Dewi Marhaeni Diah Herawati1*, Siti Nur Asiyah2, Siska Wiramihardja1, Shellita Melanie3, Deni Kurniadi Sunjaya4 and Dida Akkad Gurnida5
1Department of Public Health, Division of Medical Nutrition, Faculty of Medicine, Padjadjaran University, Indonesia
2Sumedang District Health Office, Indonesia
3Magister Programme of Basic Medical Science, Faculty of Medicine, Padjadjaran University, Indonesia
4Department of Public Health, Division of Public Health, Faculty of Medicine, Padjadjaran University, Indonesia
5Department of Pediatrics, Faculty of Medicine, Padjadjaran University, Indonesia
*Corresponding Author:
Dewi Marhaeni Diah Herawati
Department of Public Health, Division of Medical Nutrition
Faculty of Medicine, Padjadjaran University, Indonesia
Tel: +6281222242030
E-mail: dewimdh@yahoo.com; marhaeni@unpad.ac.id
Received Date: 22 September 2018; Accepted Date: 05 October 2018; Published Date: 15 October 2018
Citation: Herawati DMD, Asiyah SN, Wiramihardja S, Melanie S, Sunjaya DK, et al. (2018) Effects of Supplementation of Anguilla Biscuit on Under Five Years Old with Underweight in Sumedang District, Indonesia: A Randomized Control Trial. Health Sci J Vol.12.No.5:594.
Copyright: © 2018 Herawati DMD, et al. This is an open-access article distributed under the terms of the creative commons attribution license, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
DOI: 10.21767/1791-809X.1000594
Keywords
Anguilla biscuit; Nutritional improvement; Underweight in under five years old
Introduction
Currently, approximately 6.3 million of children less than five years old died every year, which is malnutrition was one of the causes [1]. World Health Organization data in 2017 showed that about 31.4%, or 16 million of 51 million children under five years old was malnourished [2]. Malnutrition still remains major health problem of children under five years old in developing countries, including Sub-Saharan Africa and Indonesia [3,4]. According to the latest data from National Health Research in Indonesia, the prevalence of children with malnutrition was as high as 19.6% [4].
One of the clinical manifestation of malnutrition was underweight which could lead to delayed physical growth, undeveloped intellectual intelligence, behavioral problems and impaired social skills [5]. If this condition was not thoroughly treated, severe malnutrition condition, susceptibility to infectious disease, increasing morbidity and mortality rate were unavoidable [6,7]. Approximately, 20 million children were in severe malnutrition condition and 1-2 million among them were dead every year [7].
United Nation has been established The Sustainable Development Goals (SDGs) program which is one of the main targets was to improve community nutrition by 2030 to address malnutrition problems. Some indicators of the program are to reduce the prevalence of malnutrition and energy deficiency rate in children under five years old [8]. In accordance to the program, Indonesia established nutritional improvement program for society as health sector priority in Indonesian Long Term Development Plan 2005-2025 [9]. Inadequate quantity and quality of food intake is one of the causative factors of malnutrition in children under five years old. Insufficiency of food intake could lead immunity deficiency which effect susceptibility of illness. This condition could worsen appetite and absorption of nutrition, thus, aggravating malnourished condition of children [10]. Fortified food could increase the quality of nutrition and support children growth and development [11]. Intervention using supplementary food was beneficial to provide adequate nutrition and improve health status of the children. However, supplementary food should contain the most needed and important nutrition for children growth and development [12].
Certain research reported that food supplementation in the form of RUTF (Ready to Use Therapeutic Food) to the children with underweight could improve their nutritional status [13-17]. RUTF was lipid peanut paste which resistant to bacterial contamination, contain less water, no need to be cooked, energy-rich content, which is 23 calorie/gram, and met the requirement for standard composition for therapeutic food established by WHO [18]. RUTF was only given for short period of time to the children under five years old who suffered SAM (Severe Acute Malnutrition). It did not have complication and had sufficient appetite [19].
Supplementary food program for children under five years old with underweight in Indonesia was administered in a specifically-designed biscuits which contain energy of 253-300 calorie and 4.8-5.9 grams of protein. Biscuits were given to malnourished children for 90 days. Nonetheless, the effects had not improved yet the children nutritional status optimally. In fact, nutritional content of this biscuits had not met the WHO’s standard which should contain 400 calorie of energy, 15-20 grams of protein and lipid content in 20-40% of energy. The protein in the biscuit was from isolated protein, which was vegetable protein, not animal protein. Whereas, the quality of animal protein was superior compare to vegetable protein.
