Zi Yan1*, Bradley J Cardinal2, Ruben J Guzman3, Walker A. Maddalozzo4, Gianni F.Maddalozzo5
1M.Ed., M.P.H., Doctoral degree candidate and Graduate Teaching Assistant, Exercise and Sport Science Program, School of Biological and Population Health Sciences, Oregon State University, OR, 97331 USA
2Ph.D., Professor, Exercise and Sport Science Program, School of Biological and Population Health Sciences, Oregon State University, OR, 97331 USA
3B.S., Masters degree candidate and Graduate Teaching Assistant, Exercise and Sport Science Program, School of Biological and Population Health Sciences, Oregon State University, OR, 97331 USA
4Undergraduate student, Department of Civil Engineering, Oregon State University, OR, 97331 USA
5Ph.D., Senior Instructor, Exercise and Sport Science Program, School of Biological and Population Health Sciences, Oregon State University, OR, 97331 USA
- *Corresponding Author:
- Zi Yan
M.Ed., Exercise and Sport Science Program
School of Biological & Population Health Sciences
Langton Hall, Oregon State University
Corvallis, OR 97331, USA
E-mail: yanzi@onid.orst.edu
Key words
Health, physical activity, psychology, well-being.
Introduction
Among adults 65 years of age and older, falls are the leading cause of accidental death and nonfatal injury [1]. Approximately one-third of community-dwelling adults over 65 fall each year, with approximately 50% experiencing multiple falls. For those over 80, the fall rate increases to approximately 40–50% [2]. However, falls are not an inevitable part of aging, and exercise plays a role in preventing falls [3,4]. For example, in randomized clinical trials, significant and meaningful reductions in fall rates have been reported following exercise interventions [5].
Exercise programs aimed at improving muscle strength and/or power are the most common interventions aimed at decreasing falls and fall risk [6]. However, the causal relationship between muscle function and balance is weak [6]. Moreover, there are important limitations to designing and implementing such programs among older adults (e.g., noncompliance with training, inability to perform certain exercises, increased risk of injury). Recently the benefits of whole-body vibration (WBV) for improving functional performance among older adults have been documented [7,8] and this may serve as a more tolerable and potentially beneficial alternative to resistance training programs. Furthermore, when WBV is supplemented with resistance training exercises (e.g., Thera-bands, Akron, OH), the benefits of WBV may be especially pronounced [9].
WBV activates muscles via the reflexes [10]. While the efficacy of WBV remains unclear due to a variety of methodological limitations, some studies do demonstrate its benefits for improving balance, body composition, bone density, functional mobility, and muscle performance [9,11,12]. However, whether WBV has any positive psychological benefits remains to be seen, with a recent case-study suggesting that it was a useful therapeutic modality for reducing a 70 year old male’s subjective expression foot pain associated with diabetic peripheral neuropathy [8]. To the contrary, it did not attenuate mental stress, life satisfaction, or sleep disturbances among 40-49 year olds undergoing a low-back pain reduction program [13].
The aim of this study was to compare the effects of 6-months of WBV training to an existing community-based group exercise program (CBEP) on older adults’ balance and mood. It was hypothesized that 6-months of WBV training would positively influence older adults’ balance and mood, and that there would be different effects on older adults’ balance and mood between those undergoing WBV and CBEP.
Methodology
Design and participants
This was a randomized, community-based, clinical trial conducted over 6-months. Thirty-one people volunteered to participate (5 male, M age= 89.8 ±8.8, and 26 female, M age = 74.5±8.1) and they were randomly assigned to WBV (n=15) or CBEP (n=16). The WBV group received 15 minutes of vibration, 5 days/week for 6 months on a TurboSonic® Deluxe WBV platform (Irvine, CA) while performing supervised lower-limb Thera-band exercises. Participants in the exercise class met 2 days/week for 50 minutes per session for 6 months. An American College of Sports Medicine certified instructor taught the CBEP. The intent of the CBEP was to improve the participants’ flexibility, strength, balance, and overall fitness levels. No specialized equipment was used in the CBEP.
