Keywords
Trauma; Seniors; Youth; Health; Technology; Board; Restraint
Introduction
The Brazil is the sixth country in the ranking of highest percentage of elderly population in the world. The functional, biochemical and psychological modifications, accompanying morphological aging require special care to this population in various health care fields [1,2].
The percentage of trauma in the elderly increases significantly upon the growth of this population. The active lifestyle of the elderly raises exposure to risk of accidents. There are still some features belonging to the physiological aging, such as: reduced visual acuity, reduced hearing, use of medications, and lentificada diseases, contributing to the increase in trauma victims.
After the trauma, the elderly have a decline in their quality of life, failing to return fully to its initial state. Any change in the minimum physiological parameters can be evidence of a potentially lethal injury. Therefore, the initial approach of the elderly traumatized should be performed with greater attention and strictly monitored [3].
The trauma is an injury from; can be accidental, self-inflicted, or an act of violence that reaches all systems and requires immediate attention to avoid further damage, or loss of life [4].
The loss of bone mass is common in aging and is characterized by imbalance in the process of modeling and remodeling. These changes in the cells that make up bone mass can be characterized as osteoporosis. This pathology contributes to fractures of the hips and spontaneous fractures of the vertebral bodies for compression, because the bones become porous and brittle. Also resulting from this loss is kyphosis (curvature of the spine) in the thoracic region. Vertebral compression fractures are asymptomatic, therefore the rescuer must have high level of suspicion for rachimedular injuries during patient assessment [5].
As the thoracic spine becomes more curved head and shoulders protrude forward. In the geriatric patient, severe curvature of the spine due to kyphosis can determine a difficulty in aligning the cerebrospinal thoracic segment [5,6].
The Pre-Hospital Care (APH) is committed to the health of human beings and remains always present the individual requires an urgent and emergency care in Extramural environment. In the elderly, accidents are a major cause of crippling injuries and hospitalizations in nursing homes, or other institutions, constituting the Fifth cause of mortality among individuals with more than 75 years [7].
Although the trauma is more common in young people and the geriatric emergencies are usually clinics, the number of elderly trauma is relevant, because the injuries that could be easily tolerated by young patients can result in considerable mortality rates in the elderly [8].
Death due to trauma obeys a 1ch distribution. The first peak is the immediate death, occurs in the 30 minutes following the trauma. The second peak, early death, which occurs in the first two hours after the trauma. Patients benefit from a pre-hospital care adequately planned for your needs. So this moment is called the golden hour. Finally, the third peak is named late death that occurs after the first week of the trauma. Therefore, the appropriate service and fast at the event may represent a chance of survival for the victim [6].
Accidents and violence are among the main causes of death in the young and adult population. However, come the said studies revealing that causes are worthy of emphasis as well in the elderly population and this fact requires more attention and concern of health professionals [8].
It is considered as pre-hospital level in the area of mobile urgency, which seeks early to the victim, after have been a further to your health (clinical, surgical, traumatic nature, including the psychiatric diseases), which can lead to suffering, sequels or even to death, and must, therefore, provide care appropriate transport unit a properly tiered health service and integrated into the unified Health System [9].
One of the functions and duties of the APH mobile is to mobilize and remove patients with spinal protection, using planks and other immobilization and transportation equipment. There are several types of vehicles in the APH, everyone should carry several mobile equipment that assist in the management of the trauma. In the various vehicles of mobile equipment which APH must appear on any one of them is the Backboard immobilization of the spinal column (PLICV) [9].
In cases of necessity of APH, the patient with severe kyphosis may have injuries if fixed assets following the same protocols for young people, due to changes in the cervical spine. For the geriatric patient that needs to be immobilised and transported, must, therefore, use besides cervical immobilization equipment, cushions, pillows, blankets and other material to accommodate the curvature of the spine and establishing alignment between the spine and the head [5,6].
Despite these morphological changes in the elderly are well known, the pre-hospital care services use only PLICV adult and pediatric type. In the latter still needs the use of cushions to keep the spine in aligned position, rather than leaving it in a slight bending because of the disproportionately large size of the head [5].
The flat of the PLICV conformation not fits the greater curvature in the spine. As a consequence, rescuers usually improvise shaped cushions support in the cervical region of the elderly to avoid possible injuries caused by bad rachimedular adaptation of this appliance [5]. This reality leads to the necessity of creation of adapted devices for the elderly.
