Keywords
Quality of life; Diabetes; Measurement; Foot ulcers
Introduction
Fifteen to twenty-five percent of persons with diabetes mellitus, sometime in their lifetime, will develop foot ulcers particularly susceptible to infections (diabetic foot ulcers, DFUs). An infection in the feet can rapidly be spread causing severe tissue damages which can lead to the need of amputation [1-3].
Successful healing of DFUs often requires long periods of treatment with additional limitations in patients’ daily activities. This burden in the life of patients adversely affects Health-Related Quality of Life (HRQoL) [4-8].
The HRQoL concept was developed to meet the need of measuring the subjective perception of a person's health. The World Health Organization (WHO), in 1948, influenced by the opinions of Sigerist [9,10], defined health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity” [9,11]. This evolvement had emerged the need of measuring the physical, mental and social well-being, concepts which are related to the subjective perception of the individual and are beyond, and many times superior, than the measuring ability of the biomedical indicators. For fulfilling the above need the concept of Health-Related Quality of Life was developed [12].
An understanding of the determinants of DFU patients’ HRQoL may help health professionals in clinical decision making, specifying risk groups and allowing the prediction of the HRQoL.
Aim
The aim of this review was to ascertain the health-related quality of life determining factors of patients with diabetic foot ulcers.
Method
Search strategy
This review was conducted by searching in the electronic databases PubMed, and Scopus, for the period 2000 to March 2014.
The literature search was carried out using the following string of terms: "quality of life" AND "foot" and "ulcers". As a search criterion for the articles identification, the title of the publications was set.
Eligibility criteria
The selection of the studies conducted by two reviewers working independently. (AK, TK). Initially, the articles which yielded through the literature search, were evaluated, the duplicated records were removed and the related to the purpose of the review primary studies were chosen. Afterwards, at the second phase of the selection process, a review of the full text of the publications was taken place (Figure 1).
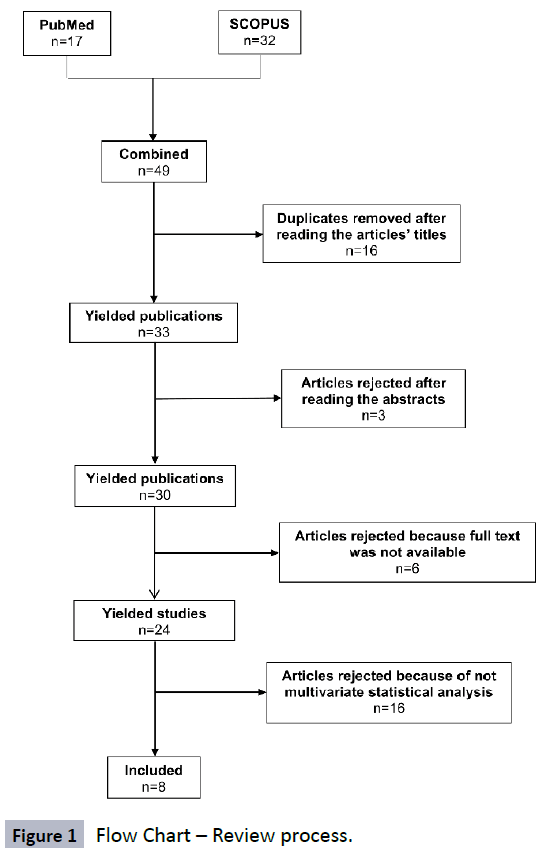
Figure 1: Flow Chart – Review process.
To include a study in the review, the following criteria were set:
• Articles written in English language.
• Reference population: Persons with Type 1 or Type 2 DM, with or without diabetic foot ulcers, regardless of age.
• Outcome: The health-related quality of life measured by a reliable and valid scale.
• Determinants: Factors concerning the health-related quality of life.
• Statistical analysis: Articles with multivariate analysis.
• Publications which are not measurement instrument development studies (scales/questionnaires) and
• Articles published in peer reviewed journals.
Data extraction
The data which retrieved from the studies, included in the review, came along after consensus of the AK and TK reviewers. The name of the study first author (or the names of the study authors in case they were two), measurement instrument, sample size, research design, gender, diabetes type (1 or 2), educational level, working status, care from others, marital status, duration of diabetes, type of treatment (insulin, medications or diet), ulcer size, ulcer duration, ulcer location, infection presence or absence, diabetes chronic complications, other health problems, body mass index (BMI), HbA1c levels, serum creatinine levels, CRP levels, ankle brachial index (ABI), Wagner ulcer classification and HRQoL outcomes were summarized (Tables 1 and 2).