Food supplementation for children with underweight could be given in the form of functional food using local food ingredients [18]. Functional food was food product that physiologically beneficial for human body, [20] furthermore, could reduce the risk of certain diseases [21]. The functional food could came from traditional local food ingredients in certain area or country and contain benefit that exceeded the nutritional requirements [20,22]. We have developed an Indonesian locally-based functional food in the form of biscuit which was built from eel; as the protein, lipid, vitamins and minerals source; and “Cilembu” sweet potato as the carbohydrate source. The aim of the study was to analyse effects of Anguilla biscuit on body weight improvement in under-five years old children with underweight.
Material and Methods
Research design
The design of this study was RCT (Randomized Controlled Trial), pre-post design with single blind. The research was conducted in Rancakalong Sub-district, Sumedang District, Indonesia in January – May 2017.
Subjects
Subjects of the study were children aged 3-5 years old with underweight (based on body weight for age) who fulfilled the study inclusion and exclusion criterion. Inclusion criteria were: children aged 3-5 years old; underweight nutritional status caused by primary factors based on WHO standard 2005; and agree to participate in the study for 90 days. Whereas, the exclusion criterion were children who had illness which would interfere supplementary food give-away process based on physical and diagnostic examination. Drop out criterion were: children who did not consumed the biscuit given at least 1 piece daily and/or did not finished up the biscuit package given; the children’s parents resigned while intervention was conducted; the parents and child moved to an unknown address; and the children who were sick and required an inpatient care. The total samples were 56 children, divided equally into 2 groups, which were intervention and control groups. The intervention group was given Anguilla biscuit, while the control group was given standard biscuit from Indonesian Ministry of Health.
Subject selection was performed using single blind random sampling. Subjects in intervention and control group came from different villages, but had similar characteristics. Subjects selection was conducted in Posyandu (integrated health post) by using anthropometric and health examination. The anthropometric measurement consist of bodyweight measurement by Posyandu cadre and validation by Puskesmas nutritionist. Health examination was then performed by doctor and assisted by midwife. The bodyweight measurement was conducted using Camry digital scales with 0.1 kg accuracy and had been calibrated previously.
Methods
Before the intervention, anthropometric examination, including bodyweight and height, was performed by Posyandu’s cadres. Validation and nutritional status determination was conducted by Puskesmas’s (Public Health Centre) nutritionists. Moreover, the food intake assessment was done by nutritionist using 24 hours recall methods. After that, the cadres accompanied by research team distributed the biscuits to be consumed in a week, the biscuits were given to the children’s parents weekly.
The cadres measured bodyweight weekly for 3 months. The compliance of biscuit consumption was monitored daily using observation logbook. There were 10 cadres participated in children’s nutritional status monitoring and biscuit consumption compliance. There were 5 nutritionists participated in this study who were in charge of 24 hours recall assessment. The food intake assessment has been done every 2 weeks to discover whether there was difference in dietary habit among children. Bodyweight measurement and food intake assessment were re-conducted at the end of the study.
The supplementary food
Supplementary formulation used in the study consist of sugar, margarine, flour and Cilembu sweet potato flour as energy sources, as well as milk, eggs and fish meal from eel as protein sources. The supplement was combined in the form of biscuit because it was the commonly consumed food in diverse population. Biscuit also had various flavors, yet had a long shelf life and relatively low cost.
Nutritional composition of Anguilla biscuit per 100 grams were 446 calorie of energy, 20.6 grams of fat, 16.5 grams of protein, 50.8 grams of carbohydrate, 116.5 mcg of vitamin A, 29.85 mg of zinc, 38,1 mg of Fe and 921.86 mg of calcium. Biscuit for the control group comprised 450 calorie of energy, 14 grams of fat, 9 grams of protein, and 71 gram of carbohydrate. The biscuit should be consumed 10 pieces daily for 90 days. There were 3 biscuit formulas which met colour, flavour, texture and aroma, including formulas with F-263, F-549 and F-708 codes. The results of organoleptic test had determined formula with F-263 code was preferred by the panellists which was has a 50:50 composition of fish meal and Cilembu sweet potato flour. The Anguilla biscuit had undergone a proximate test, metal and microbiology contamination tests in Saraswanti Indo Genetech Laboratory which confirmed that there were not any contaminations found.