Even with the growing and disturbing rise in rates of trauma in the geriatric population, it should be noted that few studies seek to identify risk factors able to predict the onset of complications and mortality in that age group [8].
On the basis of the above this study sought to investigate the anatomic differences observed when the elderly and young are stabilized in Backboard immobilization of the spinal column, through comparison of measures between two points of the posterior cervical and the top edge of the PLICV.
Methods
This is an experimental research and transversal character. 110 subjects participated in the study, distributed in two groups: elderly (EG) and young people (YG), composed of 55 individuals, respectively. The subjects who participated in the young group should have between 20 to 30 years of age, while older people would need to be over the age of 60 years. These subjects were chosen at random and all had physical and cognitive capability preserved. They were thus able to contribute to this research. In a first moment was checked marked lordosis in a subject with fixed kyphosis, through the apparatus termed Portable Simetrógrafo Sanny. Then, the browser positioned itself behind the guy who was in standing position. There was the identification of the location of the point corresponding to the first (C1) and the seventh cervical vertebra (C7), by means of manual palpation technique, and were scored two points with a pencil dermatográfico black hypoallergenic Sanny. The first cervical vertebra, while not tangible, was located, as it is at the time of the earlobe, as shown in Figure 1.

Figure 1: Following the procedure performed on data collection. (A) The location of the first cervical vertebra. (B) identification of the first cervical vertebra. (C) Identification of the seventh cervical vertebra. (D) Distance of the vertebra to the Backboard immobilization of the cervical spine.
Subsequently, the subject of the group EG and YG laid individually on long plank of cervical immobilization (PLICV), in dorsal decubitus, where was held the manual stabilization of the cervical spine and measured the distance in centimeters (cm) of the back of the neck, corresponding to the level of the first and seventh cervical vertebra, the contact surface of the PLICV (Figure 1).
The pencil had intended to ensure the correct location of the measure corresponding to the posterior cervical region, at the time of the first and the seventh cervical vertebra, minimizing mistakes.
During the procedure (cervical stabilization), the subjects mentioned your level of pain as the Numerical Estimate scale (Numeric Rating Scale-NRS). Stabilization lasted five minutes, to then be asked about the presence of pain and mention your level. Figure 1 demonstrates the procedure runs.
All subjects laid on PLICV in dorsal decubitus. They threw and raised without the need for foreign aid, since this is subject to physical and cognitive capability preserved. This study has not evaluated the procedure of placing the patient on the stretcher, but only his position once positioned on the Board. We understand that as important as it is in this position that he remains until the end of the procedure.
The data are presented as frequency, mean values and standard deviation of the mean. It was held first the Kolmogorov- Smirnov test. The independent T test was used to compare the characteristics of the subjects of the two groups. Adopted 5 confidence level for these tests. These procedures were performed in the software Instat 3.0.1 (Graph Pad Urges, San Diego, CA, USA) and the graphics in GraphPad Prism 3.0.
The study received assent and final by the ethics on Research Committee of the Centro Universitário de João Pessoa-CEPUNIPÊ. All survey respondents were asked to sign the informed consent according to the resolution of the National Health Council 19696.
Steps away from the board: cervical PLICV is designed for manual transport accident victims. Rigid, lightweight and comfortable. Has large tongs for ease of use with gloves. Angled design for better accommodation of the patient. Translucent, for use in x-ray and magnetic resonance imaging. Has specific openings to facilitate immobilization of victim. Allows the rescue in the water and at times. Produced in polyethylene with high impact resistance. Dimensions: height 65 mm; load capacity 180 kg; overall length 1830 mm; width 440 mm; weight 6.5 kg; 0.07 m³ volume.
The subjects were submitted to measure the distance in centimeters from the posterior portion of the neck, corresponding to the level of the first cervical vertebra (C1), and the seventh cervical vertebra (C7) the surface of contact with the equipment. For this, we used a tape measure Sanny (American Medical of Brazil Ltda., São Bernardo do Campo, Brazil) with precision in mm. The measuring tape Sanny was used, as recommended by the scientific community to be in accordance with the established standards for the dimensions of width and thickness of the tape. Very flexible, trena Sanny fits precisely the body circumferences, providing accurate measurement. Because it is made of steel, is inelastic, maintaining its accuracy over time.
Your box is manufactured in ABS, high-strength material, avoiding breakage. For the collection of measures, was used the technique of palpation manual, as well as, a dermatological allergy pencil marking the location of measurement, ensuring greater accuracy that the measures were being carried out in the correct place, because it would be difficult to find the points of measurement with the individual in dorsal decubitus.
