Ioannis Kyriazis1, Ioannis Raftakis2, Maria Rekleiti3, Emmanouil Mpeliotis4, Athanasios Lalousis5 and Greta Wozniak6*
1MD, PhD, 2nd Internal Medicine Department, “Asclepeion” Hospital, Voula, Athens, Greece
2MD, PhD, Rheumatology Department, “Asclepeion” Hospital, Voula, Athens, Greece
3RN, Msc, General Hospital of Korinth, Greece
4MD, 2nd Internal Medicine Department, “Asclepeion” Hospital, Voula, Athens, Greece
5MD, Rheumatology Department, “Asclepeion” Hospital, Voula, Athens, Greece
6MD, PhD, Radiology Department, Medical School, University of Thessaly, Larissa, Greece
- *Corresponding Author:
- Greta Wozniak MD, PhD
Radiology Department Medical School
University of Thessaly, Mezourlo 41 110
Larissa, Greece
Tel: +30 6972661842
E-mail: greta@med.uth.gr
Key words
Rheumatologic disorder, diffusive idiopathic skeletal hyperostosis
Introduction
Rheumatic diseases are between the most common diseases that are confronted at the primary level of health care, as well as the main cause of body incapability persons at 15 years old and over.
Ankylosin hyperostosis or Frostier’s disease or diffusive idiopathic hyperostosis (DISH) is a rheumatologic disease in which extensive fracture occurs along the conjunctions of the whole body but mainly at the front oblong conjunction of the spinal cord. Forestier’s disease is considered as a rare disease from the Committee of Rare Diseases of National Health Institute. This means that the disease or its subtype appears at less than 200.000 people in America. The disorder appears frequently in men at percentage of 65%, at age higher than 50 years old.[1-4] The birth of the disease is usually being located at age between 20 – 40 years old, but it takes a lot of years for its clinical and radiological expression. Epidemiological studies mention racial differences (white and colored).[2,3,5] The most of patients are asymptomatic while they can appear symptoms of arthritic pains, epicondylitis, trochantiritis.[3,6]
The cause is unknown and the diagnosis takes place by three basic radiological diagnostic finds:
1. Continual bridge like bone formation along of at least four adjoining vertebras.
2. Maintaining of the height of intervertebral spaces and intervertebral trays, with lack of bone degenerative falsifications such as hardener phenomena of vertebra.
3. Lack of ankylosin phenomena at arthritic surfaces of vertebra, loss of corrosive degenerative phenomena at the area of sacred bone and caudal, hardener and other endoarthric fracture phenomena.[2,3,6]
The last two criteria place the differential diagnosis between DISH and ankylosin spondylitis.[6]
Commonly appeared symptoms are dysphagia, which appears at about 28% of patients with DISH, laryngeal wheezing, laborious breathing, snoring and hoarseness. Other important symptoms that are related with Forestier’s syndrome are rigidity and back pain due to tenditis, myelopathy and pressure of marrow, which is related with hyperostosis of the back oblong conjunction and pain related with complications which concern the spinal cord, like fractures or partial disruption.[2,7-10] Patients with DISH have high risk of fracture after low energy damages.[3,11] These fractures are dangerous when concern spinal cord, due to delayed diagnosis and high rate of direct and indirect complications.
In many cases the distinction between the symptoms of the disease and its complications is hard and arbitrary. Disease complications consist of secondary situations, symptoms or disorders that are caused of the disease. The examination of these complications includes, except of the simple radiological examination, the CT and the MRI. Characteristic trait of DISH are falsifies that appear at both sides and symmetrically. Pelvis and the conjunctions, the ischiopublic, the patella, the heel and the olekrano frequently appear bone malignancies.[2,3,10,12-14] The radiological examination of the thoracic area of spinal cord is necessary for the differential diagnosis, due to possible findings.[10,15,16]
Case report of an early diagnosis of dish
43-years old-man presented with pain at waist and right rump for the 4-5 last years mainly at walking and prolonged standing. There wasn’t a history of morning rigidity. The last three years the patient appeared sterile arthritis of the right knee and the pain was increased and became intense at climbing and climbing down stairs or level. In addition, he observed a feel of tense at calf muscles at prolonged standing, which was relieved by resting.