Statistical Analysis
Data analysis in this study was done using R program version 3.2.2. Univariate analysis was performed to find out distribution of the baseline data, as well as children’s characteristics, which include age, initial bodyweight, energy and protein intake and initial Z-score. Bivariate analysis was conducted to identify association between controlled and uncontrolled variables.
Results
Characteristics of subjects in intervention and control group
Analysis results on study subjects’ characteristics showed that children’s age, initial bodyweight, initial Z-score, initial energy and protein intake did not correspond between two groups (p>0.05). It indicated that both groups were in similar condition or homogenous.
Bodyweight improvement in children in intervention and control group
The initial mean bodyweight in intervention group, which were given Anguilla biscuit, was higher (12.23 kg) compared to the control group (12.01 kg). Likewise, the calculation of mean bodyweight after intervention in the intervention group was higher (13.18 kg) compared to the control group (12.38 kg) (Table 1).
Table 1 Baseline characteristics of study subjects by groups.
| Characteristics |
Group |
P value |
| Intervention n=26 |
Control n=27 |
| Age |
| x(SD) |
49.5(6.89) |
48.6(7.14) |
|
| Median |
51 |
48 |
0.6538* |
| Range |
36-61 |
36-60 |
|
| Bodyweight |
| x(SD) |
12.18(1.11) |
12.00(0.74) |
|
| Median |
11.9 |
12.2 |
0.7245* |
| Range |
9,9-14 |
10.6-13.50 |
|
| Z-Score |
|
|
|
| x(SD) |
-2.46(0.26) |
-2.38(0.17) |
|
| Median |
-2.385 |
-2.4 |
0.4546** |
| Range |
(-2.93)-(-2.14) |
(-2.8)-(-2.06) |
|
| Energy Intake |
| x(SD) |
835(198.91) |
870(203.56) |
|
| Median |
826 |
847 |
0.5249* |
| Range |
476-13.04 |
481-1326 |
|
| Protein Intake |
| x(SD) |
22.69(6.97) |
23.07(5.07) |
|
| Median |
21,50 |
23 |
0.763* |
| Range |
Oct-37 |
16-36 |
|
*Unpaired T-test, **Chi Square test
Statistical tests were performed in both groups which resulted in the significant difference of mean bodyweight before and after the children were given the supplementary biscuits in intervention group, as well as in control group (p=0.001). The mean bodyweight improvement in the intervention group was 0.952 kg, whereas in the control group was only a 0.285 kg improvement. In accordance to statistical tests, the difference of bodyweight improvement between the intervention and control group were significant (p=0,001).
The bodyweight was measured weekly. The changes of the bodyweight per month in the intervention and control group were shown in Figure 1.
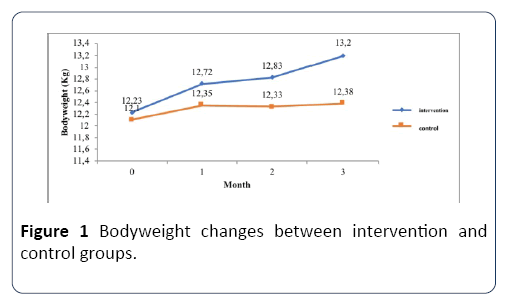
Figure 1: Bodyweight changes between intervention and control groups.
Bodyweight in the intervention group has been improving in the first through third month. However, in the control group, there was a fluctuating change in the bodyweight. The decrease of bodyweight happened in the second month (Table 2).
Table 2 Bodyweight improvement between intervention and control groups.
| Variable |
Groups |
P value |
| Intervention n=25 |
Control n=27 |
| Pre |
Post |
Pre |
Post |
| Bodyweight |
| x(SD) |
12.23(1.11) |
13.18(1.19) |
12,01(10.74) |
12.38(0.84) |
|
| Median |
12.2 |
13.3 |
12.2 |
12.3 |
|
| Range |
9.9-14.00 |
10.8-15.3 |
10.6-13.5 |
10.4-14.0 |
|
| P value |
0.001* |
|
0.001* |
|
0.001* |
| Deviation Post-pre (Δ) = |
| x(SD) |
0.952(0.6) |
|
0.285(0.3) |
|
|
| Median |
0.8 |
|
0.2 |
|
|
| Range |
0,2-1 |
|
(-0.4)- 0.9 |
|
|
| Mean Improvement |
7.80% |
|
2.40% |
|
|
*Unpaired T-test
Nutritional status improvement of children with underweight based on body Weight per age (BW/A) Z-Score in both groups
Initial mean Z-score in the intervention group was lower (-2,44) compared to the initial mean Z-score in the control group (-2,38). Nevertheless, the mean BW/A Z-score after 3 months of intervention were higher (-1,95) in the intervention group compared to the mean Z-score in control group (-2,34). The significant difference in the mean Z-score before and after intervention in both group were demonstrated in the results of statistical analysis. There was also a significant difference in the mean BW/A Z-score between the intervention and the control group (Figure 2).
