Keywords
Employment status; Suicidal ideation; Health inequalities
Introduction
Suicide is a public health problem and an important indicator of severe mental ill-health [1-4]. Much of the existing research has focused on completed suicides or suicide attempts [5- 8]. Experience of suicidal ideation and to make suicide plans, increases the risk of suicide attempts, and all forms of suicidal thoughts and behaviours imply a greater risk for completed suicide [1,9,10]. Identifying risk factors for suicidal ideation and provide adequate actions to counter it are therefore a public health priority.
Unemployment as an independent risk factor for poor mental health status, including depression, is well-known [11-14]. Recently, there has been an increased interest in whether unemployment increases the risk of suicidal behaviour, including suicidal ideation [15,16]. For instance, unemployment status has been found to be both a significant and unique risk factor for suicidal ideation for psychiatric outpatients [1]. A prospective follow-up study of the general population in Finland observed that suicidal ideation at baseline was associated with a cluster of adverse life events, including unemployment. Moreover, depressive mood seems to be a necessary mediating factor [17]. Because of the impact of unemployment on mental health, research into the effects of unemployment on suicidal ideation is of great importance.
Also, there has been a debate world-wide, and particularly in Europe regarding the impact of the recent economic crises, which started in 2008 on health outcomes, not least psychological health [18,19]. In Greece, Triantafyllou and colleagues found that significantly more individuals with high index of personal economic distress (IPED) showed suicidal ideation compared to those with low IPED [20].
Studies carried out in various industrialized countries have found that unemployment is associated with suicidal behaviour and suicidal ideation [4,21-23]. However, discussions continue about the nature of this association, and it is argued that the association on one hand may reflect a direct causation and on the other hand a non- causal association [21,24]. For instance, a longitudinal study of a birth cohort from New Zeeland has observed that after adjustment of confounders, including non-observed fixed sources of confounding, unemployment was still significantly associated with suicidal ideation [21]. On the other hand, Hintikka et al reported that even after adverse life events such as unemployment, depressive mood was an essential precondition for suicidal ideation among the Finnish population [17]. However, so far, mostly these discussions about causality or non- causality, refer to studies about suicide or suicide attempt [5,7,8,25].
To our knowledge, in Sweden, no study has investigated suicidal ideation in relation to employment status, especially in the light of recent economic recession. On the other hand, a study carried out in Sweden during the 1990`s recession found that the excess risk of suicide among the unemployed to some part was related to higher prevalence of sickness absence among the unemployed [26].
The county of Gävleborg in Sweden has experienced factory closures and layoffs above the national average caused by the economic crises that started in 2008 [27,28]. The unemployment rate among adults 16-64 years increased sharply during the period 2008-2010 and was 12,0 % of the labour force in 2010 (national average was 8.7% at the same time). The youth unemployment rate in the county (18-24 years) increased during the same period from 17.2-27.3% [29]. In addition, for men, Gävleborg County has among the highest levels of suicide in the country. For instance, age standardized death rate among men (15-64 years) in 2012 due to suicide was 25,0 per 100,000 individuals in the county, compared with the national average at 19.4 [30]. In 2010, at the time for the survey, the suicide death rate for men (15-64 years) was 20.1 per 100,000 individuals and the national average at the same time 20.2. Notably then, was the large differences between age groups. For example, the age group 60-64 had a suicide death rate of 56.3 in the county, compared to national average at 26.2. Also the youngest (15-19 year) with a suicide death rate of 20.3 was more than twice as high compared to national average at 9.6 [30]. To our knowledge research addressing the relation between employment status and suicidal ideation is non-existent in the county, considering the massive lay –offs that have occurred as a result of the economic crisis.
Therefore the present study is aimed to contribute to the ongoing debate on the health consequences of the economic crises by examining the relationship between employment status and suicidal ideation at the pick of the most recent economic recession in Gävleborg County.
Method and Material
Study setting
The Gävleborg County is located in east central Sweden with the municipality of Gävle as the capital of the county. The current population of the county is estimated to be approx. 280,000 inhabitants, where around 95,000 live in the capital. The county has ten municipalities spread over a land area of 18,192 km2, corresponding to about 4% of Sweden's total area [31]. In 2010, at the time of the survey, the unemployment rate in Gävleborg was in total 9.8 % of the population aged 16-64 and 12,0 % of the registered labour force. The national average at the same time was 6.9 % and 8.7 %, respectively [27,29].
