportive strategy to the best possible social and psychological support of patients undergoing haemodialysis.
Psychosocial nursing interventions (assessment, encouragement and support) would be better to begin at diagnosis and should be adapted to the progress of the disease and focus on the physical, psychological and social functioning of people in order to facilitate the adaptation of patients to the changes of the disease. Consequently, the role of health professionals is to encourage patients to accept the limitations of the disease and its treatment, and to enable them to undertake their self-care with responsibility.
Moreover, the promotion of health programs concerning patients with Chronic Renal Failure should enhance their confidence and focus on mental health issues that concern them (i.e depression, anxiety and suicide ideation). At the same time, counseling programs would be very useful for the staff of dialysis units, since they would raise their awareness and promote their biopsychosocial approach towards patients.
2632
References
- Papadakis E. Approach of patients with kidney disease and patients with beta-thalassemia in a general hospital in Crete and investigation of their quality of life. Thesis, 2010; available at website: https://mph.med.uoc.gr/files/Dissertations/Papadakis%20Evag_2010.pdf (19/05/12).
- Ran KJ and Hyde C. Nephrology nursing practice: more than technical expertise. European Dialysis and Transplant Nurses Association/ European Renal Care Association Journal 1999; 35 (4): 4-7.
- Theofilou P. Psychiatric disorders in chronic periodic hemodialysis. Vima of Asklepius 2010; 9 (4): 420-440.
- Moschopoulou E, Savvidaki E. Psychosocial image of patients in chronic dialysis program-Approach - Intervention. Dialysis Living 2003; 7: 14-18.
- Yang JY, Huang JW, Peng YS, Chiang SS, Yang CS, Yang CC, Chen HW, Wu MS, Wu KD, Tsai TJ, Chen WY. Quality of sleep and psychological factors for patients undergoing peritoneal dialysis. Perit Dial Int 2007; 27 (6): 675-680.
- Cukor D, Scott D, Cohen Rolf A, Peterson, Kimmel P. Psychosocial Aspects of Chronic Disease: ESRD as a Paradigmatic Illness. J Am Soc Nephrol 2007; 18: 3042–305.
- Shil LC, Honey M. The impact of dialysis on rurally based Maori and their whatau /families. Nurs Prax N.Z 2011; 27 (2): 4-15.
- Neri L, Gallieni M, Cozzolino M, Rocca – Rey L, Brambilla G, Colombi A, Foa V, Branccaccio D. Work ability and health status in dialysis patients. Int J Artif Organs 2005; 28 (6): 554-556.
- Îœuehrer JR, Schatell D, Witten B, Gangnon R, Becker NB, Hofmann M. Factors affecting employment at initiation of dialysis. Clin J Am Soc Nephrol 2011; 6: 489-496.
- Lew-Starowicz, Gellert, R. The sexuality and quality of life of hemodialyzed patients – ASED multicenter study. J Sex Med 2009; 6 (4): 1062-1071.
- Gerogianni KG. Stressors of patients undergoing chronic hemodialysis. Nursing 2003; 42 (2): 228-246.
- Kaitelidou D, Ziroyannis PN, Maniadakis N, Liaropoulos LL. Economic evaluation of haemodialysis: implications for technology assessment in Greece. Int J Technol Assess Health Care 2005; 21(1): 40-46.
- Gerogianni KS, Babatsikou PF. Psychological aspects in chronic renal failure. Health Science Journal 2014; 8 (2): 205-214.
- Koutsopoulou - Sofikiti EB, Kelesi - Stavropoulou NM, Vlachou DE, Fasoi - Barka GG. The long-term consequences of chronic renal failure in the quality of life of uremic patients. The step of Asclepius 2009; 8 (3): 41-60.
- Koutsopoulou - Sofikiti EB Kelesi - Stavropoulou NM, Vlachou DE., Fasoi – Barka. Personality of patients with chronic renal failure. Vima of Asklipiou 2009; 8 (3): 240-254.
- Leung KCD. Psychosocial aspects in renal patients. Perit Dial Int 2003; 23(S2): S90-S94.
- Gerogianni KG, Babatsikou PF. Identification of stress in chronic haemodialysis. Health Science Journal 2013; 7 (2): 169-176.
- Theofilou P. Quality of life in end - stage renal disease: a qualitative analysis. Interscientific health care 2011; 3 (2): 70-80.
- Horsburgh ME, Rice VH, Matuk L. Sense of coherence and life satisfaction: Patient and spousal adaptation to home dialysis. American Nephrology Nurses' Association Journal 1998; 25 (2): 219-228.
- Triantaphillopoulou E, Iphou A, Arvaniti P, Michalopoulos D, Nousis T, Tserkezis G, Velissari E, Iphos C. Psychological nursing support for elderly patients undergoing chronic regular haemodialysis. European Dialysis and Transplant Nurses Association/ European Renal Care Association Journal 1998; 1: 29-31.