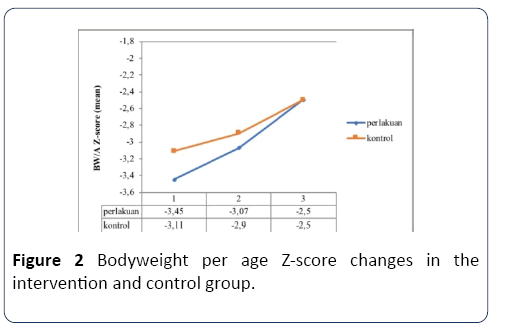
Figure 2: Bodyweight per age Z-score changes in the intervention and control group.
Changes of BW/A Z-score in the respective groups were shown in Figure 2. The Z-score were improved in both groups after the supplementary food was given. However, a higher improvement of BW/A Z-score was exhibited in the intervention group (Table 3).
Table 3 Bodyweight per age Z-Score improvement by groups.
| Variable |
Group |
P-value |
| Intervention n=25 |
Control n=27 |
| Pre |
Post |
Pre |
Post |
| BW/A Z-Score |
| x(SD) |
-2.44(0.26) |
-1.95(0.39) |
-2.38(-1.7) |
-2.34(0.32) |
|
| Median |
-2.33 |
-1.96 |
-2.4 |
-2.3 |
|
| Range |
(-2.92)-(-2.14) |
(-2.8)-(-0.71) |
(-2.80)-(-2.1) |
(-2.96)-(-1.84) |
0.001* |
| P value |
0.001* |
|
0.001* |
|
|
| Deviation (Δ) = Post-pre |
| x(SD) |
0.49(0.42) |
|
0.04(0.23) |
|
|
| Median |
0.45 |
|
0.06 |
|
|
| Range |
(-0.26)-1.96 |
|
(-0.33)-0.52 |
|
|
| Mean Improvement |
20% |
|
1.7 |
|
|
*Unpaired T-test
Discussion
This study show that supplementary Anguilla biscuit intervention to the children under five years old with underweight for 3 months could improve bodyweight and Zscore (based on bodyweight for age). In the intervention group, the bodyweight improvement reached 7.8%, while in the control group only reached 2.4%. These results were better compared to the study conducted by Zavoshy et al. in India [23]. Zavoshy study reported that supplementary food intervention for 6 months to malnourished children could improve bodyweight as high as 6.1%. The improvement of bodyweight in our study was superior compared to Zavoshy et al. [23]. It was most likely because the nutritional content of Anguilla biscuit was exceptional. Nutritional composition of Anguilla biscuit per 100 grams including 446 calorie of energy, 20.6 grams of fat, 16.5 grams of protein, 50.8 grams of carbohydrate, 116.5 mcg of vitamin A, 29.85 mg of zinc, 38.1 mg of Fe and 921.86 mg of calcium. Zavoshy et al. [23] was giving lunch which produced by rural nurseries in the form of lentil meal, Istanbul rice, lentil with rice, spaghetti, potato sauce with rice and a traditional soup. These foods had nutritional content of 360 ± 20 kcal energy, 17% protein, 53% carbohydrate and 30% fat.
Roberts et al. [24] were conducting a study in Guinea- Bissau, with giving biscuit to the children 1-3 years old for 11 weeks as the intervention. The nutritional contents of the biscuit were 291 kcal of energy, 16.8% of protein, 29.4% of carbohydrate, 48.4% of fat, 309 mg of EPA, 209 mg of DHA and 2 grams of fibre. The biscuit formulation was a substitution of RUTF (ready-to-use supplementary foods) and FBFs (fortified blended foods) which commonly used in low income countries. The effects of the biscuit were proven able to improve malnutrition condition and cognitive function of the children [24]. A study conducted by Parikh et al. [25] in the Dominican Republic among children under five years old who were given supplementary food demonstrated a reduction of acute under nutrition status rate from 40% to 23%, and chronic under nutrition status rate from 33% to 18% [25].