Study sample and design
The study used secondary data from the 2010 Gävleborg Health on Equal Terms (HET), a cross sectional population-based survey. A municipality based random sample of 12,000 individuals from Gävleborg was selected from a sampling frame based on the County Total Population Register (TPR). The sampling frame consisted of all registered residents within the county between the ages of 16-84, in total 221,618 on January, 2010. The sample selection was carried out by Statistics Sweden and a final check of the sample showed that 23 people no longer belonged to the population, resulting in a final sample size of 11,977 individuals. A total of 5,983 individuals returned the questionnaire (response rate of 50.0%.) However, for this study only 4,245 individuals at working age (16-65 years) were used.
Survey procedure
The survey was conducted by Statistics Sweden as a postal survey in combination with web survey. The survey was a collaboration between the Swedish National Institute of Public Health and the Gävleborg County Council, and carried out between March and June 2010. A mailed questionnaire was sent for the first time in Mars 22, 2010. The respondents had the opportunity to choose if they wanted to answer the questionnaire on paper or on the web; login details came with mailings, where they could login through Statistics Sweden's website to complete the survey. Along with the questionnaire, the selected individuals received an information letter containing study background and objectives, information about client, how the answers would be used and that data would also be retrieved from the register of total population, (data on education, income and taxation). The letter also emphasized the confidentiality of the survey as well as to whom they could turn to if there were any questions regarding the investigation. Three reminders were sent out to the participants to return the questionnaires. All the questionnaires were scanned by Statistics Sweden. The questionnaires contained questions about, health, economic conditions, lifestyle, labour and employment as well as security and social relationships.
Measurements of variables
In this study, the outcome variable was suicidal ideation. Suicidal ideation was assessed using the following question, “Have you ever during the last 12 months found yourself in a situation that you seriously considered taking your life?” and there were three possible answers (no, yes once and yes several times). For the purpose of this study, the responses were recoded to yes and no.
Main independent variable
The main independent variable in this study was employment status. In the survey, employment status was assessed by using one question, what is your current main job? The answers were dichotomized in two categories, those who had work and those who were out of work (including, leave of absence, students and early retired).
Other independent variables (control variables)
Demographic and socio-economic variables such as sex, marital status, age, income, cash margin and education as well as social support, self-reported health, long-standing illness, self-reported stress, anxiety and risk consumption of alcohol were used as control variables.
Marital status was defined in terms of being married (or living with a partner), being single (including divorced partner) or being widow/widowed.
For this study, five age groups were created, 16-25, 26-35, 36-45, 46-55 and 56-65 years, respectively.
Income was collected from income and taxation register (relates to 2008) as total individual annual gross income and three groups were created: a) low-income < 250 thousand SEK, b) medium-income 250-750 thousand SEK and c) high income, > 750 thousand SEK a year.
Cash margin was measured by the question: “Should you suddenly find yourself in an unforeseen situation in which you had to get hold of 15,000 Swedish crowns in a week, could you manage this?” There were two possible answers dividing those who could do it (yes) from those who couldn’t do it (no).
Education was assessed by using Statistics Sweden's educational register from 2009. The classification is made for the person's highest level of education according to Swedish educational nomenclature (SUN) 2000 [32]. For the current study three levels of education were created: primary school or similar; secondary school/similar and university/similar.
Social support was measured by using the question: “Do you have someone you can share your deepest feelings with and confide in"? There were two possible answers that divide those with social support (yes) from those without social support (no).
Self-reported health was assessed using the question, “How would you rate your general health?” and there were five possible answers (very good, good, fairly, bad and very bad). For this study, the answers were dichotomized. Those who answered very good or good were regarded as having good health and those who answered fairly, bad or very bad were regarded as having poor health
Long standing illnesses was measured using the question: “Do you have long standing illness, health problems or similar?” The answer was dichotomized in Yes or No format
Self-reported stress was assessed by the question: Do you feel stressed at present? Stressed means a state in which you feel tense, restless, nervous, worried or distracted. The question could be answered with: not at all, to some extent, pretty much and very much. For this study, self-reported stress was divided into three groups: Not at all, somewhat, and pretty much or very much as a third group.
Anxiety was measured by using the question: “Do you have symptoms or signs of Anxiety, worry or anguish?” Possible answers were: No, Yes, mild discomfort and Yes, great discomfort. A dichotomous variable was created to distinguish those without (no) anxiety from those with (yes, mild and great) anxiety.
