Key words
Medication error, risk factor, nurse, intravenous injection
Introduction
Errors that occur when injecting high-risk medications can critically harm patients, and the resulting malpractice liability falls on hospitals as well as the nurses who administer the drugs. When injected intravenously, a drug’s absorption rate is very high. [1] This means that special attention is required when performing injections, both before and after administration. Highly enriched electrolytes, such as potassium chloride (KCl) and sodium chloride (NaCl), heparin (an anticoagulant), anticancer agents, and other high-risk medications require particular care. [2,3] Looking from the patients’ point of view, “high-risk medication” means the harm (i.e., infiltration, extravasation, and phlebitis) caused by the errors related to high-risk intravenous injection. High-risk medication induces various complications such as “venous fragility,” “flare” (an acute local allergic reaction), and “venous spasm.” Such complications may occur during injection of cytotoxic drugs such as chemotherapy drugs. Looking from the nurses’ point of view, it indicates the harm and side effects induced by the drug on skin, eyes, and mucous membranes via direct contact. When patients are exposed to these drugs for a long period, the tissues in contact may develop ulcers and/or necrosis. [4-7]
To reduce negligence in this area, medical institutions have begun to establish safety guidelines for the injection of high-risk medications. Abbott [8] argues that nurses’ awareness of the safe administration of medication has a considerable effect on patient safety. Choi et al., [9] have also found a positive correlation between nurses’ awareness of a patient safety culture and their safety care activities. Identifying the causes of nurses’ errors when administering high-risk intravenous injections may facilitate safer practices. Injection-related tasks are performed by a team of nurses, doctors, and pharmacists, so all of these professionals are likely to have important insights into the factors that lead to mistakes in the injection process.
The purpose of the present study was to identify the causes responsible for and problems associated with errors in the administration of high-risk medication via intravenous injections. Since perspective on this subject is likely to differ depending on work environment and job type, we collected the viewpoints of medical personnel who work with nurses as well as viewpoints of the nurses themselves. For this, a focus-group interview was conducted with the medical personnel who are engaged in medication-related tasks in clinical settings for an in-depth examination of their experience and awareness. The main aim was to provide baseline data to aid in establishing a safety culture among nurses who administer high-riskintravenous injections.
Methods
Participants
The subjects were 13 healthcare providers (7 nurses, 3 doctors, and 3 pharmacists) working in a university hospital in Daejeon city with experience in intravenous injection-related tasks. Focus group interviews were conducted between June and November 2011 to acquire in-depth knowledge of the causes associated with errors in the administration of high-risk intravenous injections.
Procedures
In this study, we selected focus group interview to gather information and brainstorm insights, intuitions, and ideas by means of activated interactions between participants. We focused on the common topics of medical institutions under the theme of “the causes and problems of the errors relevant to high-risk intravenous injection in hospital nurses.” The focus group interview served as a forum to share their experiences regarding the topic. [10]
A focus group method has an advantage of differentiating the comments that are commonly pointed out from those that are less relevant by comparing the discussions in subgroups. To consider the intergroup differences and collect varied information, this study was performed by classifying the health care professionals who were able to provide professional and useful information and experiences of high-risk intravenous injectioninto three groups, such as current nurses, doctors, and pharmacists. The first focus group was performed with seven nurses in June 2011, the second, with three doctors in July, and the third with three pharmacists in November at the seminar room of the hospital.
Before beginning each focus group, we explained the purpose of the study and the interview to the participants. Written consent was obtained after informing participants that the contents of the interview would be recorded, stored anonymously, and used only for research purposes and that they could withdraw from the research at any point. The interview data were de-identified by replacing interviewee names with serial numbers, and records were discarded after data analysis was complete. Data from the interviews comprised experiences with and insights into errors in administering high-risk intravenous injections. Participants’ answers were prompted by the question “What are the causes and problems associated with errors in high-risk intravenous injection administration, particularly those made by nurses”? Approximately 80–100 minutes were spent collecting data. In each interview, participants were encouraged to discuss their thoughts and experiences in a free and comfortable atmosphere. The interview was performed up to the saturation point of the data that there were no new comments regarding the causes and problems related to the errors of high-risk intravenous injection from each subject; the interview was conducted in a manner that facilitated the participation of all subjects.
Two field workers attended and noted significant content in each interview. They organized the extracted material before the interviews ended, confirmed the content with the participants, and confirmed additional comments. After this, the interview ended.