Several countries had given RUTF (ready to use therapeutic food) and RUSF (ready to use supplement food) as supplementary food for malnourished children and resulted in improvement of children nutritional status. Borg did a modification of RUSF by augmenting it with fish and milk as additional protein sources. RUSF was an innovative nutritional supplement produced locally and contained some micronutrient which enriched by lipid (LNS/Lipid based nutrient supplement) [26]. Administration of this supplementary food was similar in our study which gave supplementary food produced from eels. Giving supplementary food using local products was well-accepted by children. According to Borg, giving macro-and-micronutrientcontained food which was produced locally would be better accepted and cheaper than the imported products [26].
The study by Sigh et al. [27] showed that there were no significant effects by giving locally-based RUTF on bodyweight improvement in 121 Cambodian children. This result was not in accordance to our study because the subjects with infection parameter, such as Human Immunodeficiency Virus, tuberculosis, diarrhea and fever were not included in exclusion criteria, thus, the catabolism process of the subjects could interfere the bodyweight improvement. However, Sigh et al. [27] still stated that locally-based RUTF was the most relevant alternative nutritional intake besides dairy-based imported RUTF for children with underweight [27].
The improvement of mean Z-score in our study was 20% in the intervention group and 1.7% in the control group. These results were in accordance to the study conducted by Dong, which the prevalence of wasting was decreased from 3.5% to 1.7% [28]. A research which includes 116 Aboriginal children in isolated community in Australia showed that children who were given supplementary food for 4 months had bodyweight improvement of almost 1 kg heavier than children who did not received supplementary food [29]. Systematic review conducted by Kristjansson et al. [29] demonstrated that supplementary food given to the children in low and middle income countries had a small but statistically significant beneficial impact to bodyweight improvement of 0.12 kg [30].
Supplementary food intervention helped the children to perform a more consistent diet and protect the children from food insufficiency. Therefore, with better eating pattern, the bone growth and brain development of the children would be improved simultaneously [31]. This research had limitations, including double blind was not performed, moreover, body composition and biochemistry parameter examination were not conducted.
Conclusion
Anguilla biscuit supplementation for children under five years old for 3 months associated with bodyweight and Z-score improvement of underweight children under five years old.
Acknowledgement
The authors would like to thank Padjadjaran University- Indonesia for the funding of this research. We also gratefully acknowledge all the volunteers who have participated in this study.
Author Disclosures
The authors have no potential conflicts of interest. This project was funded by the Padjadjaran University Indonesia. Functional Food is produced by JNC Cookies and has gone through microbiological test examination, metal contamination and proximate and micronutrient tests.
23553
References
- You D, Hug L, Yao C, Newby H, Wardlaw T (2014) Levels and trends in child mortality Report 2014. Estimates Estimates developed by the UN inter-agency group for child mortality estimation. New York.
- Nzefa LD, Monebenimp F, Ang C (2018) Undernutrition among children under five in the Bandja village of Cameroon, Africa. South African J Clin Nutr 658: 1-5.
- Indonesia Ministry of Health (2013) Indonesia Basic Health Research 2013. National Institute of Health Research and Development (NIHRD), Ministry of Health (Indonesia), Jakarta.
- Waber D, Bryce C, Girarad J, Zichlin M, Fitzmaurice G, et al. (2015) Impaired IQ and academic skills in adults who experienced moderate to severe infantile malnutrition: A 40-year study. Nutr Neurosci 17: 58-64.
- Black RE, Morris SS, Bryce J (2003) Where and why are 10 million children dying every year? Lancet 361: 2226-2234.
- Munthali T, Jacobs C, Sitali L, Dambe R, Michelo C (2015) Mortality and morbidity patterns in under-five children with severe acute malnutrition (SAM) in Zambia: A five-year retrospective review of hospital-based records (2009-2013). Arch Public Heal 73: 1-9.
- https://www.undp.org/content/undp/en/home/sustainable-development-goals.html.
- Yudhoyono SB (2005) Vision and direction for Indonesia long-term development 2005- 2025. Indonesian ministry of national development planning, Jakarta.
- Rytter MJH, Kolte L, Briend A, Friis H, Christensen VB (2014) The immune system in children with malnutrition - A systematic review. PLoS One 9: 8.
- Adu-Afarwuah S, Lartey A, Brown KH, Zlotkin S, Briend A, et al. (2007) Randomized comparison of 3 types of micronutrient supplements for home fortification of complementary foods in Ghane: effects on growth nad motor development. Am J Clin Nutr 86: 412-420.
