Keywords
Elderly; Physical fitness; Primary health care
Introduction
Although the right to health has been spread worldwide since the creation of the World Health Organization (WHO) in 1948, only forty years later Brazil has formally recognized health as a social right [1]. It was from the Federal Constitution of 1988 that occurred the consolidation in previous decades there is a priority health system called the Unified Health System (Sistema Único de Saúde, SUS), which had great importance for Brazilian society [2]. With the Federal Constitution of 1988, the Health came to be recognized as a social right, being inherent to the condition of the citizen, where it would be up to the government to guarantee it: “Health as a right of all and duty of the State” [1].
Four years later the Ministry of Health (Ministério da Saúde, MS) creates the Family Health Program (Programa de Saúde da Família, PSF) [3] which later becomes the Family Health Strategy (Estratégia de Saúde da Família, ESF), which takes on a reorganized role of care practice, providing a new dynamic in health services. Health by creating a relationship with the community, working in a multidisciplinary way, bringing access to health services for the whole population, especially the elderly, improving the quality of life and social life of individuals [4].
In this perspective of increasing the resolution capacity of the population's health problems, the Ministry of Health created the Family Health Support Centers (Núcleos de Apoio à Saúde da Família, NASF's), through Ordinance Nº 154, of January 24, 2008, which come as a strategic complement to improve the actions of Primary Health Care, since NASF works in a multidisciplinary way through the sharing of knowledge, further expanding the ability to solve the health problems of the entire population, emphasizing the elderly public [5].
Thinking about this accelerated growth of the elderly population, the National Elderly Policy was regulated in 1996, guaranteeing social rights to the elderly ensuring conditions for the improvement of functional autonomy through physical exercise practices. Through Ministerial Ordinance Nº. 1395, the National Health Policy of the Elderly is created, stating that the main problem that affects the elderly is the loss of functional capacity, and the loss of performing functions related to the basic activities of daily life, triggering the functional dependence of these individuals [6].
Gobbi [7] and Bocalini [8] state that one of the main factors to prevent or minimize most of the physical, psychological and social declines that escort the elderly is the practice of physical exercise, as it delays the loss of functional capacity providing a good condition. As well as controlling stress, obesity, diabetes, coronary heart disease and, especially, maintaining an active lifestyle. Thus, the inclusion of the elderly in systematized physical activity programs, with or without multiprofessional support, involving work of strength, flexibility, agility, aerobic endurance and coordination, is essential to promote autonomy and functional independence, enabling the elderly perform their basic activities of daily living, minimizing the risk of developing diseases that may lead to addiction [9].
In the studied literature, we did not identify studies that have compared the physical fitness of the elderly attended by multiprofessional groups belonging to the family health teams, having these elderly participated in joint or isolated interventions. However, multiprofessional intervention is a methodology advocated by the SUS single health system, is represented by the Family Health Support Centers (NASF's). Thus, this research may present valuable information that supports multiprofessional practice across all specialties developed by NASF. Given this context, the objective of this study was to verify the effect of a multiprofessional intervention program combined with physical exercise in the elderly attended by the Family Health Program. Given this conjuncture, it is believed that specialized multiprofessional care can promote effective results for the functional health of elderly users assisted by NAF's teams, compared to individualized care methodologies.
Methods
Type of study methods
The study is characterized as a randomized clinical, conducted in two family health units (unidades de saude da família, USF), located in the city of Vitoria de Santo Antao, in the state of Pernambuco, Brazil, from February to April 2017.