Risk consumption of alcohol was assessed by three questions a) “How often have you drank alcohol in the past 12 months”? b) “How many “glasses” (example was given) do you drink on a typical day when you drink alcohol?” c)”How often do you drink six “glasses” or more on the same occasion”? A new composite variable was used for this study and was categorized as Yes (risk consumption) and No (no risk consumption).
Statistical analyses
Data analyses were performed using IBM SPSS Statistics 20.0 [33] and included descriptive and logistic regression analyses. The logistic regressions were used to assess the relationship between employment status and suicidal ideation, and were performed using four models. Model I analysed the relationship between employment status and suicidal ideation only. Then in Model II potential demographic confounders like sex, marital status and age were included. Model III included socio-economic variables such as income, cash margin, education and social support were included. Finally in Model IV health and lifestyle variables like self-reported health, long-standing illness, self-reported stress, anxiety and risk consumption of alcohol were included. Results are presented as OR with 95% confidence intervals.
Ethical approval
Ethical approval for the study was given by the Swedish National Institute of Health and the Regional Ethical Committee in Uppsala.
Results
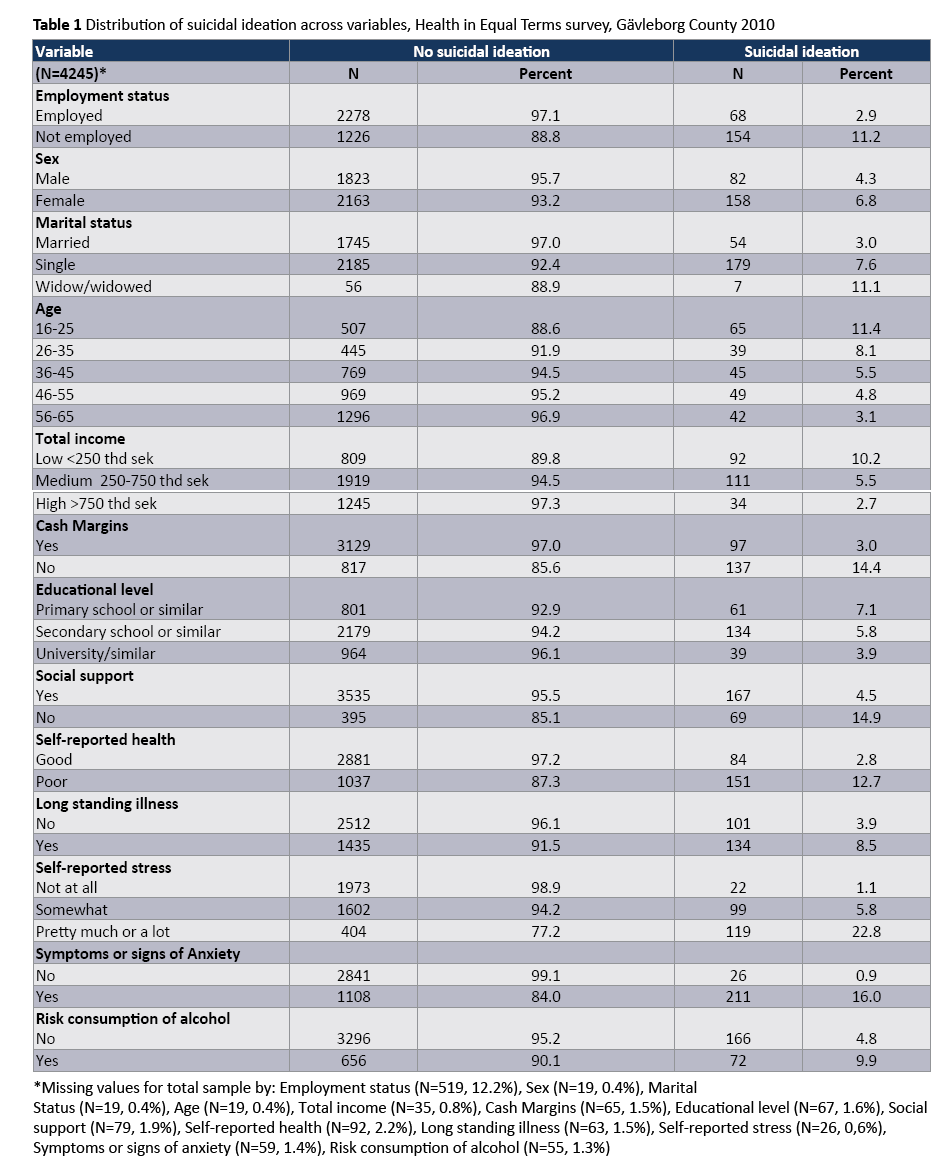
The distribution of suicidal ideation across variables can be seen in table 1. In this population of 4245 adults (16-65 years), 11.2% of those not employed had at some time been in a situation where they seriously considered taking their life. Among the employed the corresponding figure was 2.9%. In addition, the results revealed that more than three times as many (11.4%) in the youngest age group (aged 16-25 years) had reported suicidal ideation, compared with 3.1% in the oldest age group (aged 56-65 years). Regarding income, 14.4% of those with no cash margins had had suicidal ideation compared to 3.0% of those who had cash margins. In terms of health and lifestyle, suicidal ideation was more common in those with no social support (14.9%), poor self-reported health (12.7%), with pretty much or a lot of self-reported stress (22.8%) and symptoms of anxiety (16%), compared to those who had social support (4.5%), good self-reported health (2.8%), no self-reported stress (1.1%) and no symptoms of anxiety (0.9%) respectively.
