Keywords
Music therapy, pain relief, post operative pain, non-pharmacological methods.
Introduction
Pain is a known consequence of surgery, an unpleasant sensory and emotional experience associated with potential or actual tissue damage or described in terms of such damage [1]. In fact, pain in the immediate postoperative period is one of the major concerns of health professionals looking after patients who had a surgery. Despite the availability of analgesic medication, pain remains a common problem, which can interfere with appetite and sleep, and can contribute to complications, prolonging hospitalization [2].
Patients undergoing an operation often experience a loss of control as well as fear of the unknown, fear of pain, uncertainty and anxiety, emotions that may intensify the perception of pain [3]. Furthermore physical and psychological stress contributes to perceived surgical pain, prolonging postoperative recovery time and enhancing immunosuppression [4]. Quite often post operatively, patients do not always receive sufficient pain relief from opioids and may have undesired side effects [5,6]. The most effective approach to managing patients’ pain in the immediate postoperative period may include a combination of pharmacological agents and non-invasive, non-pharmacological interventions [7].
Music has been used extensively throughout history as a healing force to alleviate illness and distress [8]. The idea of music as a healing influence, which could affect health and behaviour is at least as old as the writings of Aristotle and Plato, when art, religion, and medicine still formed a unity and disease was viewed as an imbalance in harmony between a person’s physical and psychical nature. At that time music was thought to form the soul, put social life in order and heal man holistically, rather than simply entertain him. Though the origin of music itself is unknown, the fact that every civilization developed a different music history, identifiable in traditional music, indicates the strong impact music has always had on humans.
But it was not until the 20th century that music begun to be used more systematically, in the context of music therapy. By that time music was already used in hospitals mainly to boost morale, as a general aid to convalescence and as an entertaining diversion [9]. Nowadays music therapy is a recognized science of systematically applying music to support and encourage physical, mental, social and emotional well-being. Music is already used in general hospitals to alleviate patients’ mood and counteract depression, promote movement for physical rehabilitation, calm or sedate, often to induce sleep, and lessen muscle tension for the purpose of relaxation, including the autonomic nervous system [10].
Since the interest in complementary therapies has increased, the idea of using music to alleviate pain in conjunction with analgesia has been examined in the past, often combined with relaxation or guided imagery techniques. And, although health professionals frequently use music, in theatres for example, its potentialities are not widely spread. If music can indeed reduce pain, then this relatively cheap, non-pharmacological, easily applied intervention, with absolutely no side effects, becomes a useful tool for health professionals. This mini-review examines whether music reduces post-operative pain.
Methods
The population of interest is adult patients undergoing major elective surgery, under general anaesthesia, requiring post-operative pain relief, like Patient Controlled Analgesia (PCA) or opioid analgesic. The intervention is music, which is considered to be relaxing and calming, listened to through headphones so that external sounds will not interfere, either intra or post-operatively. Relaxing music is generally thought to be instrumental, with slow flowing rhythms that duplicate a pulse rate of 60-80 bpm [11]. The variety of timing and duration of the intervention between the studies is acknowledged as well as the potential for bias and error in interpretation, but as the intervention is music, ‘more music’ comparing to ‘less music’ will not make a significant difference. The outcome is post-operative pain experienced in the first 24 hours and day 1 after surgery Pain should be measured by appropriate instruments, like Visual Analogue Scale (VAS) and the amount of analgesia required.
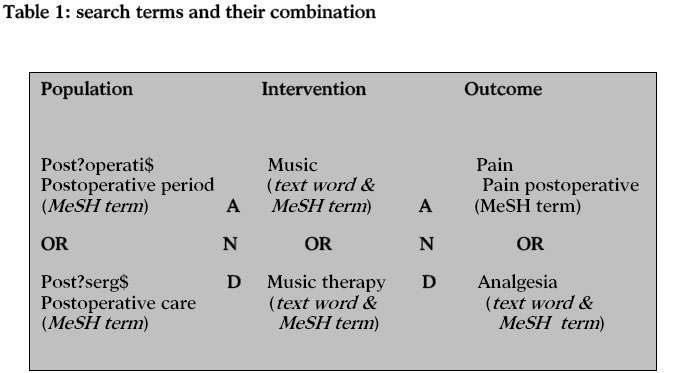
The type of research providing the best evidence to answer this question is randomized controlled trials, comparing listening to music with no intervention. Double blinding is not feasible, as a placebo cannot replace music, unless the intervention is applied during the operation. If this is not the case, lack of double blinding will not be considered as weakness of the study design. This mini review is also limited to studies available in English. The question was divided in facets, which identified the population (post-operative patients), the intervention (music) and the outcome (pain). Medline (1966-present), Embase (1980-present) and CINAHL were searched, using the following search terms in the combinations shown in Table 1: post?opetati$, post?surg$, music, music therapy, pain and analgesia. Wild card ($) was used to identify all word endings e.g. operative, operation. The MeSH terms used were ‘exploded’ to include all subheadings. The Cochran Library was also searched to identify any high quality systematic review on the subject.