Study design sample
Initially, a draw was made from family health units (USF). Of the four units located in the urban area of the municipality attended by the Family Health Support Center (NASF), two units were selected because they are those with greater adherence and community participation. After selection, a randomization was made for the allocation of individuals in the experimental group G1 (exercises+multiprofessional intervention) and G2 (exercise only). The sample consisted of 30 low-income elderly of both sexes aged 60 years and older, those with no mobility impairment, those who had not practiced regular exercise for at least three months, and the volunteers who dropped out were excluded to attend or not attend a minimum of 75% of the intervention period. Considering that the participation in each group of coexistence, respecting the place of formation of each group, it was not possible to allocate the participants in a randomized way. Similarly, and for the same reason, an intentionto- treat analysis could not be performed. Thus, the selection and maintenance of the entire final study sample occurred for convenience. The research was approved by the Research Ethics Committee Involving Human Beings of the Health Sciences Center of the Federal University of Pernambuco, CEP/CCS/UFPE, under the opinion nº 1.873.522.
Multiprofessional advisory teams
Group G1 received the support of the professionals who make up the Family Health Support Center (NASF). These professionals worked freely through themes from the community itself, as recommended by the Primary Care Booklet No. 39 [5]. The physiotherapy professional worked on the following topics: Importance of wearing shoes during physical activity, importance of physical activity to improve macha and importance of physical activity to improve dynamic balance, in order to prevent falls, because according to National Health Policy for the Elderly [6]. One of the problems that most affects the elderly is the loss of functions related to the basic activities of daily living; The nutritionist worked on the following topics: diet and diabetes mellitus, diet and hypertension, and diet and obesity, since poor diet is the gateway to the emergence of non-communicable chronic diseases; The psychologist worked on the following subjects: physical activity and memory, physical activity and sleep, and physical activity and depression, as systematic exercise, minimizes the process of decline in physical and cognitive functions; The speech therapist worked on the following contents: physical activity and hydration, physical activity and breathing and vocal abuse, since these factors are related to the improvement of performance during physical exercise. During the three months of intervention, the professionals mentioned above worked in the form of conversation and dynamics wheels in groups acting at the beginning, middle or end of physical activity practice. The average duration of these interventions was 20 minutes.
Intervention with exercises
Group G1 and G2 received the same exercise intervention during the research period. The exercise intervention was performed by two previously trained physical education professionals to ensure their objectivity. The training program consisted of strength, flexibility, agility, dynamic balance and aerobic exercises, the exercises were performed in a circuit form using the following instruments: agility ladder, dumbbells, cones, elastic resistance extender, chairs and Chinese hat. In both groups, the exercise program was performed once a week, lasting 60 minutes over a period of 12 weeks. The program consisted of 10 to 15 minutes of walking aiming at improving aerobic fitness, exercises performed with one's own body and with alternative materials, aiming at improving upper and lower limb strength and dynamic balance, lasting 30 to 35 minutes, ending with stretching exercises to improve flexibility, lasting 10 to 15 minutes. A summary of the exercise sequence is presented in Table 1.
Table 1 The sequence of the exercises performed by the elderly participants of the study is presented.
| Exercise Sequence |
Duration |
| Light to moderate intensity walking |
10 a 15 min |
| Dumbbell alternante thread |
|
| Threaded hammer with dumbbells |
|
| Direct thread with elastic extender |
|
| Triceps kick with thera band |
|
| Unilateral triceps with thera band |
|
| Horizontal row with thera band |
|
| Inverted crucifix with thera band |
|
| Dumbbell Squats |
30 a 35 min |
| Dynamic squat without dumbbells in the chair |
|
| Isometric Squats |
|
| Advance |
|
| Walks on obstacles |
|
| Agility Ladder |
|
| Arm Extension |
10 a 15 min |
| Wrist extension and flexion |
|
| Lateral trunk flexion |
|
| Frontal trunk flexion |
|
| Leg extension and flexion |
|
| Back flexion and plantar ankle flexion |
|
Demographic data
Both groups were submitted to a sociodemographic questionnaire, based on the criteria of the Getulio Vargas Foundation Social Policy Center (CPS/FGV) [10], in order to characterize the sample containing the following items: health status, education, income, age and sex.