Data Analysis
The researcher of this study analyzed the data from the professional groups separately for an integrated understanding ofthe causes and problems of the errors associated with high-risk intravenous injection. During the study period, group discussions werecarried out by reading the collected data and figuring out the discussion contents accurately.The recorded field notes and de-briefing notes were integrated, and the data were analyzed using the content analysis method in order to improve the understanding of the phenomena. For this purpose, the transcribed collected data was read through several times, and the meaningful words, sentences, and paragraphs were extracted. After the open coding, they were categorized into similar sentences and paragraphs; the subtopics were identified in the categorized sentences, and the final topics were extracted andnamed. [11] To test the validity of the original data, the participants from whom the analyzed data were extracted were subjected to an in-depth interview in order to determine whether the analyzed data well reflected the causes and problems related to the errors of high-risk intravenous injection in nurses, and the names of the topics and subtopics were appropriate.
Following the method suggested by Spradly [12] each interview began with a broadly formulated open-ended type of question such as “Can you share the experiences you have had when administering high-risk intravenous medications?” The interviewee was not interrupted while answering, and the subsequent questions were increasingly narrowed to more detailed contents, referring to the previous answer. Each focus-group interview was conducted with the participation of at least two assistant researchers, who drafted in-situ notes, describing the characteristics of the interviewees and any notable linguistic as well as non-linguistic behaviors and facial expressions. These notes were included in data analyses. All interviewees were asked the following three core questions: (1) We would like to hear about your experiences regarding the administration of high-risk intravenous medications.(2) What is your responsibility related to the administration of high-risk intravenous medications?(3) Please tell us about the problems associated with the administration of high-risk intravenous medications, and the causes of those problems.
The data analyses addressed the core research questions used in the focus-group interviews, based on the data directly obtained from the interviewees, that is, excluding the possibility of being biased by any anticipated scope or theoretical views. We set up the following five detailed analytic principles: (1) we read the obtained data repeatedly to comprehensively summarize the phenomenon; (2) words and phrases carrying core ideas and concepts were identified and labeled todetermine codes; (3) words and phrases with similar meanings were categorized into groups with abstract values; (4) the codes thus extracted were regrouped by similarity and categorized into higher abstract-level topics; (5) the topics thus extracted were compressed again and integrated, which ultimately yielded the final topics,representing the essence of the experiences.
The validity of our study was established by testing the research method for comparing the focus-group interview results, using the assessment standards for qualitative research:credibility, auditability, fittingness, and confirmability. [13] Data-related credibility was assured by deliberately selecting the research participants (interviewees) as those who had had a sufficient number of experiences regarding the administration of high-risk intravenous medications, and by choosing open-ended questions so that the analysis could consider the whole spectrum of cases incurred in all typical circumstances and contexts. To ensure the credibility of analysis and interpretation, the qualitative content analysis was conducted, focusingonconsidering the interview contents objectively. Although the research team conducted a preliminary review of papers, reports, and other literature related to the administration of high-risk intravenous medications, to familiarize themselves with the existing data-specific sensibility, every effort was made to prevent any bias likely to arise from this knowledge; this was mainly done by considering the extracted content strictly objectively, and allowing no interpretation. The topics yielded by the analyses were corrected and complemented by a peer-feedback process, paying particular attention to ensuring credibility. The resulting report also used direct quotations from the participants, thus facilitating the comparison between the collected data and the extracted topics. The auditability was ensured by describing the data analysis method and procedure in detail. To ensure applicability, we included the participants’ demographic and professional characteristics in the report. The post-hoc validity was provided by verifying the differences among the three professional groups (nurses, doctors, and pharmacists), regarding the causes and problems of the administration of high-risk intravenous medications, from their respective perspectives. Thus, we performed an in-depth investigation of relevant problems in conjunction with related experiences.