In the bivariate analysis (model I), people who are not employed had a higher risk for suicidal ideation than those employed (Table 2). Those not employed had about 4 -fold higher risk for suicidal ideation with odds of 4.21 (CI 3.14-5.64).
Adjustment for sex, marital status and age only (model II) slightly decreased the odds for suicidal ideation, from 4.21 (CI 3.14- 5.64) to 3.93 (CI 2.85-5.42). In model III, which included socioeconomic variables such as total income, cash margins education and social support, the odds decreased further to 2.64 (CI 1.84-3.81). In the final model (model IV), which further added variables such as self-reported health, long standing illness, selfreported stress, symptoms of anxiety and risk consumption of alcohol in the multivariate analyses reduced further the odds, but the association between no employment and suicidal ideation continued to be statistical significant with odds of 1.73 (CI 1.16- 2.57) compared with those who were employed (Table 2).
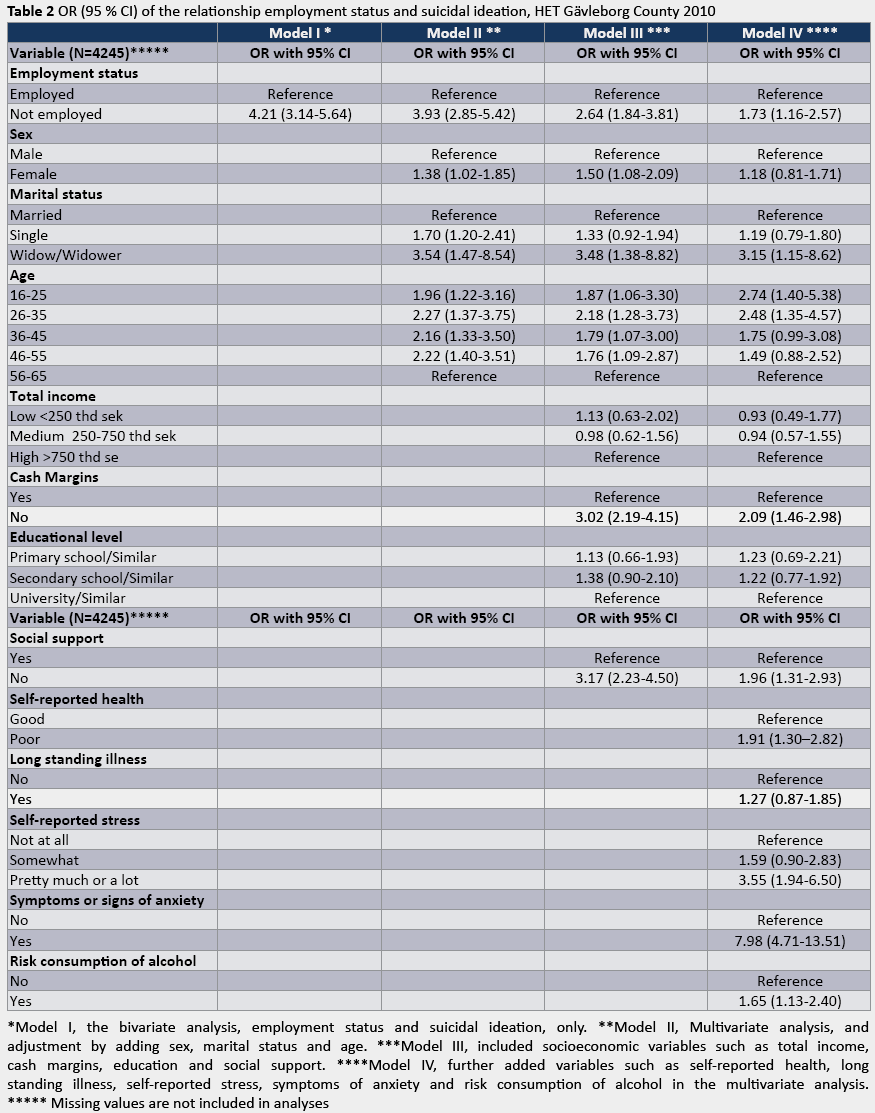
Regarding other variables, being a widow/widower, at young age (16-25, 26-35 year), lack of cash margins, no social support, and poor self- reported health, pretty much or a lot of self-reported stress and symptoms of anxiety as well as risk consumption of alcohol were associated with suicidal ideation. For instance, those who reported anxiety had odds of 7.98 (CI 4.71-13.51) for suicidal ideation compared to those without such symptoms (Table 2). Furthermore, persons who reported pretty much or a lot of stress had odds of 3.55 (CI 1.94 – 6.50) compared to those who had no stress. In regard to age, individuals 16-25 years had odds of 2.74 (CI 1.40-5.38), and individuals aged 26-35 had odds of 2.48 (CI 1.35-4.57) for suicidal ideation, all compared to the oldest, aged 56-65 years (Table 2).
Discussion
The present study found evidence of an association between employment status and suicidal ideation among residents of the Gävleborg County aged 16-65 years. Individuals who were not employed had higher odds of suicidal ideation of 4.21 (CI 3.14-5.64). Other studies have observed a similar relationship [15,16,21,24,34]. For instance, Fergusson and colleagues, reported that exposure to unemployment was associated to suicidal ideation among young Australians 18-21 years old. In addition, the study found that the impact of unemployment on individual risk was entrenched in a wider context of risk factors for disorder, such as social disadvantage, family dysfunction, and personal characteristics [21].