Findings
The search strategy (table 1) found a total of 1631 articles. Exclusion criteria included review articles, studies with qualitative design, studies that did not include music in the interventions, and studies that used sounds instead of music and those who used combination of music with other methods such as relaxation. Titles and abstracts were examined for relevance to the review question, accessibility and English language. A total of 45 articles were excluded, as 9 were in foreign language, 15 not accessible and 19 irrelevant to the subject, either studying guided imagery techniques using music or factors reducing postoperative pain in general. Five of them were excluded, Koch et al., [12] and Shertzer et al., [13] because the population of the studies was different to the population of interest: in the first study subjects had spinal anaesthesia and in the second had day surgery not requiring post-operative pain relief. Good et al., [14] examined relaxation and music and their combination but the results reported did not mention each of the intervention group separately and no conclusions could be drawn for the music intervention. Heiser et al., [7] studied the use of music during the immediate postoperative recovery period in 34 patients and although the study design was excellent, the final sample size of 10 patients (5 in the treatment and 5 in the control group) decreased the power of the study while introduced great possibility of error in the results and therefore was not included in this review.
Six randomized controlled trials were retrieved and examined in further detail.
Methodological quality of included studies
One double-blinded controlled trial [15] and five randomized controlled trials [16-20] were analyzed using the critical appraisal checklist for articles describing randomized controlled trials [21]. Half of the included studies were performed by Nilsson et al [15,16,17]. All of them addressed a clearly focused question, though Good et al., [18] tested music and jaw relaxation in separate treatment groups as well as their combination. All studies were approved by local Ethics Committee, subjects’ informed consent was obtained and all provided full inclusion and exclusion criteria. Randomization was clearly described in all of the studies, mostly done by using a computer to generate randomization lists. Because of the type of intervention double blinding was not possible but in Nilsson’s et al., [15] study, when the intervention took place intra-operatively, while subjects were under general anesthesia. Subjects were treated equally and received the same type of premeditation, drugs for anaesthesia induction and maintenance, and immediate post-surgical analgesia within all trials. Post-operative analgesia was provided by patient-controlled analgesia with opioids (either ketomidone or morphine) in all trials and morphine equivalent was received via intravenous (IV) or intramuscular (IM) routes on request.
The music listened to was soothing relaxing music. Good et al., [18] offered a choice of different kinds of music: synthesizer, harp, piano, orchestral or slow jazz, to the treatment group. Nilsson et al., [15,16,17] used soft classical music reported to be relaxing and calming. Masuda et al., [19] used western classical music as well as traditional Chinese music and Laurion and Fetzer [20] piano music. Subjects in the control groups listened to either blank tape i.e. silence or they were exposed to operating theatre’s sounds. Subjects listened to the music from the time of arrival at the Post Anaesthesia Care Unit (PACU) [15-19] or intra-operatively without being conscious [16]. Pain intensity was estimated on Visual Analogue Scale (VAS), calibrated from 0=no pain to 10=maximal possible pain, every 30’16, every 60’ for the first 24 hours and every 3 hours during the 2nd day15 , every 15’ until the discharge from the PACU [18] or at a times agreeable to subjects [19]. The assessment was done during the intervention and on discharge in the study by Laurion and Fetzer [20]. Opioid intake was measured in all but two trials [18,19] and when not reported was checked before and after the data collection to make sure it did not affect the results.
In all studies statistical analysis (Kruskal-Wallis ANOVA) was used to test differences between the groups. There were no significant differences in the demographic data, anaesthetic and surgical factors between the groups. Confidence intervals were not provided in none of the studies.
Results
Nilsson et al., [16] tested music’s effects in 125 patients undergoing varicose vein or inguinal hernia repair surgery (table 2). Patients exposed to music from the time of arrival at the PACU and as long as they felt like it had significantly lower pain intensity postoperatively, compaired with patients in the control group (p-value<0.002), but not significant differences in postoperative morphine requirement (p-value<0.382). Postoperative anxiety, nausea, well-being, fatigue, urinary problems and headache, were also examined; no difference was found between the groups.