Results
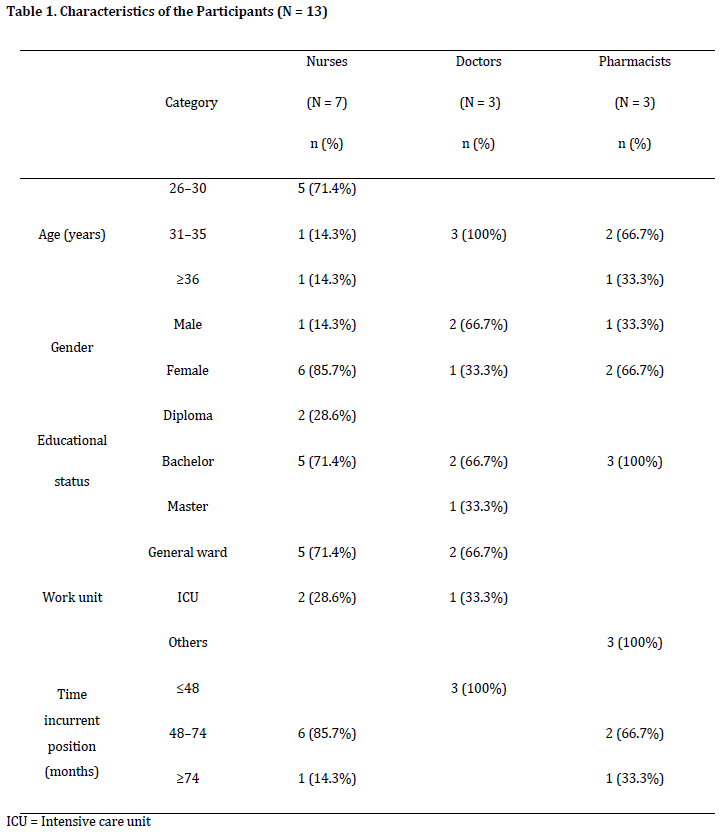
Demographic characteristics of the participants can be found in Table 1. Five of the seven nurses were between 26 and 30 years old, all three doctors in the study were between 31 and 35, and two of the three pharmacists were between 31 and 35. In addition, most of the interviewees had graduated university, including five of the nurses and all of the doctors and pharmacists. Finally, the majority of participants had over 48 months of experience in their current position. Six of the nurses had worked for 48 to 74 months while another had worked more than 74 months, and all of the pharmacists had over 48 months of experience in their position. By contrast, all three doctors had been in their position less than 48 months.
From the 13 healthcare providers’ experiences with and insights into the causes of nurses’ errors when performing high-risk intravenous injections, we extracted three causal categories: (1) human-related factors, (2) injection procedure-related, and (3) environmental factors. A detailed description of each category and subcategory listed above follows Table 2.

1) Human-related factors: lack of preparedness by the injection-administering nurse
“Lack of knowledge and awareness of high-risk medications” and “carelessness in controlling the drip and speed of high-risk medication” were two human-related factors that reflected a lack of preparedness by the injection-administering nurse.
• Lack of knowledge and awareness of high-risk medications
Both doctors and nurses pointed out that the number of different medications in use has climbed. If nurses lack appropriate knowledge and understanding of these medicines or inexperienced nurses administer injections, errors can result. By contrast, pharmacists perceived a decrease in attention and awareness resulting from the frequent administration of high-risk medications as an important factor in injection errors. They emphasized that a systematic approach is needed to reduce the occurrence of such mistakes.
“In the case of anticancer injections, except for nurses in wards that frequently use them, most of us don’t know much about the administration procedures or the medication precautions… [also] there are so many new medications nowadays, and we often have to administer them before we’re familiar with the medications’ mechanisms or precautions…” (Nurse)
“When administering high-risk medications, in the case of new nurses, problems arise from a lack of knowledge and experience; moreover, since the injection is done intravenously instead of orally, side effects manifest quickly and solutions are more difficult than in cases where the medication has been administered through other means.” (Doctor)
“In wards that frequently use [high-risk] medications, I have observed instances where they [nurses] habitually lacked familiarity with the precautions that must be taken when injecting.” (Pharmacist)
• Carelessness when controlling the drip speed of high-risk medication
Nurses raised concerns about the need to adjust drip rates based on the posture of each patient and the need to manually adjust the drip rate of high-risk medication, a process that is less accurate than automated adjustment. Doctors expressed concern about the decreased effects of medication if the drip rate is delayed. Pharmacists, despite working in an environment that did not allow them to observe what typically occurs, implicated inaccurate adjustment of fluid speed by nurses as a primary error in the administration of high-risk intravenous injections.
“When I inspect patients on my rounds, sometimes I notice that the fluid lines become entangled, and then the fluid rapidly enters the patient’s system as the lines are untangled… When we can’t borrow injection machines, we cannot accurately adjust the drip speed. Manually-adjusted rates change abruptly when a patient shifts their position…” (Nurse)
“There have been cases where the injection route into the vein was blocked, or the blood was regurgitated, or air had entered the veins… consider that it’s a high-risk medication and that the effect of the medicine decreases due to poorly administered intravenous injections…” (Doctor"The drip rate for high-risk medications cannot be adjusted accurately if the nurse uses only her eyes to measure … I have heard of patients having emergencies because of inaccurate high-risk intravenous injections.” (Pharmacist)
2) Injection procedure-related factors: omission of or negligence in important steps
Injection procedure-related factors can arise from omission of or negligence in carrying out the steps of the injection procedure, including “confusion as to which type of fluid should be injected” and “unclear verbal prescriptions from doctors.”