- Dingwall RR. Living with renal failure: the psychological issues. European Dialysis and Transplant Nurses Association/ European Renal Care Association Journal 1997; 4: 28-30, 35.
- Lacroix A, Jacquemet S, Assal JP. Patients' experiences with their disease: learning from the differences and sharing the common problems. Patient Education and Counseling 1995; 26: 301-312.
- Kaitelidou D, Liaropoulos L, Siskou O, Mamas T, Zirogiannis P, Maniadakis N, Papakonstantinou V, Prezerakos P. The social and economic consequences of dialysis in patients' lives with chronic renal insufficiency. Nursing 2007; 46 (2): 246-255.
- Ormandy P. Dialysis (part 2): haemodialysis. Nursing Standard 1997; 11 (23): 48-56.
- Spiridi S, Iakovakis A, Kaprinis G. Renal insufficiency: Biological and psychosocial consequences. Psychiatry 2008; 19: 28-34.
- Anees M, Hameed F, Mumtaz A, Ibrahim M, Nasir Saeed Khan M. Dialysis – related factors affecting quality of life in patients on hemodialysis. Iran Journal of Kidney Diseases 2011; 5 (1): 9-14.
- Hedayati SS, Bosworth HB, Briley LP, Sloane RJ, Pieper CF, Kimmel PL, et al. Death or hospitalization of patients on chronic hemodialysis is associated with a physician-based diagnosis of depression. Kidney Int 2008; 74:930-6.
- Hedayati SS, Jiang W, O’Connor CM, Kuchibhatla M, Krishnan KR, Cuffe MS, Blazing MA, Szczech LA. The association between depression and chronic kidney disease and mortality among patients hospitalized with congestive heart failure. Am J Kidney Dis 2004; 44 (2): 207-15.
- Chan R, Steel Z, Brooks R, Heung T, Erlich J, Chow J, Suranyi M. Psychosocial risk and protective factors for depression in the dialysis population: a systematic review and meta-regression analysis. J Psychosom Res 2011; 71 (5):300-10.
- Jansen LD, Grootendorst CD, Rijken M, Heijmans M, Kaptein Ad A, Boeschoten EW, Dekker FW, PREPARE-2 Study Group. Pre-dialysis patients' perceived autonomy, self-esteem and labor participation: associations with illness perceptions and treatment perceptions. A cross-sectional study. BMC Nephrology 2010; 11:35.
- Ryan RM, Brown KW. Why we don't need self-esteem: On fundamental needs, contingent love, and mindfulness. Psychol Inq 2003; 14 (1):71-76.
- Paradise AW, Kernis MH. Self-esteem and psychological well-being: implications of fragile self-esteem. J Soc Clin Psych 2002; 21:345-361.
- Marinakis D, Xanthopoulos B. Anemia and chronic kidney disease. Treatment. Use of iron preparations, vitamin B12, folic acid and vitamin complexes. Dialysis Living 2009; 24: 36-50.
- Merkus MP, Jager KJ, Dekker FW, Boeschoten EW, Stevens P, Krediet RT. Quality of life in patients of chronic dialysis: self-assessment 3 months after the start of treatment. The Necosad Study Group. Am J Kidney Dis 1997; 29: 584-592.
- Zyga S. Anemia of chronic kidney disease. Clinical manifestations - diagnosis. Proceedings of the 19th Conference of Nephrology Nurses: ‘Anemia in chronic kidney disease and its treatment’, 2008; 37-43.
- Balodimos C, Petropoulou H, Triantafyllou G. The treatment of chronic pain in patients with hemodialysis. Dialysis Living 2006; 15: 6-12.
- Scalone L, Mantovani LG, Krol M, Rofail D, Ravera S, Bisconte M, Borgna-Pignatti C, Borsellino Z, Cianciulli P, Gallisai D, Prossomariti L, StefĂ no I, Cappellini MD. Costs, quality of life, treatment satisfaction and compliance in patients with β-thalassemia major undergoing iron chelation therapy: the ITHACA study. 2008; 24 (7): 1905-1917.
- Tijerina MS. Psychosocial factors influencing Mexican-American women's adherence with hemodialysis treatment. Soc Work Health Care 2006; 43 (1):57-74.
- Arabatzi S. Protocol of training in nurses and patients in dialysis units. Proceedings of the 24th Conference of Nephrology Nurses: "Infections in dialysis" 2013.
- Zyga S. Chronic kidney disease and quality of life. Proceedings of the 9th Panhellenic Conference of public health and health services, 26-28/03/2012: "The health of the Greeks in the light of new 'epidemics.'" Round table: Haemodialysis patients and their approach to primary health care.