However, other studies have reported different results regarding factors associated with suicidal ideation [35,36]. For instance, Botega and colleagues found no association between unemployment and suicidal ideation among men and women in Campinas, Brazil. In that study, suicidal ideation was associated with factors linked to mental disorders and psychological distress [35]. In a study of 17 countries who participated in the WHO World Mental Health Surveys, it was found that employment was unrelated to suicidal behaviours. In that study, the strongest risk factors were impulse control disorders in middle-and low- income countries, and mood disorders in high-income countries [36].
Controlling for other variables, the association between being out of work (not employed) and suicidal ideation decreased from 4.21(CI 3.14-5.64) in model I, to 1.73 (CI 1.16- 2.57) in model IV, but continued to be statistically significant (Table 2). Similar findings were reported by a study carried out in the Province of Kuopio, Finland, where the risk of suicidal ideation among the unemployed persisted even after adjusting for socio-demographic variables. In addition, when results were adjusted for higher BDIScore (Beck Depression Inventory, [37,38]. the risk was reduced to no significance [17]. In our study, self-reported psychological health was measured by the variables stress and anxiety. Controlling for these variables in model IV reduced significantly the risk, but it remained significant. This might suggest that other factors such as unemployment duration, depression etc. which were not captured by the questionnaire might be at play. Several studies have reported that people with depression and severe mental health have suicidal thoughts [35,36,39].
As a result of the economic crisis that started in 2008, the unemployment rate in the county was high, at the time when data for this study were collected. Among adults 16-64 years of age the unemployment rate increased dramatically from 7.2% in 2008 to 12% of the labour force in 2010 (national average increased from 5% to 8.7% for the same period). The youth unemployment rate in the county (18-24 years) increased at the same time from 17.2 to 27.3% [29]. This rapid increase in unemployment levels might have caused a great economic and emotional strain among individuals and their families. Furthermore, being out of the labour force could have ignited feelings of helplessness, which have been found to be associated with thoughts of suicide [35,36].
The debate continues on the nature of the association between unemployment and suicidal ideation. For instance, if unemployment is not a causing event, it has been argued that unemployment could increase the risk of suicidal behaviour, not in the sense of being a ‘triggering agent’, but as an ongoing situation affecting vulnerability when a provoking agent is present. Of course, unemployment may act as a provoking agent sometimes and a vulnerability factor otherwise [40].