Measures and Procedures
Balance testing was conducted on the Neurocom-7 Smart Balance Master (Clackamas, OR) using the Sensory Organization Test (SOT) protocol. Visual, somatosensory, and vestibular stimuli were manipulated in the six conditions of the test, each of which had three 20-second trials. In condition one, the control condition, all sensory information was available for use. In condition two, the participant’s eyes were closed. In condition three the participant watched the visual scene, which moved in conjunction with the participant’s postural sway, providing visual/vestibular conflict and making visual information unreliable. In conditions four, five, and six, the visual manipulations of conditions one, two, and three, respectively, were repeated, but the force plate pitched in conjunction with the participant’s postural sway. The participant’s equilibrium score, which is the average of the scores from the three sensory systems together, reflects their overall balance.
The Profile of Mood States (POMS) was used to assess total mood disturbance (TMD). The POMS is a widely used measure of mood state and mood change [14]. It assesses six mood states: tension-anxiety, depression-dejection, anger-hostility, vigor-activity, fatigue-inertia, and confusion-bewilderment. The measure has good internal consistency(α = .84 to .95) and adequate test–retest reliability (r = .65–74) [15]. On the measure, participants responded to 65 different adjectives representing the six higher-ordered mood states. Respondents assessed each adjective on the basis of how they felt over the previous 6-months using a 5-point Likert scale where 0 is “not at all,” 1 is “a little,”2 is “moderately,” 3 is “quite a bit,” and 4 is “extremely.” A TMD score was calculated by summing all of the raw scores, with some values reverse scored (i.e., high vigor scores reflected a good mood or emotion and low scores in the other factors also reflected this.). Thus, scores could range from a low of -32 to a high of 228 on the measure.
The experimental protocol and study procedures, including the manner in which informed consent was obtained from the participants and all necessary exercise clearances, was approved by the authors’ Institutional Review Board. Moreover, all study personnel completed the National Institutes of Health research ethics online certification program prior to their involvement in the study.
Analysis
Data were collected pre- and post-intervention. Given the age and gender distribution of the participants, and in an effort to increase statistical power, age and gender served as covariates in the main analysis, which consisted of a 2 (group) × 2 (time) repeated measures multivariate analysis of covariance (MANCOVA). Data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 16.0.
Results
The internal consistency for POMS was α = 0.91 and α = 0.92 for pre- post-intervention, respectively. There was no group, time, or interaction effect observed within the MANCOVA. Specifically the group effect was Wilk’s Lambda = 0.91, F (2, 26) = 1.23, p >0.05, η2 = 0.09; the time effect was Wilk’s Lambda = 0.99, F (2, 26) = 0.10, p >0.05, η2 = 0.01; and the group by time interaction was Wilk’s Lambda = 0.86, F (2, 26) = 2.19, p >0.05, η2 = 0.14.
Although none of the main or interaction effects were significant, the proportion of variance accounted for in the group by time interaction was 14%, which is moderate. The Delta values for the WBV and CBEP for balance were +2.00 and +5.31, respectively; and for mood +5.66 and -0.19, respectively.
Discussion
This study compared the effects of 6-months of WBV training to an existing CBEP on community-dwelling older adults’ balance and mood. No significant differences between the two training protocols was found; however, 14% of the group by time interaction effect was accounted for, suggesting a moderate effect in favor of the CBEP group over the WBV group for balance and mood. The apriori hypotheses in which differential effects in the opposite direction were expected was not supported. Given the limited sample size and large standard deviations observed on the mood variable in particular, the statistical power in this study was low and, therefore, the results should be interpreted with caution.
In this study two exercise training protocols were compared, with the WBV protocol being the experimental protocol and the CBEP being the standardized protocol. The WBV protocol was more of an individualized training program occurring 5 days per week, for 15 minutes per session (i.e., 75 minutes per week total). The CBEP was an existing community-based program that was group-based and it occurred 2 days per week for 50 minutes per session (i.e., 100 minutes per week total). Given the differences in type, frequency, and duration of training, it is difficult to attribute the findings of this study exclusively to the exercise training protocols being compared. Future studies should strive to equate these to a greater degree, though this may be difficult in real-world terms. That is, it may be cost prohibitive and contraindicated to use the vibration platform in an identical manner as the CBEP protocol. Specifically, there were only two WBV units available for use in this study, which necessitated that this phase of the intervention be delivered in more of an individualized format versus the group format of the CBEP. Group exercise classes allow people to exercise together, which may increase social support and social cohesion. In addition, instructor characteristics such as knowledge, skill, and leadership style, may also influence participant satisfaction and psychological response to the intervention [16]. Lastly, it may be contraindicated to engage in WBV for durations longer than those employed in the present study. Such real-world challenges will need to be addressed in future research so as to improve the quality of science seeking to test the efficacy of WBV.