Assessment of functional fitness
They were applied to the test battery, Senior Fitness Test initially developed and validated for the elderly in the United States by researchers Jones and Rikli [11]. This battery measures the physical fitness of the elderly to perform the activities of daily living and consists of six tests that assess strength. Upper and lower limbs MMSS, lower limb (arm lift and sit, arm flexion) upper and lower limb flexibility MMSS, lower limb (hands-on back, sit and reach) agility and dynamic balance (come and go) and aerobic endurance (6-minute walk). Therefore, this battery was widespread and used in different countries, including Brazil. In this regard, Marques et al. [12] developed the normative values that classify the level of physical fitness of elderly Brazilians.
Statistical analysis
Data were stored in a double-typed Excel database and analyzed using descriptive statistics. The results were presented through tables, graphs with the crossing of the main and secondary variables in absolute and relative values.
Normality assumptions were analyzed using the Shapiro-Wilk test. Then, the groups were compared by means of independent means comparison tests (unpaired t-test), to verify if the multiprofessional care potentiated benefits to the functional aptitude of the elderly assisted by the NASF team. In addition, the power of the analyzes and the effect size were performed to verify the impact of the results obtained using the cutoff points established by Alves et al. [13] and calculated using the G* Power Software, version 3.1. 2 (Franz Faul, Dusseldorf, ALE). All descriptive and inferential analyzes were performed using Prism software, version 6.0 (Graphpad, USA). The significance level established was 5% (p<0.05).
Results
A total of 30 individuals entered the physical exercise program under the guidance of a physical education professional between February and April 2017. Of these, only 23 met the inclusion criteria and underwent testing, and after data analysis, It was observed that the age of the analyzed elderly ranged from 60 to 80 years or older and had an arithmetic average of 68.56. Regarding the socio-economic profile of the sample, it varied from class C to class E, with Class E being more prevalent, with income between R $ 0.00 and R $ 1.085.00 in relation to education. Most individuals in both groups were literate (Table 2). After three months of activity, significant changes were observed in almost all domains in the group that received multiprofessional support, G1, (Figure 1).
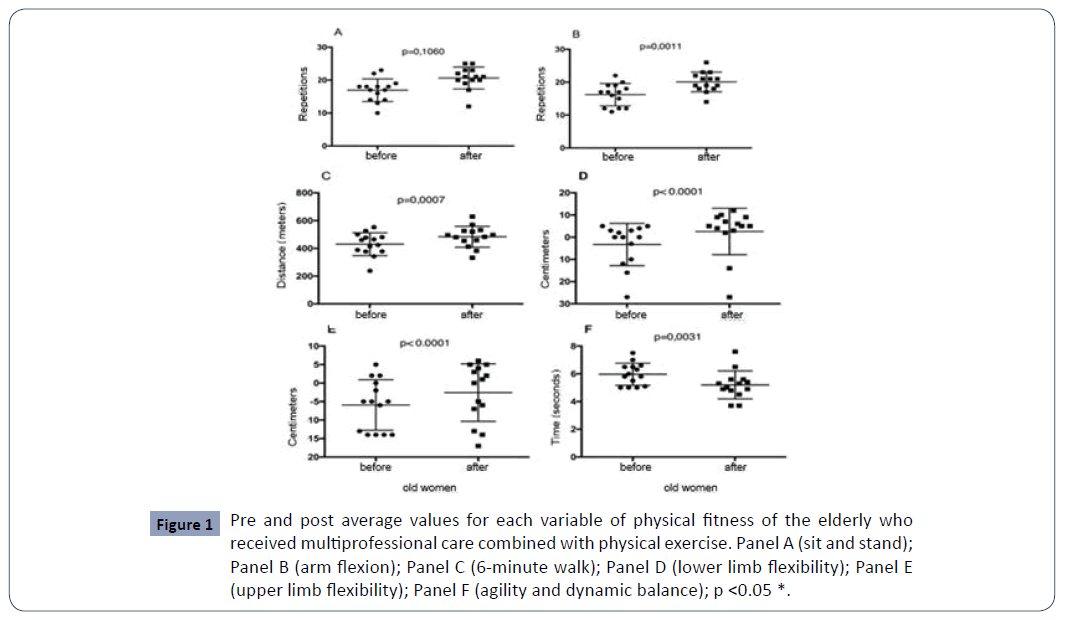
Figure 1: Pre and post average values for each variable of physical fitness of the elderly who received multiprofessional care combined with physical exercise. Panel A (sit and stand); Panel B (arm flexion); Panel C (6-minute walk); Panel D (lower limb flexibility); Panel E (upper limb flexibility); Panel F (agility and dynamic balance); p <0.05 *.