By predict that as with tape measure could be a curvature of the same, changing the result, a comparison was made of the measure with a caliper (Sanny ® with accuracy 0, 1 cm). The data showed that there were no differences between the measures with these two instruments, nor for C1 or to C7, with young or elderly. These figures attest to the use the tape measure to the measures.
Application of numerical scale of pain: when it is stabilized in PLICV, the subject reported the intensity of their pain, as the Numerical Estimate scale (Numeric Rating Scale-NRS) that assess the pain on a scale of 1 to 10, with 0 showing no pain and 10 indicating the worst pain. This measure is used to assess pain intensity levels [10].
Evaluation of cervical kyphosis: Kyphosis was measured by means of the apparatus termed Portable Simetrógrafo Sanny. This appliance is equipped with horizontal and vertical lines that enable the professional to perform a subjective evaluation of postural deviation. Can be built easily with a transparent plate (glass or acrylic) of approximately 2.00 m x 0.90 m, scratched vertically and horizontally to form squares of 5 cm, and with a setup that allows you to stand, identifying postural deviations more evident. The evaluated was placed in an orthostatic position side (sagittal) in relation to the appliance, with your arms along the body, heels slightly apart about shoulder-width apart, arms loose at your sides and staring straight ahead. During the gathering, the evaluator stood at a distance of three metres from the evaluated, sitting in a chair with backrest. Postural evaluation, the subject was observed in the sagittal plane with the right or left shoulder parallel to the midline of the simetrógrafo. The following parameters were: head and neck. The criteria established to detect kyphosis was the protrusion of the cervical spine in relation to the median line of the simetrógrafo, as it is used by Moreira (2001) and (1998).
Results
The subject of EG and 68 ± 6 years possessed of 23 ± 3 YG years 69 % (38) women of EG and 78 (43) of YG.
The data referents pain stabilizing the cervical spine of the study subjects are shown in Table 1 and Figure 2.
Table 1: Pain reporting cervical stabilization.
| Ache |
N |
% |
M ± DS |
| Presence of pain in elderly |
50 |
90 |
9 ± 2 |
| Absence of pain in the elderly |
5 |
10 |
- |
| Presence of pain in young |
- |
- |
- |
| Absence of pain in young |
55 |
100 |
- |
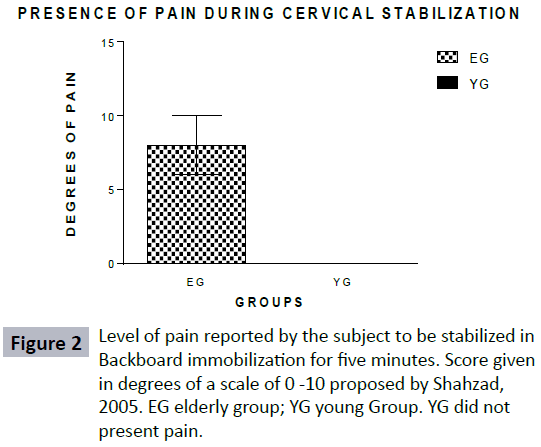
Figure 2: Level of pain reported by the subject to be stabilized in Backboard immobilization for five minutes. Score given in degrees of a scale of 0 -10 proposed by Shahzad, 2005. EG elderly group; YG young Group. YG did not present pain.
N = absolute number, % = percentage, M = media degrees of pain, DS = standard deviation of the average.
The sample evaluated, 96.4 % (53) of the elderly had kyphosis and 32.8 % (18) of young people as well, while the other had curvature of the spine considered normal.
Figures 3 and 4 demonstrates the distance corresponding to the posterior portion, at the first (back of neck) and the seventh cervical vertebra (neck) the surface of contact with the PLICV.
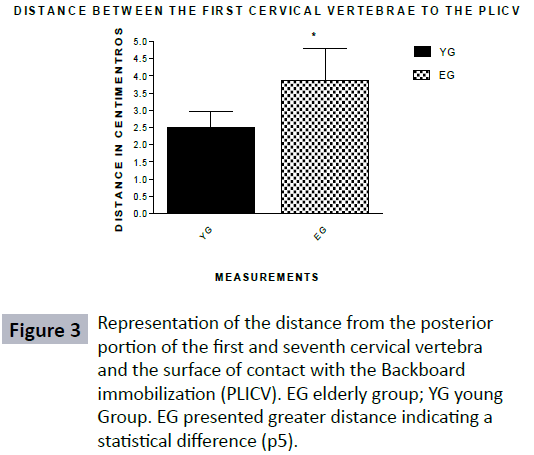
Figure 3: Representation of the distance from the posterior portion of the first and seventh cervical vertebra and the surface of contact with the Backboard immobilization (PLICV). EG elderly group; YG young Group. EG presented greater distance indicating a statistical difference (p5).