Although it is unclear precisely how WBV influences balance in comparison to CEPB, previous studies have reported the effects of WBV on performance among elders to be as effective, if not more so, than other types of intervention. For example, Bruyere and colleagues [17] compared the effect of WBV plus physical therapy (n=22) to physical therapy only (n=20) on balance and health-related quality of life among 44 elders living in a nursing home. Compared to the physical therapy only group, those receiving the six-week WBV intervention with physical therapy had a greater increase in their overall balance, as well as health-related quality of life. Another study showed that 24 weeks of WBV was as effective as resistance training on increasing knee strength among older women [18]. In their review, Rehn and colleagues [19] concluded that there is strong to moderate evidence that long-term WBV exercise can have positive effect on leg muscular performance, including balance performance. The effect of short-term WBV remains inconclusive. Moreover, as more studies focus on the physical effects of WBV, few studies have examined the psychological effects of WBV. It is clear that regular exercise has positive psychological effect such as improving mood [20]. The positive psychological effects obtained from regular exercise also promote long-term physical activity participation. Hence, exploring the psychological effects of WBV is necessary, as it may influence long-term WBV participation.
In conclusion, our study addresses the short-term effect of WBV, differences between WBV and CBEP in conjunction with supplemental resistance training exercises, as well as the psychological effect of WBV. Notably, we did not observe any between or within group differences suggesting that 6-months of WBV, at least within our set of observations, was equally as effective as was the CBEP on community-dwelling older adults’ balance and mood.
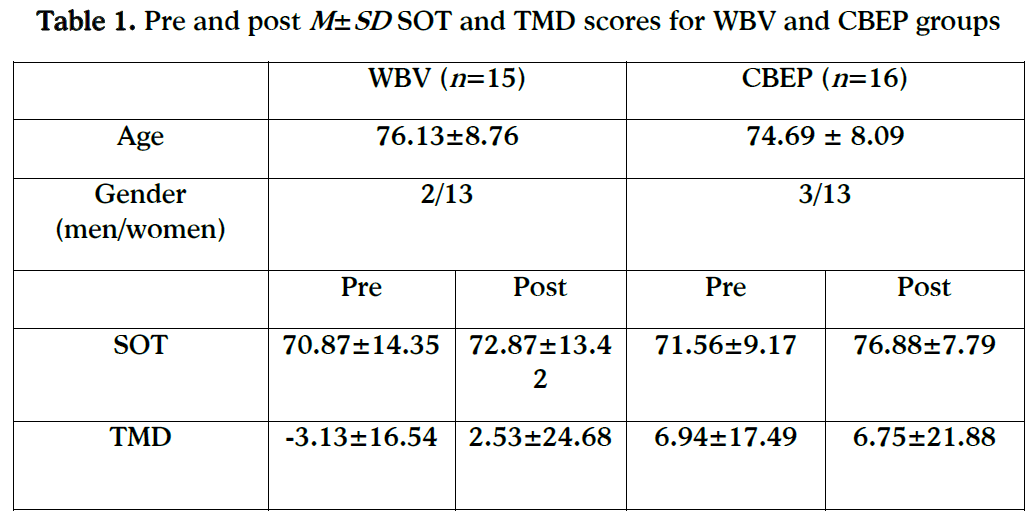
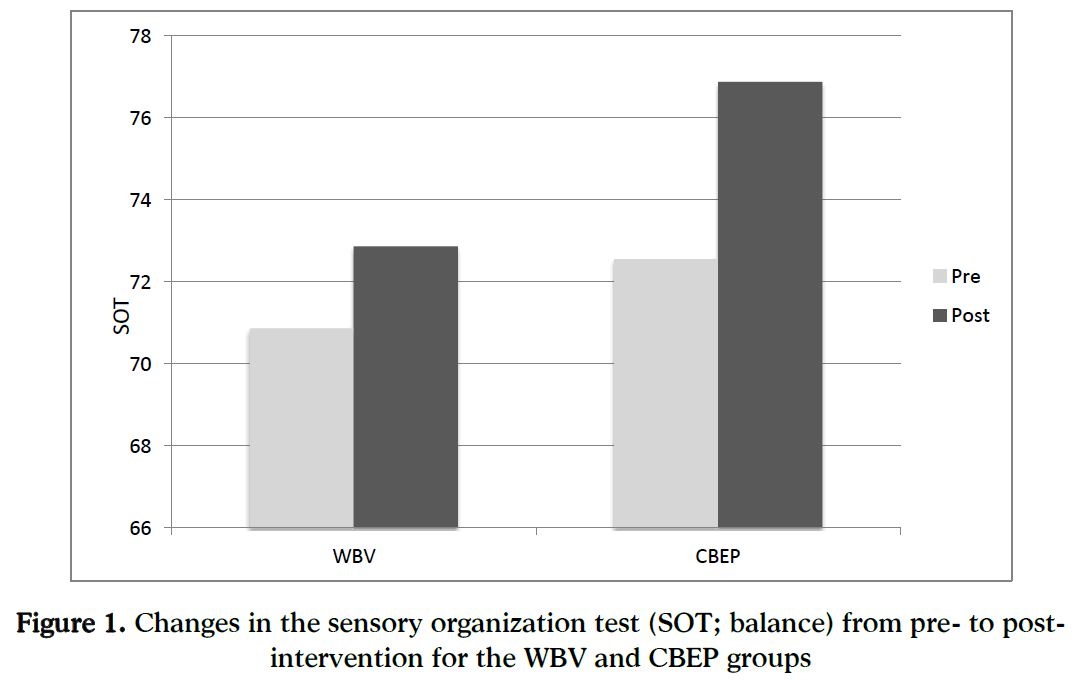
Figure 1: Changes in the sensory organization test (SOT; balance) from pre- to post-intervention for the WBV and CBEP groups
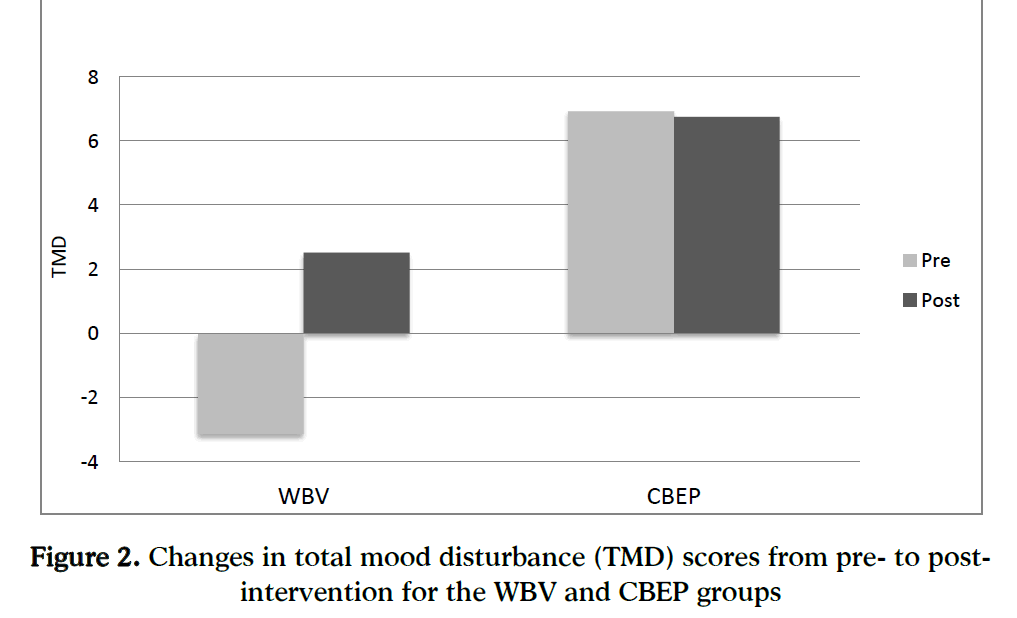
Figure 2: Changes in total mood disturbance (TMD) scores from pre- to post-intervention for the WBV and CBEP groups
Acknowledgment
This study was funded by a research grant awarded to G. F. Maddalozzo, Ph.D. from the John C. Erkkila, M.D. Endowment for Health and Human Performance, Good Samaritan Hospital Foundation, Corvallis, OR.