Radiographs of the thorax spine showing calcification of the right anterior attitude ligaments and vertebral hyperostosis (Figure 1), the patients had no limitation of motion, pain or other joint symptoms. Laboratory studies revealed sedimentation rate of 15mm after 1 hour. Other blood tests were inconclusive (Hb: 14 g/dl, Hct: 42%, WBC: 6, 9 mm3, fasting glucose: 83 mg/dl and the rest biochemical analysis were normal as well, ASO: (-), hsCRP 0.5 mg/L.) Total lack of clinical expressions, of inflammatory musculoskeletal disease, lack of inflammatory indicators at related blood tests and characteristic representative findings, confirmed that the patient suffered of general, non inflammatory, idiopathic degenerative disease of musculoskeletal system that consisted DISH.
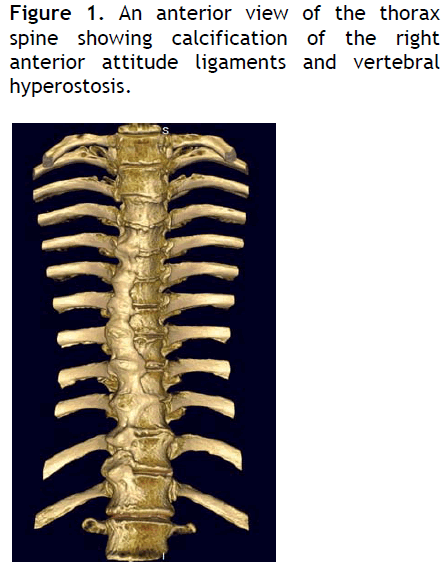
Figure 1: An anterior view of the thorax spine showing calcification of the right anterior attitude ligaments and vertebral hyperostosis.
The final diagnosis of DISH syndrome, instructions were given to the patient for symptomatic therapy with NSAIDs, combination of calcium- vitamin D2, diphosphonic and regular nature care. In additional, was applied acupuncture of thoracic - lumbar region of spinal cord. Diffusive Patient mentioned relief of symptoms at his, after 10 months, re-examination.
Discussion
At 1950, Forestier and Rotes Querol described a special type of ankylosing hyperostosis of spinal cord, which was different from the other diseases of spinal cord, including ankylosing arthritis and vertebra arthritis. Since then, the diagnosis of this special clinical radiological entity has been studied by a lot of radiologists and orthopedic surgeons. Spinal and out spinal demonstrations of the disease are summarized at annex 2 and 3.[17]
Resnick, Shaul and Robins (1975) proposed a more suitable definition, naming the Diffuse Idiopathic Skeletal Hyperostosis (DISH). The disease usually appears at adult patients, mainly men, with mild symptomatology.[18]
Patient’s history, the location and the nature are important. There aren’t laboratory examinations that help at differential diagnosis. When the hint of disorder is layed radiological examinations should be executed which have to include the thoracic area of spinal cord.[13] The lumbar area is being included at radiological examination due to the referred pain of patient. The recognition of the disorder is important for the patient because it gives an explanation to the symptomatology. The therapy to the disorder includes a symptomatic treatment and rarely surgical interventions, especially in specific complications. At patients with back pain move therapy, nature treatment and treatment with NSAIDs and diphosphonic are the most suitable symptomatic treatment.[3,18] The surgical confrontation is advisable at special cases such as fractures, narrowing, malignancies, and inflammations.[11] Acupuncture was used at the therapy of patient with back pain and Forestier’s disease. The symptoms improved very much by acupuncture where other therapies by analgesic, NSAIDs, natural therapy and water therapy proved ineffective. There isn’t any case at bibliography that medical acupuncture has been used at back pain therapy at such patients.