Figure 4: Distance of the seventh cervical vertebra of the plicv.
It is observed in Figures 3 and 4 that the elderly are stabilized in PLICV, differences in confrontation with young guys. The subject of YG show 2.4 ± 0, 4 cm, while the EG 3.8 ± 0.9 cm, confirming the existence of a dead space between the region corresponding to the first cervical vertebra and the contact surface with the PLICV, which is superior in EG. The distance corresponding to the seventh cervical vertebra also showed differences in both, being: YG 2.15 ± 0, 59 cm and 4.4 ± 0.72 cm EG.
Discussion
There is a lack of studies proving the inadequacy of PLICV for elder. Thus, this study comes from an unprecedented way confirm the theory that the PLICV requires adaptations to accommodate this audience. We hope to contribute to the scientific society, in order to stimulate researchers to invest more on this theme.
To assist the elderly, trauma victim, the rescuer has to be concerned with the following issues: differences in the anatomy of the cervical spine and thoracic spine, osteoporosis, etc. In the geriatric patient severe curvature of the spine due to kyphosis, may determine a difficulty in aligning the cerebrospinal segment. The elderly with severe kyphosis may have injuries if immobilized forcibly, in the same way that a young patient [6].
Thoracic kyphosis leads senior forward's head away from the backboard, more than in young people. Therefore, individualized assistance is needed for the elderly, so that they do not cause damage associated with the pre-hospital care inadequate.
There is a systematic approach in protocols to better serve victims of trauma, that is, an order of priorities that interfere in the survival of the victim. The basic equipment used in the initial approach to the victim of trauma are: and PLICV that have the primary function of minimizing possible damage to the spine.
However, the PLICV available for APH mobile systems are only intended for young patients and Pediatric [5,9]. Based on this concept, the figure two, presented earlier, showed the distance between the posterior portion of the first and seventh cervical vertebra and the surface of contact with the PLICV.
The analysis of this figure showed that the elderly are stabilized inappropriately in PLICV and this could be avoided if there was a device to fill the dead space between the equipment and the cervical spine [11,12].
It is known that the cervical stabilization composes the first stage to be held in a situation of trauma and that if this is not performed properly will cause secondary lesions, as the rachis injury.
The spinal column has as main features two opposing roles: rigidity and mobility. Is supported in the hip bones, serves as a support to the skull, and protection for the spinal cord which constitutes a high specialization and tissue fragility, where circulating all motor sensory orders ranging from periphery to the brain. Such a structure, if damaged, will lead to serious damage to human health that can acquire irreversible pathology that will influence in your life, preventing him from exercising their activities normally [13,14].
Thus, the care of the Airways and the stabilization of the cervical spine of the victim are priorities in attendance. In this respect, the correct installation of the appropriate equipment, to keep the airway pérvia and good stabilization of the cervical spine, is of great importance for the success of attendance [5].
There is no effective treatment able to restore the functions of the spinal cord. The treatment is performed for the rehabilitation of patients, so that every effort should be made to prevent irreversible injury like that [15].
Despite recent advances in medicine, spinal trauma (Traumatic Rachis (TRM)) remain as one of the most tragic injury. The main objective in attending to the victims of trauma involving the spine and marrow is to reduce the chance of there being neurological deficits and prevent additional injuries that may occur in the service to the victim. Most injuries happen in the cervical region (neck area) [15,16].
It is known that elderly people have the spine damaged by anatomical and physiological changes characteristic of senescence and that are more conducive to becoming victims of external trauma. Therefore, it is imperative that a particular vision of APH, related to this audience, but also that the existing equipment for adults and are suited to the anatomofisiológicas changes of the elderly. With the proper equipment, focusing on rachimedular Trauma (TRM), can reduce considerably the number of spinal injuries [17,18].