Table 1: Summary of the studies included in the review.
| Study |
Country |
Sample |
Research design |
Measurement instrument |
| Ali Alzahrani&Sehlo[13] |
Saudi Arabia |
60 randomly selected adult persons with DFUs, 60 randomly selected adult people with DM and 60 matched healthy controls |
Analytical, retrospective, case-control |
SF-36 |
| Ribu et al. [6] |
Norway |
127 patients with DFUs |
Cross-sectional |
DFS, SF-36 |
| Ribu et al.[7] |
Norway |
127 patients with DFUs |
Cross-sectional |
SF-36 |
| Sanjari et al.[14] |
Iran |
54 patients with DFUs and 78 persons with DM Type 1 or Type 2 |
Analytical, retrospective, case-control |
SF-36 |
| Siersma et al. [18] |
Multicenter |
1232 patients with a new foot ulcer |
Cross-sectional |
Euro-Qol-5D |
| Yao et al. [16] |
China |
131 patients with DFUs |
Analytical, retrospective, case-control |
SF-36 |
| Yekta&Ghasemirad[15] |
Iran |
90 patients with DFUs and 160 persons with DM Type 2 |
Analytical, retrospective, case-control |
SF-36 |
| Valensi et al. [17] |
France |
239 patients with DFUs and 116 people with DM |
Analytical, retrospective, case-control |
DFS, SF-36 |
Table 2: Descriptive table of patients’ characteristics.
| Variables |
|
N |
Percentage |
| Gender |
Male |
1291 |
62,9% |
| Female |
762 |
37,1% |
| Total |
2053 |
100,0% |
| Educational level |
Secondary education |
169 |
8,2% |
| Bachelor’s degree |
61 |
3,0% |
| Missing values |
1823 |
88,8% |
| Total |
2053 |
100,0% |
| Working status |
Employed |
154 |
7,5% |
| Unemployed |
154 |
7,5% |
| Missing values |
1745 |
85,0% |
| Total |
2053 |
100,0% |
| Care from others |
Yes |
729 |
35,5% |
| Missing values |
1324 |
64,5% |
| Total |
2053 |
100,0% |
| Marital status |
Single |
122 |
5,9% |
| Married |
17 |
0,8% |
| Cohabitation |
78 |
3,8% |
| Missing values |
1836 |
89,4% |
| Total |
2053 |
100,0% |
| Diabetes duration |
< 5 years |
167 |
8,1% |
| 5 – 10 years |
275 |
13,4% |
| > 10 years |
1443 |
70,3% |
| Missing values |
168 |
8,2% |
| Total |
2053 |
100,0% |
| Treatment |
Insulin |
1244 |
60,6% |
| Medications |
190 |
9,3% |
| Diet |
4 |
0,2% |
| Total |
2053 |
100,0% |
| Ulcer size |
< 1 cm2 |
540 |
26,3% |
| 1 – 5 cm2 |
665 |
32,4% |
| > 5 cm2 |
147 |
7,2% |
| Missing values |
701 |
34,1% |
| Total |
2053 |
100,0% |
| Duration of ulcer |
< 1 week |
194 |
9,4% |
| 1 week – 3 months |
787 |
38,3% |
| > 3 months |
429 |
20,9% |
| Missing values |
643 |
31,3% |
| Total |
2053 |
100,0% |
| Ulcer location |
Forefoot |
702 |
34,2% |
| Midfoot |
392 |
19,1% |
| Heel |
166 |
8,1% |
| Missing values |
793 |
38,6% |
| Total |
2053 |
100,0% |
| Infection |
Yes |
673 |
32,8% |
| Missing values |
1380 |
67,2% |
| Total |
2053 |
100,0% |
| Diabetes chronic complications |
Cardiovascular disease |
264 |
12,9% |
| Retinopathy |
397 |
19,3% |
| Charcot foot |
9 |
0,4% |
| Amputation |
103 |
5,0% |
| Missing values |
1280 |
62,3% |
| Total |
2053 |
100,0% |