Conclusion
This incidence reminds us that doctors except rheumatologists usually fail at the differential diagnosis between inflammatory and sterile inflammatory diseases. This inefficacy has also been proved earlier. For this reason should not have always his thought at systematic diseases at a patient with rheumatologic demonstration, but to a wider pathological and rheumatologic approach, to use in an appropriate way the laboratory and the opinion of the special doctor. We believe that the including of a basic study of musculoskeletal system during the specialization, would improve this situation.
3372
References
- Weinfeld RM, Olson PN, Maki DD, Griffiths HJ. The prevalence of diffuse idiopathic skeletal hyperostosis (DISH) in two large American Midwest metropolitan hospital populations. Skeletal Radiol, 1997; 26: 222?5.
- Sharon G. Diffuse Idiopathic Skeletal Hyperostosis-Forestier?s Disease. Childs Orthopaedic Nursing, 2004; 23(6): 375.
- Sarzi-Puttini P, Atzeni F. New developments in our understanding of DISH (diffuse idiopathic skeletal hyperostosis). CurrOpinRheumatol, 2004; 16: 287?292.
- Kiss C, Szilagyi M, Paksy A, Poor G. Risk factors for diffuse idiopathic skeletal hyperostosis: a case?control study. Rheumatology, 2002; 41: 27?30.
- Robert M, Weinfeld Paul N, Olson Daniel D, Maki Harry J. The prevalence of diffuse idiopathic skeletal hyperostosis (DISH) in two large American Midwest metropolitan hospital populations. Griffiths Skeletal Radiol, 1997; 26: 222?225
- Cammisa M, DeSerio A, Guglielmi G. Diffuse idiopathic skeletal hyperostosis. Eur J Radiology, 1998; 27: S7?S11.
- Resnick D, Niwayama G. Diffuse idiopathic skeletal hyperostosis (DISH): Ankylosing hyperostosis of Forestier and Rotes-Querol, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, 3rd ed. Philadelphia: WB Saunders, 1995, vol 3, pp 1463-1495.
- Gay I, Elidan J: Dysphonia caused by Forestier?s disease. Ann OtolRhinolLaryngol, 1988; 97(3 pt1): 275-276.
- Palmer JHM, Ball DR. Awake tracheal intubation with the intubating laryngeal mask in a patient with diffuse idiopathic skeletal hyperostosis. Anaesthesia, 2000; 55: 70-74.
- Editorials. Clinical Manifestations of Diffuse Idiopathic Skeletal Hyperostosis ?DISH? Br J Rheumatology, 1996; 35: 1193-1196.
- Belanger TA, Rowe DE. Diffuse Idiopathic Skeletal Hyperostosis: Musculoskeletal Manifestations. J Am AcadOrthopSurg, 2001; 9: 258-267.
- Rotes Querol J. Clinical manifestations of diffuse idiopathic skeletal hyperostosis (DISH). Br J Rheumatol 1996; 5: 193?1194.
- Mata S, Hill RO, Joseph L, Kaplan P, Dussault R, Watts CS,et al. Chest radiographs as a screening test for diffuse idiopathic skeletal hyperostosis. J Rheumatol, 1993; 20(11): 1905-1910.
- Stechison MT, Tator CH. Cervical myelopathy in diffuse idiopathic skeletal hyperostosis: Case report. J Neurosurg, 1990; 73: 279-282.
- Vezyroglou G, Mitropoulos A, Kyriazis N, Antoniadis C. A metabolic syndrome in diffuse idiopathic skeletal hyperostosis: A controlled study. J Rheumatol, 1996; 23: 672-676.
- Matteucci BM. Metabolic and endocrine disease and arthritis. CurrOpinRheumatol, 1995: 356?358.
- Forestier J, Rotes-Querol J. Senile Ankylosing Hyperostosis of the Spine. Ann Rheum Dis, 1950; 9: 321-330.
- Resnick D, Shaul SR, Robins JM. Diffuse idiopathic skeletal hyperostosis (DISH): Forestier's disease with extraspinal manifestations. Radiology, 1975; 115: 513-24.