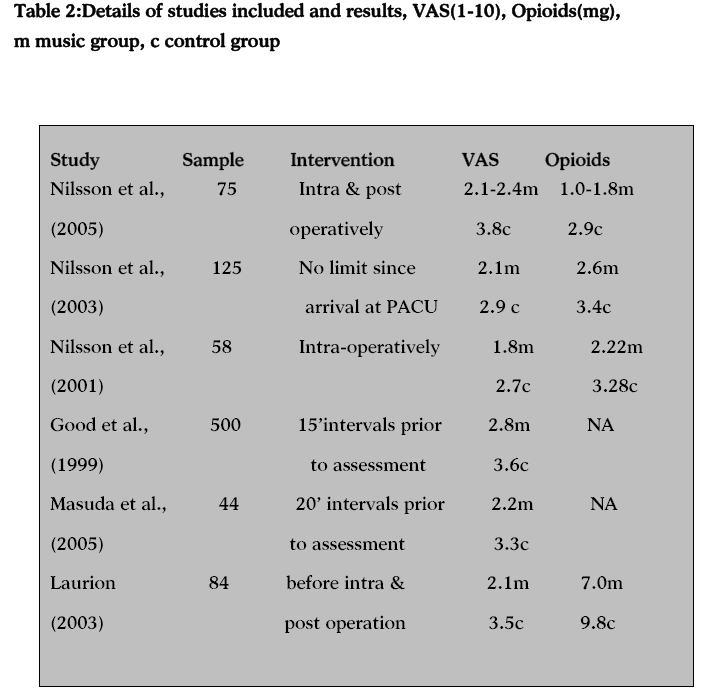
After intra-operative exposure to music, Nilsson et al., [15] found that 30 out of 58 patients undergoing elective abdominal hysterectomy had significantly less pain on the first day after surgery compared to the patients in the control group (p-value<0.001). It was also noted that the treatment group experienced less fatigue on the day of discharge and patients were mobilized significantly earlier. No differences were found between the groups regarding the total amount of ketomidone (p-value<0.057), nausea and well-being.
In another study Nilsson et al., [17] divided 75 patients undergoing open hernia repair as day care surgery in three groups: intra operative music, post operative music and silence. In addition to VAS data, the research team is also measuring stress markers such as cortisol and glucose blood levels. Indeed patients in the intra and post operative music groups had a significant decrease 45% in cortisol levels comparing with a 16% of the control group. After 1 hour in the PACU, the patients in both the post- and intra operative music groups had a significantly lower pain score compared with the control group, (p-value < 0.01) and the requirement of morphine was significantly less in the postoperative music group compared with the control group (p-value < 0.05).
Good et al., [18] noted that 233 patients after major abdominal surgery in the treatment group experienced significantly less pain than the control group (p-value<0.013). Differences in pain were supported by significantly lower radial pulse rate on day 2 and observed respiration rate. Opioid intake was not measured in this study.
The effects of music in postoperative orthopaedic pain were studied by Masuda et al., [19]. Forty four elderly patients divided in a group of music listening and a control group. After 20 minutes of listening to music the intervention group reported significantly lower VAS levels (p-value< 0.001) up to 79.1% compared with the control group where there was no significant change in the measures.
Finally Laurion and Fetzer [20] in their study of 84 laparoscopy gynae patients found in music group had significantly less pain on PACU discharge to home than the patients in the control group. The researchers in this study had the intervention group members to listen to the listened to the audiotape of piano music at least two times a day as well as during surgery and after surgery in the PACU. However the data collected an hour after surgery between the groups did not show a significant difference until the discharge measurements. However the methodological limitations influenced the strength of the study: there was no ability to control the number of times a subject actually listened to the interventional audiotapes before admission and piano music may be irritating to some individuals, thus, opening the pain gate pathways. There was no significant difference in the incidence of nausea or nausea and vomiting among the groups.