Table 2 Descriptive data of elderly study participants.
| |
Multiprofessional Group (n=14) |
Isolated Group (n=9) |
| Age |
|
|
| 60 -69 |
08 |
05 |
| 70 -79 |
06 |
03 |
| 80 years or older |
00 |
01 |
| Body mass (kg) |
|
|
| Average |
67,80 |
66,98 |
| Stature |
|
|
| Average |
1,50 |
1,56 |
| BMI |
|
|
| Average |
30,12 |
27,19 |
| Genre (n) |
|
|
| Men |
03 (21.4%) |
05 (55.6%) |
| Women |
11 (78.6%) |
04 (44.4%) |
| Family income (n) |
|
|
| 1 minimum wage |
10 (71.5%) |
06 (67%) |
| More than 1 minimum wage |
04 (28.5%) |
03 (33%) |
| Education (n) |
|
|
| Literate |
12 (86%) |
07 (78%) |
| Not literate |
02 (14%) |
02 (22%) |
Similarly, the group (G2) signaled significant improvements for almost all functional capacities, thus showing that physical exercise alone or with multidisciplinary support is a potent instrument to improve individuals' quality of life, autonomy and functional independence (Figure 2). Analyzing the data on effect size, significant results were observed Alves et al. [13] for sitting and standing (ET=0.6060), arm flexion (ET=1.050), 6-minute walk (ET=0.0137), lower limb flexibility (TE=0.566), upper limb flexibility (0.181), agility and dynamic balance (TE=0.143).
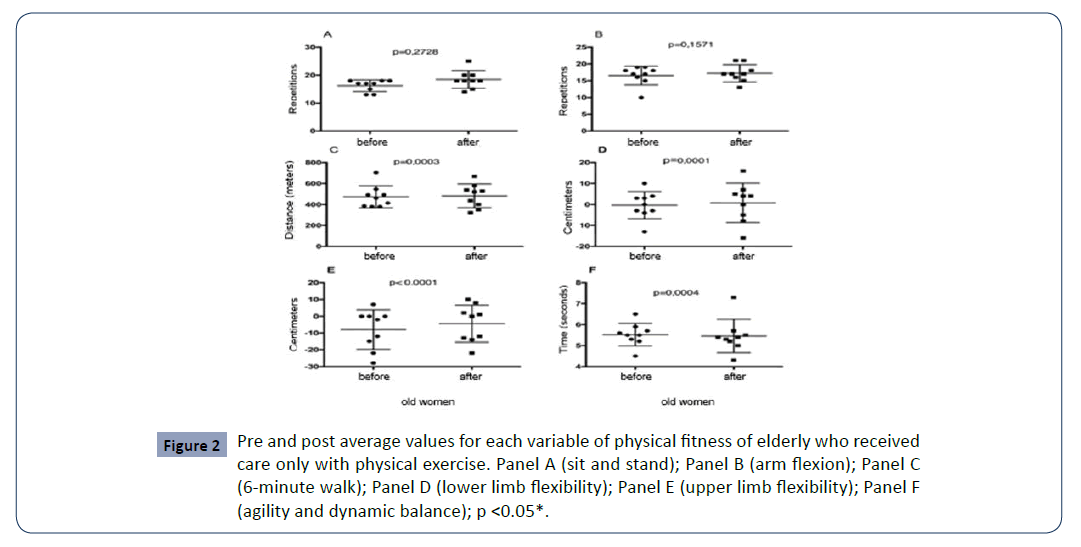
Figure 2: Pre and post average values for each variable of physical fitness of elderly who received care only with physical exercise. Panel A (sit and stand); Panel B (arm flexion); Panel C (6-minute walk); Panel D (lower limb flexibility); Panel E (upper limb flexibility); Panel F (agility and dynamic balance); p <0.05*.