5299
References
- Murphy SL. Deaths: final data for 1998. National Vital Statistics Reports. 2000;48(11):1–108.
- Luukinen H, Koski K, Honkanen R, Kivelä SL. Incidence of injury-causing falls among older adults by place of residence: a population-based study. Journal of the American Geriatrics Society. 1995;43(8):871-876.
- Moreland J, Richardson J, Chan DH, O’Neill J, Bellissimo A, Grum RM, et al. Evidence-based guidelines for the secondary prevention of falls in older adults. Gerontology. 2000;49(2):93–116.
- Feder G, Cryer C, Donovan S, Carter Y. Guidelines for the prevention of falls in people over 65. British Medical Journal. 2000;321(7267):1007-1011.
- Barnett A, Smith B, Lord SR, Williams M, Baumand A. Community-based group exercise improves balance and reduces falls in at-risk older people: a randomised controlled trial. Age and Ageing. 2003;32(4):407-414.
- Orr R. Contribution of muscle weakness to postural instability in the elderly. A systematic review. European Journal of Physical and Rehabilitation Medicine. 2010;46(2):183-220.
- Furness TP, Maschette WE, Lorenzen C, Naughton GA, Williams MD. Efficacy of a whole-body vibration intervention on functional performance of community-dwelling older adults. The Journal of Alternative and Complementary Medicine. 2010;16(7):795–797.
- Hong J. Whole body vibration therapy for diabetic peripheral neuropathic pain: A case report. Health Science Journal. 2011;5(1):66-71.
- Maddalozzo GF, Dodge N, Galver JW, Li F, Cardinal BJ. Effects of whole-body vibration on bone mineral density in post hip surgery patients. Medicine & Science in Sports & Exercise. 2009;41(5):140.
- Rittweger J, Beller G, Felsenberg D. Acute physiological effects of exhaustive whole-body vibration exercise in man. Clinical Physiology. 2000;20(2):134–142.
- Merriman H, Jackson K. The effects of whole-body vibration training in aging adults: a systematic review. Journal of Geriatric Physical Therapy. 2009;32(3):134.
- Vissersa D, Verrijkenb A, Mertensc I, Van Gilsc C, Van de Sompelc A, Truijena S, et al. Effect of long-term whole body vibration training on visceral adipose tissue: A preliminary report. Obesity Facts. 2010;3(2):93–100.
- Miranda H, Viikari-Juntura E, Punnett L, Riihim\äki H. Occupational loading, health behavior and sleep disturbance as predictors of low-back pain. Scandinavian Journal of Work, Environment & Health. 2008;34(6):411–419.
- Berger BG, Motl RW. Exercise and mood: A selective review and synthesis of research employing the profile of mood states. Journal of Applied Sport Psychology. 2000;12(1):69–92.
- McNair DM, Lorr M, Droppleman LF. POMS manual: Profile of mood states. San Diego, CA: Educational and Industrial Testing Service. 1992;
- Leary MR, Kowalski RM. Impression management: A literature review and two-component model. Psychological Bulletin. 1990;107(1):34-47.
- Bruyere O, Wuidart MA, Palma ED, Gourlay M, Ethgen O, Richy F, Reginster JY. Controlled whole body vibration to decrease fall risk and improve health-related quality of life of nursing home residents. Archives of Physical Medicine and Rehabilitation. 2005;86(2):303-307.
- Roelants M, Delecluse C, Verschueren SM. Whole-Body-Vibration training increases knee-extension strength and speed of movement in older women. Journal of the American Geriatrics Society. 2004;52(6):901-908.
- Rehn B, Lidstrom J, Skoglund J, Lindstrom B. Effects on leg muscular performance from whole-body vibration exercise: a systematic review. Scandinavian Journal of Medicine & Science in Sports. 2007;17(1):2-11.
- Penedo FJ, Dahn RB. Exercise and well-being: a review of mental and physical health benefits associated with physical activity. Current Opinion in Psychiatry. 2005;18(2):189-193.