- Remans R, Pronyk PM, Fanzo JC, Chen J, Palm CA, et al. (2011) Multisector intervention to accelerate reductions in child stunting: An observational study from 9 sub-Saharan African countries. Am J Clin Nutr 94: 1632-1642.
- Ciliberto MA, Sandige H, Ndekha MJ, Ashorn P, Briend A, Ciliberto HM, et al. (2005) Comparison of home-based therapy with ready-to-use therapeutic food with standard therapy in the treatment of malnourished Malawian children: A controlled, clinical effectiveness trial. Am J Clin Nutr 81: 864-870.
- Linneman Z, Matilsky D, Ndekha M, Manary MJ, Maleta K, et al. (2007) A large-scale operational study of home-based therapy with ready-to-use therapeutic food in childhood malnutrition in Malawi. Matern Child Nutr 3: 206-215.
- Manary MJ, Ndekha MJ, Ashorn P, Maleta K, Briend A (2004) Home based therapy for severe malnutrition with ready-to-use food. Arch Dis Child 89: 557-561.
- Diop EHI, Dossou NI, Ndour MM, Briend A, Wade S (2003) Comparison of the efficacy of a solid ready-to-use food and a liquid, milk-based diet for the rehabilitation of severely malnourished children: A randomized trial. Am J Clin Nutr 78: 302-307.
- Manary M, Sandige H (2008) Management of acute moderate and severe childhood malnutrition. Br Med J 13: 337.
- Manary MJ (2006) Local production and provision of ready-to-use therapeutic food (RUTF) spread for the treatment of severe childhood malnutrition. Food Nutr Bull 27: 83-89.
- Bazzano AN, Potts KS, Bazzano LA, Mason JB (2017) The life course implications of ready to use therapeutic food for children in low-income countries. Int J Environ Res Public Health 14: 4.
- Shahidi F (2012) Nutraceuticals, functional foods and dietary supplements in health and disease. J Food Drug Anal 20: 226-230.
- Briend ANP (2005) Malnutrition: primary causes, epidemiology, and prevention. (2nd edn.). In: Caballero B, Allen L, editors. Encyclopedia of human nutrition. Oxford: Elsevier Academic Press; pp: 203-212.
- Doyon M, Labrecque JA (2008) Functional foods: A conceptual definition. Br Food J 110: 1133-1149.
- Zavoshy R, Noroozi M, Jahanihashemi H, Kiamiri D (2012) Nutritional intervention on malnutrition in 3-6 years old rural children in Qazvin province, Iran. Pakistan J Biol Sci 15: 347-352.
- Roberts SB, Franceschini MA, Krauss A, Lin P-Y, Braima de Sa A, et al. (2017) A Pilot Randomized Controlled Trial of a New Supplementary Food Designed to Enhance Cognitive Performance during Prevention and Treatment of Malnutrition in Childhood. Curr Dev Nutr 1: e000885.
- Parikh K, Marein-Efron G, Huang S, O’Hare G, Finalle R, et al. (2010) Nutritional status of children after a food-supplementation program integrated with routine health care through mobile clinics in migrant communities in the Dominican Republic. Am J Trop Med Hyg 83: 559-564.
- Borg B, Mihrshahi S, Griffin M, Sok D, Chhoun C, Laillou A, et al. (2018) Randomised controlled trial to test the effectiveness of a locally-produced ready-to-use supplementary food (RUSF) in preventing growth faltering and improving micronutrient status for children under two years in Cambodia: A study protocol. Nutr J 17: 1-11.
- Sigh S, Roos N, Chamnan C, Laillou A, Prak S, et al. (2018) Effectiveness of a locally produced, fish-based food product on weight gain among cambodian children in the treatment of acute malnutrition: A randomized controlled trial. Nutrients 10: 1-17.
- Dong C, Ge P, Ren X, Wang J, Fan H, et al. (2013) Prospective study on the effectiveness of complementary food supplements on improving status of elder infants and young children in the areas affected by Wenchuan Earthquake. PLoS One 8: 9.
- Kristjansson B, Petticrew M, Macdonald B, Krasevec J, Janzen L, et al. 2009) School feeding for improving the physical and psychosocial health of disadvantaged students. Cochrane Databse Syst Rev 1: 2007-2009.
- Kristjansson E (2016) Supplementary feeding for improving the health of disadvantaged infants and children What works and why?? March 2016 Systematic Review Summary 5.
- Vaitla B, Devereux S, Swan SH (2009) Seasonal hunger: A neglected problem with proven solutions. PLoS Med 6: 6.