Due to the cross-sectional nature of our study, it was not possible to make any assumptions if unemployment acted as a provoking agent or vulnerability factor. However, the additional risk observed for suicidal ideation among those out of work remained despite adjustment for other covariates. On the other hand, unemployment has been shown to be a risk factor for poor mental health status and severe depressive reactions, and thus could cause this vulnerability [14,41]. Due to small cell numbers and wide confidence intervals we could not perform analysis of the stratified sample of those who were not employed (e.g. students, early retired).
Regarding other variables included in the analyses, the study found increased odds of 2.74 (1.40-5.38) among persons aged 16-25 years and of 2.48 (1.35-4.57) among those aged 26-35 years compared to the oldest group, 56-65 years. In addition, being widow/widower appeared to be associated with suicidal ideation. Similar findings have been reported by Pirkis and colleagues. These authors also found that age and marital status were associated with suicidal ideation among Australian adults [42]. Our study also observed associations between suicidal ideation and lack of social support, lack of cash margin, poor selfreported health as well as risk consumption of alcohol. These results are in line with a study by Hintikka et al., [43], which used data from a 12 month follow- up study on suicidal ideation in the Finnish general population. The authors reported that suicidal ideation was more common among those who at baseline, lived alone, were unemployed, reported subjective financial hardship, and were frequent alcohol drinkers [43]. Other life-style variables such as smoking have been found to be associated with suicidal ideation in clinical samples and general populations [17,44,45], something that could not be seen in this study.
Furthermore, our study observed a relationship between lifecondition variables such as self-reported stress and symptoms of anxiety and suicidal ideation. The link between suicidal ideation and anxiety has been reported by others [39,46,47]. For example, Sareen and colleagues reported that the existence of any anxiety disorder was significantly associated with suicidal ideation in both cross-sectional and longitudinal analysis among Dutch, aged 18- 64 years 46. Moreover, anxiety has been linked to unemployment [48].
Our study was carried out at County level (Gävleborg County). Thus, it can provide lessons to similar international contexts on the potential impact of job loss on mental health outcomes such as suicidal ideation and other suicidal behaviours (e.g. suicidal attempts and completed suicide). The understanding of the role of place (e.g. County) on differences in mental health among economically active persons can contribute to reduce employment related inequalities at national level, especially in times of economic hardship.
Limitations and strengths
The analyses were based on cross-sectional data, which obviously have their limitations. Even if properly supplementary information is available; it precludes causality and its direction. In addition, it was not possible to conduct analyses for duration of unemployment. Previous studies have shown that the duration of unemployment may have an impact on suicidal thoughts [24].
The non-response rate of fifty per cent is another limitation of the present study. Still, that is in line with decreasing response-rates in population based surveys in Sweden as a whole [49]. It is implied that in population based surveys, non-respondent groups have a high likelihood to report poor health outcomes [50,51]. However, results from our study are unlikely to have been affected by nonresponse bias. Statistics Sweden used population weightings to calculate prevalence at the population level. Furthermore, apart from adjustments for the sample sizes in the different strata, the register data was used for calibration of non-response bias for various groups of individuals [52-54]. Also, our analyses could not include self-reported depression a variable, which has been found to be associated with suicidal ideation and suicidal behaviour in general [11-14,17].
The strengths of the present study are the large data set, collected at the county level, in a region hard hit by factory closures and a high level of unemployment [27]. Also the study used validated instruments, which had been quality reviewed. For instance, the whole Health on Equal Terms questionnaire has been reviewed for validity, and where e.g. the question about suicidal thoughts has been found to works well [55].
Conclusion
The present study found a statistically significant association between being out of work and suicidal ideation. The association was explained for the most part by social, demographic and selfreported psychological variables. Results of the study suggest the need for primary prevention strategies among those out of the labour market, especially during times of economic hardship.
3805
References
- Brown GK, Beck AT, Steer RA, Grisham JR (2000) Risk factors forsuicide in psychiatric outpatients: a 20-year prospective study. JConsult Clin Psychol 68: 371-377.
- Nock MK, Hwang I, Sampson N, Kessler RC, Angermeyer M, et al.(2009) Cross-national analysis of the associations among mentaldisorders and suicidal behavior: findings from the WHO WorldMental Health Surveys. PLoS Medicine 6: e1000123.