| Renal insufficiency |
Yes |
27 |
1,3% |
| Missing values |
2026 |
98,7% |
| Total |
2053 |
100,0% |
| Other health problems |
Yes |
362 |
17,6% |
| Missing values |
1691 |
82,4% |
| Total |
2053 |
100,0% |
| Body mass index (BMI) |
< 25 Kg/m2 |
79 |
3,8% |
| 25 – 29,9 kg/m2 |
349 |
17,0% |
| > 30 kg/m2 |
189 |
9,2% |
| Missing values |
1436 |
69,9% |
| Total |
2053 |
100,0% |
| HbA1c |
< 48 mmol/mol |
7 |
0,3% |
| 48 – 58 mmol/mol |
89 |
4,3% |
| > 58 mmol/mol |
339 |
16,5% |
| Missing values |
1618 |
78,8% |
| Total |
2053 |
100,0% |
| Serum creatinine |
Normal |
56 |
2,7% |
| High |
57 |
2,8% |
| Missing values |
1940 |
94,5% |
| Total |
2053 |
100,0% |
| CRP |
< 10 mg/l |
68 |
3,3% |
| > 10 mg/l |
38 |
1,9% |
| Missing values |
1947 |
94,8% |
| Total |
2053 |
100,0% |
| Ankle Branchial Index (ABI) |
< 0,9 |
58 |
2,8% |
| 0,9 – 1,2 |
59 |
2,9% |
| > 1,2 or unable to be determined |
25 |
1,2% |
| Missing values |
1911 |
93,1% |
| Total |
2053 |
100,0% |
| Wagner ulcer classification |
Grade 1 |
127 |
6,2% |
| Grade 2 |
58 |
2,8% |
| Grade 3 |
158 |
7,7% |
| Grade 4 |
31 |
1,5% |
| Missing values |
1679 |
81,8% |
| Total |
2053 |
100,0% |
Data analysis
The Wald chi-square test was used to evaluate the contribution of each sociodemographic and clinical variable in the multivariate model. The dependent variable of the linear model was the SF-36 domains mean score.
Results
After the selection process (Figure 1) eight studies were included in the review, five of analytical, retrospective, case-control research design and three of cross-sectional.
The studies of Ali Alzahrani and Sehlo [13] from Saudi Arabia, Sanjari et al. [14] and Yekta & Ghasemirad [15] from Iran, Yao et al. [16] from China and Valensi et al. [17] from France were of the analytical, retrospective case-control design while the two studies of Ribu et al. [6,7] and the study of Siersma et al. [18] were of the cross-sectional design (Table 1).
By the statistical analysis it was detected that positive impact on DFU patients’ HRQoL had the Type 1 DM (Wald Chi- Square=164,69, p<0,001), the lack of family obligations (X2=24,96, p<0,001), the utilization of non-pharmacological interventions for the management of diabetes (diet) (X2=21,61, p<0,001), the ulcer size of >5cm2 (X2=1758,92, p<0,001), the ulcer location at the forefoot or midfoot (X2=24,23, p<0,001 and X2=39,21, p<0,001 respectively), the BMI of 25-29,9kg/m2 (X2=215,67, p<0,001) and the high serum creatinine levels (X2=391,97, p<0,001).
On the other hand, negative influence on DFU patients’ HRQoL had the unemployment status (X2=560,69, p<0,001), the duration of diabetes >10 years (X2=158,84, p<0,001), the duration of ulcer/s from 1 week to 3 months (X2=354,46, p<0,001), the cardiovascular complications (X2=83,35, p<0,001), and the HbA1c levels >58 mmol/mol (X2=1331,41, p<0,001) (Tables 2 and 3).
Table 3: DFU patients’ HRQoL determining factors.