Discussion
The aim of the present study was to verify the effect of a multiprofessional intervention program combined with physical exercises in the elderly attended by the Family Health Program, having these elderly participated in joint or isolated interventions, if it would show any benefit regarding the improvement of the functional capacities, after regular exercise.
For this analysis, the Senior Fitness Test battery was used, which measured the physical fitness of the elderly before and after insertion in a physical activity program. After analysis, significant changes were observed in the functional capacities of the elderly, indicating that the practice of physical exercise together with a multidisciplinary care can be a predictor of improvement in quality of life.
As in most of the best age groups, the prevalence of women was observed. In a study conducted at USP at the physical education school in 2009, researchers obtained the participation of 74% of women [14], similar values to the findings in this research. This phenomenon may be linked to the higher prevalence of women in the Brazilian population. In addition, it is worth remembering that women are more health-conscious than men, more easily adhering to physical activity programs where they have the possibility to improve their physical abilities, as well as promoting social interaction [15].
A determining factor for physical exercise during old age is the improvement or maintenance of functional capacities, since there are several adaptations resulting from the practice of regular exercise, the National Health Policy of the Elderly recommends in its guidelines the promotion of active and healthy aging through physical activity practices [6].
The income of the elderly in this study corroborates the data from Brazil, where 12.4% of the population live with up to half a minimum wage [16]. If we highlight the absolute values of the elderly in poverty, it can be observed that most of them live in the states. Bahia (334 thousand), Minas Gerais (268 thousand) and São Paulo (248 thousand) [16].
Among the investigated elderly, a complete and incomplete elementary school education prevailed, leading us to predict that access to education in the past was quite difficult. For health education activities it is necessary to take into account the level of education, as it can be in fact one of the influencing agents in the process of understanding, interpretation, and application of written or spoken health information. In addition to a strong link between loss of functional capacity and low education according to [17].
In the literature studied, we did not identify any study with a methodology identical to ours that compared the physical fitness of the elderly assisted by multiprofessional groups belonging to family health teams, having participated in joint or isolated interventions. This made comparative analysis of our results difficult.
In the first test applied (sitting and standing) we tried to verify basically the strength of the lower limbs, and we can observe that there was no significant improvement in both groups. Our results do not resemble the findings in the literature Frontera et al [18] that found a 227% strength gain after a 12-week period [19] and Hicks et al [20] also found an increase in strength in older men and women who did strength training. 12 to 26 weeks.
The arm flexion that seeks to verify the strength of the upper limbs, we can verify that only in the group (G2) there were no significant improvements. The results of this study corroborate those of Cipriani et al [21], who, after ten months of a physical activity program aiming at analyzing the General Functional Fitness Index (IAFG), also found no significant improvement in upper limb strength. However, it is worth mentioning the importance of maintaining these variables during the study period, which may already be a positive point in the face of the aging process.
Strength training depends on the adjustment of variables, such as the number of repetitions, series, overload, intensity, volume, sequence, and intervals between sets and exercises [22]. Therefore, we understand that the fact that no significant differences were identified in the lower limb strength variable in both groups and upper limb strength in the group (G2) could be related to the fact that there was no strict control regarding all the variables that compose strength training.
The sit and reach test accurately measure the flexibility of the lower limbs. In our research, the elderly began to perform the test with less autonomy, in contrast to the findings by Hoerger and Hopkins [23] where after a stretching, walking and dancing program with the elderly for 12 weeks, they also obtained a significant result in the test.