By be on anthropometric tape measure could be a curvature of the same, changing the result, a comparison was made of the measure with a caliper (Sanny ® with accuracy 0, 1 cm). The data showed that there were no differences between the measures with these two instruments, nor for C1 or to C7 's with young or elderly. These figures attest to the use of anthropometric tape to the measures.
In the elderly, stabilization should be performed in a manner that is cautious, because the instrument used by the emergency services and pre-hospital emergency do not fit the anatomical and physiological changes of aging, being the first responder use of improvisation in the attempt to provide appropriate assistance.
Conclusions
The pre-hospital care is intended to deal with situations of imminent risk of death, avoiding complications of previously existing lesions. The health professional who attends this audience should consider the changes arising from the aging process, adapting its assistance and equipment to the elderly trauma victim.
At the end, they identified the respective distances between the Board and the region corresponding to the first cervical vertebra of the elderly: 3.8 ± 0, 9 cm and 2.4 ± 0, young 4 cm and the seventh rib: elderly 4.4 ± 0, 72 cm and young 2.15 ± 0, 59 cm, thus confirming a statistically significant difference between the two groups as it showed the measures taken with the tape Sanny, ratifying the hypothesis suggested in this dead space between the spine of elderly with kyphosis and the contact surface of the PLICV. This research sets out to be inconclusive and future studies are needed to confirm these results.
Such a find, induces researchers analyses by means of x-rays, the sagittal Cobb, or by the Flexicurva Method of the cifótico angle of the thoracic spine. Still, evaluates the degree of seriousness of a removal of an old man with severe kyphosis, critical in the current Board.
Other studies have scoped the design of devices to adjust the current technology (PLICV) to the cifótico angle of the elderly and ensure a better stabilization of the cervical spine of these, providing customer service and damage-free removal and discomfort emphasized by the seniors involved in the research.
8708
References
- Vieira EB (2004) Handbook of Gerontology a theoretical-practical guide for professionals, caregivers and family members. ed2, edtRevinter, Rio de Janeiro.
- Hirano, Fraga GP, MantovanM (2007) Trauma in th e elderly. Rev. RibeirãoPreto Medicine 40: 352-357.
- Huddleston SS, Ferguson SG (2006)Clinical Emergencies: approaches, interventions and self-assessment. 3A ed. Rio de Janeiro: Guanabara Koogan; 2006.
- PHTLS (2009) Committee of NationalAssociationofEmergency Medical Technicians (NAEMT) in cooperation with the Committee on Trauma of the American College of dental surgeons. Pre hospital care to Traumatized PHTLS Prehospital Trauma Life Support. Rio de Janeiro: Elsevier.
- Tan RR, Lima FV (2004) Special considerations in the pre-hospital care to elderly trauma victim. Rev PaulEnf Act; 17: 229-234.
- Cantera GO, Sunday PL (2000)Nursing Guide: geriatrics. Rio de Janeiro: McGraw Hill.
- Lima RS, MLP Fields (2011) Profile of the elderly trauma victim answered in an urgent and emergency unit. RevEscEnferm USP; 45: 659-664.
- Ordinance No. 2048 GMMS, of November 5, 2002. Regulates the service of urgencies and emergencies.
- Shah FF, Silva Already (2005)The metric of pain (dormetria): theoretical and methodological issues. Rev PAIN 6: 469-513.
- Maung CA (2001) Physical activity at maturity: evaluation and exercise prescription. Rio de Janeiro: Shape.
- Nakashima H, Yukawa Y, Ito K, Machino M, El Zahlawy H, et al. (2011) Posterior approach for cervical fracture-dislocations with traumatic disc herniation. Eur Spine J 20: 387-394.
- Gentile JKA (2009) Pipelines in spinal cord injury. Rev Emergency Clinic, Barueri: Editorial Bolina Brazil Ltda 4: 124-130.
- Loyal MBF (2008) Spinal cord injury: an epidemiological study of 386 cases with emphasis to those patients admitted after four hours of the trauma. Neuro-Psychiatry files magazine, São Paulo: File Arq. Neuro-Psiquiatr 66: 365-368.
- Define HLA (1999) Spinal Cord Injury. Rev. MedicinaRibeirãoPreto. 32: 388-400.
- De Souza JA, Iglesias AC (2002) [Trauma in the elderly]. Rev Assoc Med Bras 48: 79-86.
- Chan,Farias GM, Saints KN (2009) Knowledge of nursing staff in the process of caring for victims of traumatic spinal medullar. Rev International Scientific Inter Science Place 2: 6.