Discussion
The aim of this mini review was to find out whether music could reduce postoperative pain. The six studies included in the review showed significant difference between post-operative patients who listened to relaxing music and those who did not. Patients in the treatment groups experienced less pain compared with the control groups, regardless of the different ways intervention was operated. This review is limited in a number of ways. Foreign articles or the ones unobtainable in the time allowed should also have been accessed for assessment. The Journal of Music Therapy must have been also hand searched. The studies included performed the intervention differently, either during the operation, afterwards or in intervals, and with variations on the duration of music exposure. Although these variances should not be overlooked, the fact that music therapy as a science was developed the last century and therefore there is not much research around, justifies the reasons why the inclusion criteria concerning the intervention were flexible. Furthermore, music as a non pharmacological, side effect free intervention, would not ‘harm’ patients and less exposure to music could only result in non significant results, if no difference at all. The outcome pain was measured at different stages post-operatively, something that may introduce error in the analysis of the results. The inclusion of Nilsson’s et al., [16] trial where subjects had varicose vein and inguinal hernia surgery, unlike the abdominal surgeries the rest of the studies examined, may introduce error as well, but pain is quite objective in its context and reports regarding pain intensity after common surgical procedures have shown that pain can be a considerable problem [22].
This review has not been focused on what type of music is more beneficial or when is the most appropriate time for time exposure. Instead this search tried to answer if music has beneficial effect on postoperative pain in general and therefore it is difficult to draw any conclusion regarding the most effective timing for the intervention. In addition, the choice of music and the duration of the intervention are topics for further studies. Recovery after surgery has been focused on pharmacological interventions to minimize patient discomfort during the postoperative period. The results of this review suggest that music have some positive effects on postoperative recovery after surgery and support the idea of using music, a non-pharmacological intervention along with analgesic medication to reduce pain.
The mechanism of this effect can probably be best explained by the gate control theory: the perception of pain is decreased via ‘gates’, which are numerous and diverse points of filtration, abstraction and modulation of noxious input in the central nervous system. The gates are influenced by emotional and cognitive factors through descending inhibition systems [23]. The effect may occur through distraction, reduction of tension and sympathetic modulation [24]. When music distracts the mind, the result is selective attention mediated by thalamus that alerts the prefrontal cortex to the sound rather to the painful input [25] causing pain inhibition [26]. Soothing music reduce muscular and mental tension and thereby, reduce sympathetic stimulation of the hypothalamus [27] which activates endogenous opiates in the central nervous system, reducing propagation of pain impulses and modulating perceptions of the sensory and affective components of pain [28].
According to these results, taped music should be offered to surgical patients because the technique is inexpensive, non-pharmacological and non-invasive with beneficial effects. Patients should be encouraged to listen to music preoperatively to reduce stress as well as postoperatively, for as long as they like, since there are no side effects. Henry [29] states that the optimal duration for listening to music is not known but recommends a listening time of 25-90 min. The use of headphones would also screen some of the PACU noises generated from staff and equipment, increasing patient satisfaction [7].
But what would be the most appropriate kind of music to listen to? Some music therapists suggest that classical music is the best music for relaxation because of its consistent tone and form [8] but there are studies showing that musical preferences play a large role in decreasing anxiety for surgical patients [30]. In practice, patients scheduled for elective surgery could either bring with them the kind of music that is relaxing for them, or choose from a small variety provided by hospitals. This procedure may sound time-consuming for health professionals, but could definitely fit in the time spent to explain the operation to the patient and consent them, for the benefits of music are undoubted.
Music’s ability to comfort human body and soul has been known for centuries and has been used in medicine in an amateurish and rather mystical kind of way, until music therapy was placed alongside with other complementary therapies and started exploring the benefits of music as a therapy more systematically. Nowadays, although music therapy has been around as a science for the last 60 years, little is known about music’s merits and music therapy is still treated with skepticism. However, research activity taken by health professionals who believe in music’s advantages, is starting to spread the idea of using music as a therapeutic tool in general.
The findings of his review suggest that music reduces postoperative pain, but not the amount of opioid intake after surgery. In view of this fact and having in mind that music is a non-pharmacological, easy, inexpensive, non-invasive intervention, the use of music perioperatively is highly recommended to reduce anxiety, stress and reduce pain after surgery.
3212
References
- International Association for the Study of Pain. Pain Terms: A List with Definitions and Notes on Usage. Recommended by the IASP Subcommittee on Taxonomy. Pain 1979;6:249.
- Acute Pain Management Guideline Panel, Acute pain management: operative or medical procedures and trauma: Clinical practice guideline (AHCPR No. 92-0032), Agency for Health Care Policy and Research, Public Health Service, U.S. Department of Health and Human Services, Rockville, MD,1992.
- Bushnell MC, Duncan GH, Hofbauer RK, Ha B, Chen JI, Carrier B. Pain perception: Is there a role for primary somatosensory cortex? Proceedings of the National Academy of Sciences of the United States of America, 1999; 96 : 7705–7709.