- Bernal M, Haro JM, Bernert S, Brugha T, de Graaf R, et al. (2007) Riskfactors for suicidality in Europe: results from the ESEMED study. JAffect Disord 101: 27-34.
- Inder KJ, Handley TE, Johnston A, Weaver N, Coleman C, et al. (2014)Determinants of suicidal ideation and suicide attempts: parallelcross-sectional analyses examining geographical location. BMCPsychiatry 14: 208.
- Blakely TA, Collings SC, Atkinson J (2003) Unemployment and suicide. Evidence for a causal association? J Epidemiol Community Health 57: 594-600.
- Kposowa AJ (2001) Unemployment and suicide: a cohort analysisof social factors predicting suicide in the US National LongitudinalMortality Study. Psychol Med 31: 127-138.
- Beautrais AL, Joyce PR, Mulder RT (1998) Unemployment and serious suicide attempts. Psychol Med 28: 209-218.
- Jones SC, Forster DP, Hassanyeh F (1991) The role of unemployment in parasuicide. Psychol Med 21: 169-176.
- report on the 2007 National Survey of Mental Health and Wellbeing. The Department of Health, USA.
- Kuo WH, Gallo JJ, Tien AY (2001) Incidence of suicide ideation and attempts in adults: the 13-year follow-up of a community sample in Baltimore, Maryland. Psychol Med 31: 1181-1191.
- Kim SS, Subramanian S, Sorensen G, Perry MJ, Christiani DC (2012) Association between change in employment status and new-onset depressive symptoms in South Korea - a gender analysis. Scand J Work Environ Health 38: 537-545.
- Frese M, Mohr G (1987) Prolonged unemployment and depression in older workers: a longitudinal study of intervening variables. Soc Sci Med 25: 173-178.
- Mossakowski KN (2009) The influence of past unemployment duration on symptoms of depression among young women and men in the United States. Am J Public Health 99: 1826-1832.
- Jefferis BJ, Nazareth I, Marston L, Moreno-Kustner B, Bellón JÁ, et al. (2011) Associations between unemployment and major depressive disorder: Evidence from an international, prospective study (the predict cohort). Soc Sci Med 73: 1627-1634.
- Fanous AH, Prescott CA, Kendler KS (2004) The prediction of thoughts of death or self-harm in a population-based sample of female twins. Psychol Med 34: 301-312.
- Fu Q, Heath AC, Bucholz KK, Nelson EC, Glowinski AL, et al. (2002) A twin study of genetic and environmental influences on suicidality in men. Psychol Med 32: 11-24.
- Hintikka J, Koivumaa-Honkanen H, Lehto SM, Tolmunen T, Honkalampi K, et al. (2009) Are factors associated with suicidal ideation true risk factors? A 3-year prospective follow-up study in a general population. Soc Psychiatry Psychiatr Epidemiol 44: 29-33.
- Stuckler D, Basu S, Suhrcke M, Coutts A, McKee M (2009) The public health effect of economic crises and alternative policy responses in Europe: an empirical analysis. Lancet 374: 315-323.
- Stuckler D, Basu S, Suhrcke M, Coutts A, McKee M (2011) Effects of the 2008 recession on health: a first look at European data. Lancet 378: 124-125.
- Triantafyllou K, Angeletopoulou C (2011) Increased suicidality amid economic crisis in Greece. The Lancet 378: 1459-1460.
- Fergusson DM, Horwood LJ, Woodward LJ (2001) Unemployment and psychosocial adjustment in young adults: causation or selection? Soc Sci Med 53: 305-320.
- Kessler RC, Berglund P, Borges G, Nock M, Wang PS (2005) Trends in suicide ideation, plans, gestures, and attempts in the United States, 1990-1992 to 2001-2003. JAMA 293: 2487-2495.
- Kjøller M, Helweg-Larsen M (2000) Suicidal ideation and suicide attempts among adult Danes. Scand J Public Health 28: 54-61.
- Fergusson DM, Boden JM, Horwood LJ (2007) Unemployment and suicidal behavior in a New Zealand birth cohort: a fixed effects regression analysis. Crisis 28: 95-101.
- Mäki N, Martikainen P (2012) A register-based study on excess suicide mortality among unemployed men and women during different levels of unemployment in Finland. J Epidemiol Community Health 66: 302-307.
- Lundin A, Lundberg I, Allebeck P, Hemmingsson T (2012) Unemployment and suicide in the Stockholm population: a register-based study on 771,068 men and women. Public Health 126: 371-377.