- Ju-Yeh Yang, Jenq-Wen Huang, Yu-Sen Peng, Shou-Shang Chiang, Chwei- Shiun Yang, Chin-Ching Yang, Huey- Wen Chen, Ming- Shiou Wu, Kwan- Dun Wu, Tun- Jun Tsai, Wan- Yu Chen. Quality of sleep and psychosocial factors for patients undergoing peritoneal dialysis. Perit Dial Int 2007; 27: 675-680.
- Theofilou P. Quality of life and mental health of patients with chronic periodic hemodialysis. Dialysis Living 2008; 21: 42-50.
- Barroso LVS, Miranda EP, Cruz NI, Medeiros M AS, Araujo ACO, Mota Filho FHA, Medeiros FC. Analysis of sexual function in kidney transplant men. Transplant Proc 2008; 40: 3489-3491.
- Balioti A, Bristogiannis G. Sexual dysfunction in patients with chronic kidney disease. INFO UROLOGY 2007; 47: 10-12.
- Coelho- Marques FZ, Wagner MB, Poli de Figueiredo CE. Quality of life and sexuality in chronic dialysis female patients. Int J Import Res 2006; 18: 539-543.
- Mavromatis P. Exercise and chronic renal failure. Dialysis Living 2005; 13: 22-38.
- McHorney CA, Ware JE, Lu JF, Sherbourne CD. The MOS 36-item Short- Form Health Survey (SF-36): III. Tests of data quality, scaling, assumptions and reliability across diverse patient groups. Med Care 1994; 32 (1): 40-66.
- Pappa E, Kontodimopoulos N, Niakas D. Validating and norming of the Greek SF-36 Health Survey. Quality of Life Research 2005; 14: 1433-1438.
- Kontodimopoulos N, Niakas D. Using KDQOL- SFTM for the measurement of health-related quality of life of Greek haemodialysis patients. Files of Greek Medicine 2007; 24 (6): 590-599.
- Economidou G, Zlatanos D, Vaiopoulos X, Hatzidimitriou X. Depression of patients with chronic renal failure. Dialysis Living 2005; 14: 22-32.
- Stavrianou K. Technology assessment of home dialysis study of factors affecting adoption and evaluation of quality of life of hemodialysis patients in Greece. Thesis, 2007, Available at website: https://nemertes.lis.upatras.gr/dspace/handle/123456789/511 (19/05/12).
- Creary J, Drennan J. Quality of life of patients on haemodialysis for end-stage renal disease. Journal of Advanced Nursing 2005; 51 (6): 577-586.
- Spyrou A. Stress in chronic dialysis patients. Thesis, 2004. Available at website: https://ktisis.cut.ac.cy/handle/10488/769 (10/05/2013).
- Joachim K. Quality of life of persons with chronic renal failure. Thesis, 2002. Available at website: https://ktisis.cut.ac.cy/jspui/handle/10488/770 (10/05/2013).
- Gabriel R. A patient’s guide to dialysis and transplantation (4th ed). Academic Publishers. Dordrecht: Kluwer, 1990.
- Levy NB. Psychological complications of dialysis. Bulletin of the Menninger Clinic 1984; 48 (3), 237-250.
- Theofilou P. Τhe role of sociodemographic factors in health – related quality of life of patients with end – stage renal disease. International Journal of Caring Sciences 2011; 4(1): 40-50.
- Golper T. Patient education: can it maximize the success of therapy? Nephrol Dial Transplant 2001; 16 (Suppl 7): 20-24.
- Aydinok Y, Eresmis S, Bukusoglu N, Yilmaz D, Solak U. Psychosocial implications of thalassemia Major. Pediatr.Int 2005; 47(1): 84-89.
- Koutsopoulou - Sofikiti EB. The effect of chronic hemodialysis in personality of uremic patients. PhD thesis. National and Kapodistrian University of Athens. 1999; 77.
- Davenport U, Strawgate- Kanefsky L. A CAPD patient group on sexuality – a critical view. Clin Exp Dial Apheresis 1983; 7 (4): 303-311.
- Carney RM, Wetzel RD, Hagberg J, Goldberg AP. The relationship between depression and aerobic capacity in hemodialysis patients. Psychosom Med 1986; 48 (1-2): 143.
- Morris PJ. Renal transplantation: indications, outcome, complications and results. In: Schrier RW, Gottschalk CW. (eds), Diseases of the kidney (4th ed.), Boston, Little Brown, 1988; 3:3211-35.
- Toorians AW, Janssen E, Laan E, Gooren LJ, Giltay EJ, Oe PL, Donker AJ, Everaerd W. Chronic renal failure and sexual functioning: clinical status versus objectively assessed sexual response. Nephrol 1997; 12: 2654-63.