Reaching behind the back measures the general movement of the shoulder girdle, adduction, abduction, internal rotation and external rotation of the shoulder; In our study, we obtained inferior results after the training period. Hubley, Wall and Hogan [24] found that after the elderly participated in a regular exercise program, they had significant improvement in all joint segments. From 65 years of age onwards, the process of osteoarticular deterioration occurs, and through a systematized physical exercise program, a good range of motion can be achieved, representing an important gain in the quality of life of these Shepard individuals [25].
We believe that the lower results in relation to the flexibility components (upper and lower limbs) were caused by the lower stimulus during the exercise program compared to the other trained fitness components. Additionally, it has been found that increases in muscle strength and endurance may negatively influence flexibility gains in older people Rebelatto Jr et al. [26], Ueno et al. [27].
The ability to come and go assesses agility and dynamic balance; our findings were significant for both groups [28] and found significant improvements in the balance of the elderly after performing a 10-week training program. Hoerger and Hopkins [23] obtained a 12% increase in the mobility of the elderly undergoing a 12-week exercise program.
The 6-minute walk measures cardiorespiratory capacity, an important ability for individuals to perform their basic activities of daily living or instrumental of daily living. We observed a significant increase in the cardiorespiratory capacity of the elderly participants of our training program, corroborating the findings of Matsudo, Matsudo, and Barros Neto [29] who after an exercise program observed an improvement of 10 to 40%, mainly due to the increase in the arteriovenous difference. Oxygen, systolic volume, cardiac output, plasma, and blood volume.
Although we were able to carry out the training program in a short period of time, three months, it was possible to observe significant changes in almost all results, as in the literature there are few studies comparing the improvement of functional capacities with multiprofessional care. Further studies are needed to analyze the possible variables that influence the loss of functional capacities that accompany the elderly. Matsudo et al [29] admit that the effects of a strength training program for the elderly are slightly lost with the suspension of activities, reaching a percentage of 32% after 4 weeks without training.
The decrease in physical fitness resulting from the process of senescence is a relentless fact, which begins gradually, from the age of fifty. However, several other studies, such as ours, point to the benefits of exercise programs for the elderly as a preventive measure to postpone the effects of aging on physical fitness as much as possible Matsudo et al. [29] and Zenker [30].
Conclusion
The present study identified significant improvements in almost all functional abilities of the elderly, during 03 months of participation in a systematized physical activity program with multiprofessional or isolated support, with 6-minute walking, arm flexibility, agility, and dynamic balance were the variables that had significant and positive changes.
We can see that a systematized physical activity program with multiprofessional support or isolation contributed significantly to the improvement of the functional capacities of the elderly, consequently providing a better quality of life and functional independence. However, it is necessary to verify other possible variables that may be related to the loss of functional capacity that accompanies the elderly, since the decrease in physical fitness due to the aging process has a multifactorial cause.
31014
References
- Paim, Silva J (2009) An analysis of the Brazilian Health Reform process. Health Debate 33: 27-37.
- Brasil (1988) Constitution of the Federative Republic of Brazil. Text promulgated on 10/05/1988.
- Brasil (2014) Family Health Support Center - Volume 1: Tools for management and daily work.
- Brasil (2006) Official Gazette of the Federative Republic of Brazil, Brasília, section 1, n ° 237-E, 20-24.
- Gobbi S (1997) Physical Activity for Elderly People and Recommendations of the 1996. Brazilian Journal of Physical Activity & Health 2: 41-49.
- Bocalini DS, Santos L dos, Serra AJ (2008) Physical exercise improves the functional capacity and quality of life in patients with heart failure. Clinics 63: 437-442.
- Nakamura Y, Tanaka K, Yabuschita N, Sakai T, Shigematsu R (2007) Effects of exercise frequency on functional fitness in older adult women. Archives Gerontology Geriatrics 44: 163-173.
- The New Middle Class: the bright side of the poor, Center for Social Policies, FGV, Rio de Janeiro, mimeo.