| Factors |
B |
Wald Chi-Square |
P value |
| Type of diabetes |
Type 1 |
9,89 |
164,69 |
< 0,001 |
| Type 2 |
8,34 |
169,03 |
< 0,001 |
| Working status |
Employed |
-18,64 |
496,43 |
< 0,001 |
| Unemployed |
-19,47 |
560,69 |
< 0,001 |
| Marital status |
Single |
2,82 |
24,97 |
< 0,001 |
| Married |
1,23 |
1,49 |
0,223 |
| Cohabitation |
-1,49 |
2,41 |
0,120 |
| Diabetes duration |
< 5 years |
-1,72 |
3,38 |
0,066 |
| 5 – 10 years |
-2,91 |
18,48 |
< 0,001 |
| > 10 years |
-6,85 |
158,84 |
< 0,001 |
| Treatment |
Insulin |
2,06 |
27,07 |
< 0,001 |
| Medications |
5,67 |
90,76 |
< 0,001 |
| Diet |
7,47 |
21,61 |
< 0,001 |
| Ulcer size |
< 1 cm2 |
28,27 |
1029,85 |
< 0,001 |
| 1 – 5 cm2 |
28,89 |
1249,23 |
< 0,001 |
| > 5 cm2 |
29,22 |
1758,92 |
< 0,001 |
| Duration of ulcer |
< 1 week |
-10,33 |
178,44 |
< 0,001 |
| 1 week – 3 months |
-10,59 |
354,46 |
< 0,001 |
| > 3 months |
-8,06 |
203,06 |
< 0,001 |
| Ulcer location |
Forefoot |
3,89 |
24,23 |
< 0,001 |
| Midfoot |
3,89 |
39,21 |
< 0,001 |
| Heel |
2,92 |
32,37 |
< 0,001 |
| Diabetes chronic complications |
Cardiovascular disease |
-4,96 |
83,35 |
< 0,001 |
| Retinopathy |
-3,55 |
114,64 |
< 0,001 |
| Charcot foot |
-2,85 |
6,21 |
0,013 |
| Amputation |
-3,57 |
31,98 |
< 0,001 |
| Body mass index (BMI) |
< 25 Kg/m2 |
6,16 |
49,75 |
< 0,001 |
| 25 – 29,9 kg/m2 |
9,32 |
215,67 |
< 0,001 |
| > 30 kg/m2 |
7,43 |
135,26 |
< 0,001 |
| HbA1c |
< 48 mmol/mol |
-26,69 |
255,06 |
< 0,001 |
| 48 – 58 mmol/mol |
-26,69 |
458,71 |
< 0,001 |
| > 58 mmol/mol |
-27,59 |
1331,41 |
< 0,001 |
| Serum creatinine |
Normal |
44,01 |
398,94 |
< 0,001 |
| High |
44,32 |
391,97 |
< 0,001 |
Discussion
Diabetic foot ulcers, for being successfully managed, need long periods of treatment that bring about restrictions on patients’ daily activities and negatively influence the HRQoL. An understanding of the determinants of DFU patients’ HRQoL could help health professionals in clinical decision making as well as in screening and in the prediction of quality of life [4].
The most significant finding of this review, was the fact that cardiovascular complications have a negative effect on HRQoL. This finding is in agreement with the study done by De Visser et al. [19] in which the cardiovascular disease had a negative impact on quality of life of people with DM Type 2.
Another weighty finding was the positive effect on HRQoL of the diet as main diabetes treatment. Diet as a non-pharmacological intervention may promote the empowerment of the DFU patients and hence the, subjectively assessed, HRQoL. According to Elvin-Lewis [20] “for a variety of reasons more individuals are nowadays preferring to take personal control over their health, not only in the prevention of diseases but also to treat them”. It is worth mentioning that numerous trials has been conducted regarding the effectiveness of herbs and dietary supplements on DM glycemic control but with insufficient evidence to be provided [21].
In regard to working status, it was detected that unemployment status has adverse influence on HRQoL. Employment is a factor of wealth production and therefore a factor of better health services receiving [22,23].
With respect to ulcer size, size >5cm2 was found to have positive impact on HRQoL. This finding seems a bit peculiar but it could be explained by the fact that the patients with bigger ulcers may receive better therapeutic equipment (casts or appropriate footwear) resulting in better everyday functionality.
With regard to diabetes type, DM Type 1 had positive effect on HRQoL. DFUs usually occurs much later after diagnosis in persons with DM Type 1 [24]. There is a possibility the people’s with DM Type 1 total sample of the studies which were included in the systematic review to reflect the aforementioned acknowledgement, and hence, the prevalence of diabetic foot syndrome to be lower than the persons’ with DM Type 2 commensurate sample.
In terms of diabetes duration, duration >10 years had negative impact on HRQoL. This detection is consonant to the findings of Sparring et al. study [25] that diabetes duration associated negatively to HRQoL levels such as of Redekop et al. study [26] in which persons with ≥10 years diabetes duration was the subgroup with the lowest quality of life score (for mobility Euroqol 5D subscale, the P value was <0,0001) and of Papadopoulos et al. [27] (Physical Functioning SF-36 subscale, 56,4 score, p=0,049 and Vitality subscale, 47,4 score, p=0,016).