- https://www.arbetsformedlingen.se/Om-oss/Statistik-prognoser/ Tidigare-statistik.html
- https://www.arbetsformedlingen.se/Om-oss/Statistik-prognoser/ Tidigare-statistik.html
- https://www.lansstyrelsen.se/gavleborg/Sv/om-lansstyrelsen/om-lanet/Pages/default.aspx
- Statistics Sweden. Svensk utbildningsnomenklatur: SUN 2000: standard för klassificering av svensk utbildning = Swedish standard classification of education. Stockholm: Statistiska centralbyrån; 2000.
- Gunnell D, Harbord R, Singleton N, Jenkins R, Lewis G (2004) Factors influencing the development and amelioration of suicidal thoughts in the general population. Cohort study. Br J Psychiatry 185: 385-393.
- Botega NJ, Barros MB, Oliveira HB, Dalgalarrondo P, Marín-León L (2005) Suicidal behavior in the community: prevalence and factors associated with suicidal ideation. Rev Bras Psiquiatr 27: 45-53.
- Nock MK, Borges G, Bromet EJ, Alonso J, Angermeyer M, et al. (2008) Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br J Psychiatry 192: 98-105.
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J (1961) An inventory for measuring depression. Arch Gen Psychiatry 4: 561-571.
- Beck AT, Steer RA, Carbin MG (1988) Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clin Psychol Rev 8: 77-100
- Bronisch T, Wittchen HU (1994) Suicidal ideation and suicide attempts: comorbidity with depression, anxiety disorders, and substance abuse disorder. Eur Arch Psychiatry Clin Neurosci 244: 93-98.
- Platt S (1984) Unemployment and suicidal behaviour: a review of the literature. Soc Sci Med 19: 93-115.
- Björklund A, Eriksson T (1998) Unemployment and mental health: evidence from research in the Nordic countries. Int J Soc Welf 7: 219-235.
- Pirkis J, Burgess P, Dunt D (2000) Suicidal ideation and suicide attempts among Australian adults. Crisis 21: 16-25.
- Hintikka J, Pesonen T, Saarinen P, Tanskanen A, Lehtonen J, et al. (2001) Suicidal ideation in the Finnish general population. A 12-month follow-up study. Soc Psychiatry Psychiatr Epidemiol 36: 590-594.
- Park HS, Schepp KG, Jang EH, Koo HY (2006) Predictors of suicidal ideation among high school students by gender in South Korea. J Sch Health 76: 181-188.
- Tanskanen 1, Viinamäki H, Hintikka J, Koivumaa-Honkanen HT, Lehtonen J (1998) Smoking and suicidality among psychiatric patients. Am J Psychiatry 155: 129-130.
- Sareen J, Cox BJ, Afifi TO, de Graaf R, Asmundson GJ, et al. (2005) Anxiety disorders and risk for suicidal ideation and suicide attempts: a population-based longitudinal study of adults. Arch Gen Psychiatry 62: 1249-1257.
- Taylor A, Dal Grande E, Gill T, Fisher L, Goldney R (2007) Detecting determinants of suicidal ideation: South Australian surveillance system results. Int J Pub Health 52: 142-152.
- Molarius A, Berglund K, Eriksson C, Eriksson HG, Lindén-Boström M, et al. (2009) Mental health symptoms in relation to socio-economic conditions and lifestyle factors--a population-based study in Sweden. BMC Public Health 9: 302.
- Boström G (2014) What non-response means to the result in public health surveys? [In Swedish].
- Drivsholm T, Eplov LF, Davidsen M, Jørgensen T, Ibsen H, et al. (2006) Representativeness in population-based studies: a detailed description of non-response in a Danish cohort study. Scand J Public Health 34: 623-631.
- Kotaniemi JT, Hassi J, Kataja M, Jönsson E, Laitinen LA, et al. (2001) Does non-responder bias have a significant effect on the results in a postal questionnaire study? Eur J Epidemiol 17: 809-817.
- Statistics Sweden (2010) Health on equal terms. Survey 2010. Gävleborg County Council.
- Lundström S, Särndal C (1999) Calibration as a standard method for treatment of nonresponse. Journal of Official statistics 15: 305-328.
- Särndal C, Lundström S (2005) Estimation in surveys with nonresponse. John Wiley & Sons, Chichester.
- Boström G and Nyqvist K (2010) Objective and background of the questions in the national public health survey. Swedish National Institute of Public Health, Sweden.