- American Medical Association. Pain management: Pathophysiology of pain and pain assessment. (2003)Retrieved January 21, 2008, from https://www.ama-cmeonline.com/pain_mgmt/module01/index.htm.
- Good M, Anderson GC, Stanton-Hicks M, Grass JA, Makki M. Relaxation and music reduce pain after gynaecologic surgery. Pain Manag Nurs 2002;3 : 61–70
- Good M, Anderson GC, Ahn S, Cong X, Stanton -Hicks M. Relaxation and music reduce pain following intestinal surgery. Res Nurs Health 2005; 28 : 240–25.
- Heiser R, Chiles K, Fudge M, Gray SE. The use of music during the immediate postoperative recovery period. AORN J 1997; 65 :777–785.
- Gerdner LA, Buckwalter KC. Music therapy. In: (ed 3 ed.),GM Bulechek and JC McCloskey, Editors, Nursing Interventions. Effective Nursing Treatments, Saunders, Philadelphia, 1999.
- Watkins GR. Music therapy: Proposed physiological mechanisms and clinical implications. Clin Nurs Spec 1998;11 : 43–50.
- Chlan L. Effectiveness of music therapy intervention on relaxation and anxiety of patients receiving ventilator assistance. Heart and Lung 1998; 27 (3):169–176.
- Koch ME, Kain ZN, Ayoub C, Rosenbaum SH. The sedative and analgesic sparing effect of music. Anaesthesiology 1998;89: 300–306.
- Shertzer KA, Keck JF. Music and the PACU environment. J Perianesth Nurs 2001;16 : 90–102.
- Good M, Stanton-Hicks M, Grass J, Anderson G, Makii M, Geras J. Pain following gynaecological surgery. Pain Management Nursing 2000;1(3):96-104.
- Nilsson U, Rawal N, Uneståhl LE, Zetterberg C, Unosson M. Improved recovery after music and therapeutic suggestions during general anaesthesia: A double-blind randomized controlled trial. Acta Anaesthesiol Scand 2001;45: 812–817.
- Nilsson U, Rawal N, Engqvist B. Unosson M. Analgesia following music and therapeutic suggestions in the PACU in ambulatory surgery; a randomized controlled trial. Acta Anaesthesiol Scand 2003; 47 : 278–283.
- Nilsson U, Unosson M, Rawal N. Stress reduction and analgesia in patients exposed to calming music postoperatively: A randomized controlled trial. Eur J Anaesthesiol 2005; 22 : 96–102.
- Good M, Stanton-Hicks M, Grass JA. Cranston Anderson G, Choi C, Schoolmeesters LJ, Salman A. Relief of postoperative pain with jaw relaxation, music and their combination. Pain 1999; 81: 163–172.
- Masuda T, Miyamoto K, Shimizu K. Effects of music listening on elderly orthopeadic patients during postoperative bed rest. Nordic J Music Ther 2005;14: 4–14.
- Laurion S, Fetzer SJ. The effect of two nursing interventions on the postoperative outcomes of gynecologic laparoscopic patients. J Perianesth Nurs 2003;18 : 254–261.
- Greenhalgh T. How to read a paper: the basics of evidence based medicine BMJ books, Blackwell publishing, London, 2006.
- Gilbert HC. Pain relief methods in the postanesthesia care unit. J Post Anesth Nurs 1990;5: 6–15.
- Melzack R. Pain and the Neuromatrix in the brain. J Dent Educ 2001;65: 1378–1382.
- Mac Lellan K. Postoperative pain: Strategy for improving patient experiences, Journal of Advanced Nursing 2004;46: 179–185.
- Wong HL, Lopez-Nahas V, Molassiotis A. Effects of Music Therapy on Anxiety in Ventilator-dependent Patients. Heart & Lung, 2001;30 :376-87.
- Mok E, Wong K Y. Effects of Music on Patient Anxiety. AORN Journal, 2003; 77: 396-7,401-6,409-10.
- Melzack R. The short-form McGill Pain Questionnaire. Pain 1987;30: 191–197.
- Evans MM, Rubino PA. Music: A diversionary therapy. Todays OR Nurse. 1994;16(4):17-22.
- Henry LL. Music therapy: A nursing intervention for the control of pain and anxiety in the ICU: A review of the research literature. Dimens Crit Care Nurs 1995;14 : 95–304.
- McCaffrey R, Locsin RC. Music listening as a nursing intervention: a symphony of practice. Holist Nurs Pract 2002;16(3):70-7.