In relation to marital status, single status was found to have affirmative influence on HRQoL. Although in accordance to the literature [27,28] married people mark better scores on quality of life measurement instruments, this could be explained by the case that DFUs affect primarily physical well-being and therefore having family obligations might burden more persons with diabetic ulcers. Additionally, an alternative explanatory hypothesis could be that the concrete detection mirrors relevant sample synthesis. For example, concordantly to the study done by Han et al. [29], single women have higher quality of life values than single men.
By the data analysis, it was detected that ulcer durations from <1 week and 1 week to 3 months affect HRQoL more adversely than duration >3 months. Duration of 1 week to 3 months could be considered to be included in the crisis phase of diabetic foot disease, so, the burden on the individual is greater [30]. Furthermore, in a time period of >3 months, it is likely the ulcers to have been cured largely.
With respect to the ulcer location, site of the sore did not have negative influence on HRQoL. Less positive contribution in the multivariate model had the location of the heel (B=2,92, p<0,001).
Regarding BMI, it was found that BMIs of 25-29,9 kg/m2 and of >30 kg/m2 have more positive impact on HRQoL than a BMI of <25 Kg/m2. This detection is in contrast with the literature [31-33]. However, DFU patients with higher BMI than the normal may be unconcerned with their health issues and this could be reflected on their subjective perception of their well-being. They might have developed a fictitious sense of good well-being.
Concerning HbA1c levels, concentration of >58 mmol/mol had adverse effect on HRQoL. Low HbA1c values are associated with higher mental quality of life scores [34].
With regard to serum creatinine levels, high levels were detected to have affirmative effect on HRQoL. Physical exercise, and hence unrestricted mobility, is positively associated with serum creatinine for both men and women [35]. High creatinine levels might correspond to persons with less foot problems.
Limitations
The two reviewers (AK, TK) did not have direct access to the EMBASE database [36]. Although the review of Burnham [37] claims that Scopus has 100% coverage of EMBASE, recently published studies might was absented.
Conclusions
Since HRQoL is an important health outcome measure, health professionals could emphasize more on the prompt treatment of diabetic ulcers, the prevention and treatment of cardiovascular complications as well as on the promotion of employment among DFU patients and the utilization of non-pharmacological interventions for managing diabetes.
Another modifiable factor which should be taken into account is HbA1c and its regulation through glycemic control.
7425
References
- Edmonds M, Foster A(2011) The diabetic foot. In: Wass AHJ, Stewart MP (eds) Endocrinology and diabetes. 2nd ed. Oxford University Press, New York.
- Polikandrioti M, Kalogianni A (2009) Education on foot care in people with diabetes mellitus, type II. Rostrum of Asclepius 8: 107-119.
- Manes C, Sotiropoulos A, Katsaros T (2003) [Diabetic Foot]. In: Tountas DC (eds) [Diabetes Mellitus: Theory – Practice]. Athens.
- Tennvall GR, Apelqvist J (2000) Health-related quality of life in patients with diabetes mellitus and foot ulcers.J Diabetes Complications 14: 235-241.
- Abetz L, Sutton M, Brady L, McNulty P, Gagnon DD (2002) The Diabetic Foot Ulcer Scale (DFS): a quality of life instrument for use in clinical trials. Pract Diab Int 19: 167-175.
- Ribu L, Hanestad BR, Moum T, Birkeland K, Rustoen T (2007) Health-related quality of life among patients with diabetes and foot ulcers: association with demographic and clinical characteristics. J Diabetes Complications 21: 227-236.
- Ribu L, Birkeland K, Hanestad BR, Moum T, Rustoen T (2008) A longitudinal study of patients with diabetes and foot ulcers and their health-related quality of life: wound healing and quality-of-life changes.J Diabetes Complications 22: 400-407.
- De Almeida SA, Silveira MM, Do Santo PFE, De Pereira RC, Salome GM (2013) Assessment of the quality of life of patients with diabetes mellitus and foot ulcers. Rev Bras Cir Plast 28: 142-146.
- Terris M (1975) The contributions of Henry E. Sigerist to health service organization.Milbank Mem Fund Q Health Soc 53: 489-530.
- Tountas Y, Sarafis P (2009) Η Υ[The Health of the Greek Population]. Athens, Papazisis.
- Ali Alzahrani H, Sehlo MG (2013) The impact of religious connectedness on health-related quality of life in patients with diabetic foot ulcers.J Relig Health 52: 840-850.