- Rikli RE, Jones JC (2001) Development and validation of a functional fitness test for community residing older adults. Journal of Aging Physical Activity 7: 129-161.
- Marques EA, Baptista F, Santos R, Vale S, Santos DA, et al. (2014) Normative functional fitness Standards and trends of Portuguese older adults: cross-cultural comparisons. Journal of Aging Physical Activity 22: 126-137.
- Alves RV, Mota J, Costa MC, Alves JGB (2004) Physical fitness related to the health of the elderly: influence of water aerobics. Brazilian Journal of Sports Medicine 10: 31-37.
- Pereira JRP, Okuma S (2009) The profile of those entering a physical education program for the elderly and the reasons for their initial adherence. Brazilian Journal of Physical Education and Sport 23: 319-334.
- Goggio NL, Morrow JJR (2001) Physical activity, behaviours of older adults. Journal of Aging and Physical Activity 9: 58-66.
- Brazilian Institute of Geography and Statistics (2008) Synthesis of social indicators: an analysis of the living conditions of the Brazilian population: 2008/IBGE, Coordination of Population and Social Indicators.
- Almeida MHM, Litvoc J, Perez MP (2012) Difficulties for basic and instrumental activities of daily living, reported by users of a School Health Center in São Paulo. Brazilian Journal of Geriatrics and Gerontology 15: 187-200.
- Frontera WR, Meredith CN, O’Reilly KP, Evans WJ (1990) Strength training and determinants of VO2 max in older man. Journal Applied Physiol 68: 329-333.
- Hagber JM, Graves JE, Limacher M, Woods DR, Leggett SH, et al. (1989) Cardiovascular response of 70 to 79 -year old men and women to exercise training. Journal Applied Physiol 66: 2589-2594.
- Hicks AL, Cupido CM, Martins A, Dent A (1991) Twitch potentiation during fatiguing exercise in the elderly: the effects of training. European Journal of Applied Physiology and Occupational Physiology 63: 278-281.
- Cipriani NCS, Meurer ST, Beneditti TRB, Lopes MA (2010) Functional fitness of elderly women who practice physical activities. Brazilian Journal of Cineanthropometry & Human Performance 12: 106-111.
- Silva NLD, Farinatti PTV (2007Influence of counter-resistance training variables on muscle strength in the elderly: a systematic review with an emphasis on dose-response relationships. Brazilian Journal of Sports Medicine 13: 60-66.
- Hoerger WW, Hopkins DR (1992) A comparison of sit and the modified sit and reach in the measurement of flexibility in woman. Research Quarterly for Exercise Sport 63: 191-195.
- Hubley KCL, Wall DR, Hogan DB (1995) Effects of a general exercise program on passive hip, knee, and ankle range of motion of older women. Topics Geriatric Rehabilitation 10: 33-44.
- Shepard RJ (1997) Aging, physical activity, and health. Champaign, Illinois: Human Kinetics.
- Rebelatto JR, Calvo JI, Orejuela JR, Portillo JC (2006) Influence of a long-term physical activity program on hand muscle strength and body flexibility among elderly women. Brazilian Journal of Physical Therapy 10: 127-132.
- Ueno LM, Okuma SS, Miranda LL, Filho WJ, Ho LL (2000) Analysis of the Quantitative and Qualitative Effects of a Physical Education Program on Hip Flexibility in Individuals Over 60. Driving 6: 9-16.
- Lord SR, Castell S (1994) Physical activity program for older persons: effect on balance, strength, neuromuscular control, and reaction time. Archives of Physical Medicine Rehabilitation 75: 648-652.
- Matsudo SM, Matsudo VKR, Neto TLB (2000) Impact of aging on anthropometric, neuromotor and metabolic variables of physical fitness. Brazilian Journal of Science and Movement 8: 21-32.
- Zenker TK (1996) Physical fitness in the elderly. Rehabilitation 35: 233-236.

