Niraj James Shah*
Department of Medicine, Division of Digestive Disease, The University of Mississippi Medical Center, 2500 North State Street, Jackson, MS, USA
Corresponding Author:
Niraj James Shah
Department of Medicine
Division of Digestive Disease
The University of Mississippi Medical Center
2500 North State Street, Jackson, MS, USA
Tel: 601-984-4540(7915)
E-mail: jnshah@umc.edu
Received date: September 27, 2017; Accepted date: October 09, 2017; Published date: October 12, 2017
Citation: Shah NJ (2017) Constrictive Pericarditis as a Cause of Ascites. Arch Med Vol No:9 Iss No:5:4
Copyright: © 2017 Shah NJ. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Image Article
A 71 year old Caucasian male with a past medical history of asthma, dyslipidemia and (a one year diagnosis of) cryptogenic cirrhosis was referred to the hepatology clinic for evaluation of ascites with imaging suggestive of cirrhosis. He complained of worsening exertional dyspnea, ascites and a 50 pound weight loss in the past 6 months. His exam was notable for ascites and elevated neck veins. He had normal liver function tests, platelet counts and INR. A diagnostic paracentesis revealed an elevated SAAG of 1.5 with negative infection or malignancy. He had a liver imaging performed 11 months prior at an outside hospital which revealed dilated hepatic veins and pericardial thickening (Figure 1a and 1b). An echocardiography and a right heart catheterization showed classic constrictive physiology with pericardial thickening suggestive of constrictive pericarditis.
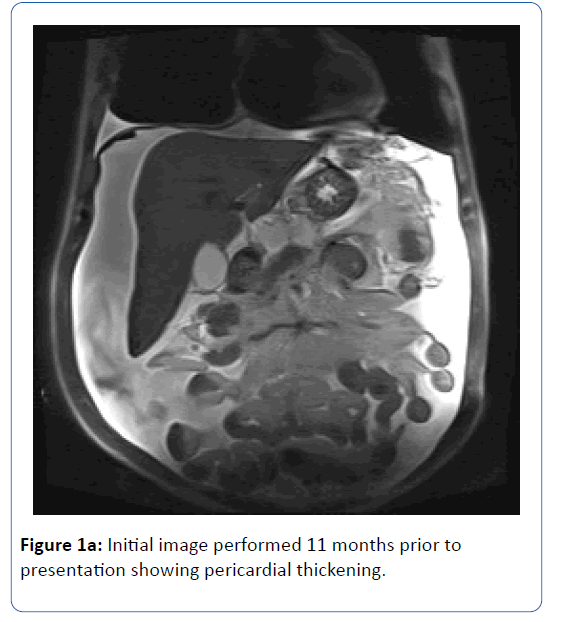
Figure 1a: Initial image performed 11 months prior to presentation showing pericardial thickening.
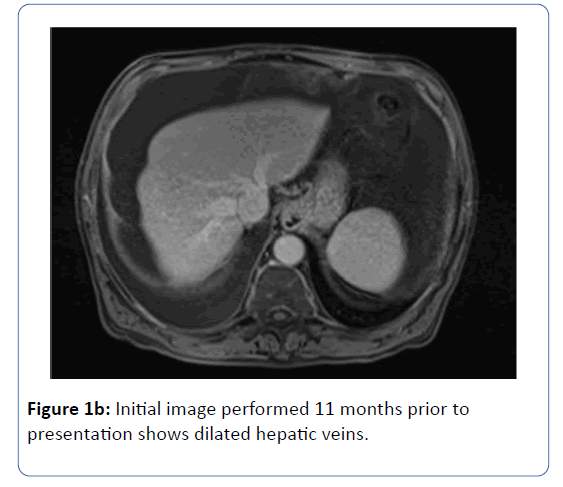
Figure 1b: Initial image performed 11 months prior to presentation shows dilated hepatic veins.
The patient was referred for a pericardiectomy. Post operatively he required two paracentesis. Presently, his ascites has entirely resolved (Figure 2).
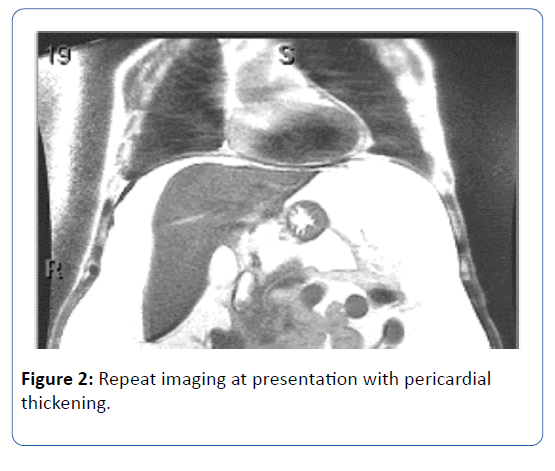
Figure 2: Repeat imaging at presentation with pericardial thickening.
20833