- Sanjari M, Safari S, Shokoohi M, Safizade H, Rashidinezhad H, et al. (2011) A cross-sectional study in Kerman, Iran, on the effect of diabetic foot ulcer on health-related quality of life.Int J Low Extrem Wounds 10: 200-206.
- Yekta Z, Pourali R, Ghasemi-rad M (2011) Comparison of demographic and clinical characteristics influencing health-related quality of life in patients with diabetic foot ulcers and those without foot ulcers. Diabetes Metab Syndr Obes 4: 393–399.
- Yao H, Ting X, Minjie W, Yemin C, Xiqiao W, et al. (2012) The investigation of demographic characteristics and the health-related quality of life in patients with diabetic foot ulcers at first presentation.Int J Low Extrem Wounds 11: 187-193.
- Valensi P, Girod I, Baron F, Moreau-Defarges T, Guillon P (2005) Quality of life and clinical correlates in patients with diabetic foot ulcers.Diabetes Metab 31: 263-271.
- Siersma V, Thorsen H, Holstein PE, Kars M, Apelqvist J, et al. (2013) Importance of factors determining the low health-related quality of life in people presenting with a diabetic foot ulcer: the Eurodiale study.Diabet Med 30: 1382-1387.
- De Visser CL, Bilo HJ, Groenier KH, de Visser W, Jong Meyboom-de B (2002) The influence of cardiovascular disease on quality of life in type 2 diabetics.Qual Life Res 11: 249-261.
- Elvin-Lewis M (2001) Should we be concerned about herbal remedies.J Ethnopharmacol 75: 141-164.
- Yeh GY, Eisenberg DM, Kaptchuk TJ, Phillips RS (2003) Systematic review of herbs and dietary supplements for glycemic control in diabetes.Diabetes Care 26: 1277-1294.
- Park BH, Jung M, Lee TJ (2009) Associations of income and wealth with health status in the Korean elderly.J Prev Med Public Health 42: 275-282.
- Link BG, Phelan J (1995) Social conditions as fundamental causes of disease.J Health Soc Behav Spec No: 80-94.
- Sparring V, Nyström L, Wahlström R, Jonsson PM, Östman J et al. (2013) Diabetes duration and health-related quality of life in individuals with onset of diabetes in the age group 15—34 years–a Swedish population-based study using EQ-5D. BMC public health 13: 377.
- Redekop WK, Koopmanschap MA, Stolk RP, Rutten GE, Wolffenbuttel BH, et al. (2002) Health-related quality of life and treatment satisfaction in Dutch patients with type 2 diabetes.Diabetes Care 25: 458-463.
- Papadopoulos AA, Kontodimopoulos N, Frydas A, Ikonomakis E, Niakas D (2007) Predictors of health-related quality of life in type II diabetic patients in Greece.BMC Public Health 7: 186.
- Jacobson AM, De Groot M, Samson JA (1994) The evaluation of two measures of quality of life in patients with type I and type II diabetes. Diabetes Care 17: 267-274.
- Han KT, Park EC, Kim JH, Kim SJ, Park S (2014) Is marital status associated with quality of life?Health Qual Life Outcomes 12: 109.
- Taylor, Shelley E (2012) Health psychology. 8th ed. McGraw-Hill, New York.
- Ul-Haq Z, Mackay DF, Fenwick E, Pell JP (2013) Meta-analysis of the association between body mass index and health-related quality of life among adults, assessed by the SF-36.Obesity (Silver Spring) 21: 322-327.
- Kearns B, Ara R, Young T, Relton C (2013) Association between body mass index and health-related quality of life, and the impact of self-reported long-term conditions - cross-sectional study from the south Yorkshire cohort dataset. BMC Public Health 13: 1009.
- Bottone FG Jr, Hawkins K, Musich S, Cheng Y, Ozminkowski RJ, et al. (2013) The relationship between body mass index and quality of life in community-living older adults living in the United States.J Nutr Health Aging 17: 495-501.
- Lau CY, Qureshi AK, Scott SG (2004) Association between glycaemic control and quality of life in diabetes mellitus.J Postgrad Med 50: 189-193.
- Vikse BE, Vollset SE, Tell GS, Refsum H, Iversen BM (2004) Distribution and determinants of serum creatinine in the general population: the Hordaland Health Study.Scand J Clin Lab Invest 64: 709-722.
- Wright RW, Brand RA, Dunn W, Spindler KP (2007) How to write a systematic review.Clin Orthop Relat Res 455: 23-29.