• Confusion related to the type of fluid injection
Most of the experiences related by nurses consisted of accidentally injecting a patient with the wrong fluid. Participants noted that if a large dose is required or there is a shortage of time, mistakes are more likely to happen.
“Some patients are injected with several medications at the same time. Therefore, sometimes there are several injection lines on a single fluid hanger, and if the nurse rushes or is not careful about it … mistakes are easily made. In the case of medication delivered through an inhaler solution, if it is prepared in a syringe and there is no marking on it, it can be mistaken for an intravenous injection.” (Nurse)
• Confusing verbal prescriptions from doctors
Nurses pointed out that administration errors could result from breakdowns in communication. In particular, they reported that when they are given verbal prescriptions by doctors in emergency situations, they can become confused about the name and dosage of the medication ordered. Pharmacists agreed that mistakes are made when nurses receive their instructions via verbal prescriptions. Doctors believed that errors did not stem from the verbal prescriptions themselves but occurred during the administration of medications.
“When prescriptions are given over the phone, because one cannot verify them and must carry them out independently, there is a higher possibility of making a mistake than with electronic prescriptions … inexperienced new nurses or nurses administering unfamiliar medications often make mistakes by not verifying the name or dosage of the medication … [Furthermore,] medications these days do not go by a uniform unit. With each drug having its own [dosage units] … [it can be either] 0.5 g or 500 mg [which can get confusing] . Some medications differ only by their label color, although the dosage for each matters considerably. Verbal prescriptions are usually given during emergencies, and so it’s kind of natural, considering the circumstances, for miscommunication to happen.” (Nurse)
"Nurses are very keen to receive electronic prescriptions as well, especially after being given verbal prescriptions … but we cannot help making verbal prescriptions [during emergencies] …” (Doctor)
“I believe that, if given verbal orders for highly enriched electrolytes, some nurses will make mistakes in the prescription confirmation and administration process.” (Pharmacist)
3) Environmental factors: inappropriate working environment
Factors related to working environments that are inappropriate for administering medication included “inappropriate medication management” and “shortage of medicators and lack of operating experience.”
• Inappropriate medication management
Nurses commented that confusion could arise when the medication storage cabinet was left open or when proper attention was not given to labels as medications were being blended. Doctors credited errors in medication management to a lack of safety devices and the failure of new nurses to adequately monitor the storage and administration of medicine. Pharmacists pointed out that safety can be compromised if the light-resistant wrappings of some medications, such as anticancer drugs, are damaged.
“Although some of the high risk medications are labeled accordingly and stored separately, the storage cabinet can be left open, and these medications can be confused with others. I often think that even if there is no ‘warning’ sign in the storage room or drug packaging box, something serious could still happen.” (Nurse)
“New nurses sometimes forget, especially when rushed, to connect the anticancer drugs properly, often failing to set the safety device at the right time. I get worried when I think about the hazards associated with such medications and the precautions that must be taken.” (Doctor)
“Caution must be taken not to expose anticancer drugs to light when administering them… when the packaging has been damaged, however, … [nurses] might administer the drug without knowing that it has happened.” (Pharmacist)
• Shortage of medicators and a lack of experiencein administering injections
Nurses pointed out that a high-risk medication injection can beinterrupted or compromised when a patient leaves their room with the medicator machine or when machines in the examination room are misused. Doctors suggested that the shortage of medicators was an important cause of injection errors, while pharmacists pointed out that sometimes nurses administer a medication without regard for the patient’s safety, often paying no attention to the drug’s characteristics.
“If the medicator stops operating when the patient is out of the nurse’s sight … then administration of the drug is not properly carried out…. The infusion device in examination rooms can also stop operating correctly, injecting the fluid injection too fast or too slow. This is especially dangerous when administering KCl-blended intravenous injections, because in serious cases, respiratory arrest may occur. So, in handling such high-risk medications, nurses often become anxious … I hope some systemized structure is set in place [in the future] to prevent a shortage of medicators or problems arising from misoperation.” (Nurse)
“I think there are times when there are a shortage of fluid injection devices in the wards … So I believe fluid loading can occur when administering KCl, NaCl, heparin, and anticancer drugs, especially in urgent cases where fluid injection speed adjustment devices are not used.” (Doctor)
“Some of the nursesomit the use of protective equipment when administering high-risk drugs (anticancer drugs) under the pretext that they are busy and are familiar with the proper drug administration as they have done it many times”(Pharmacist)
Discussion
The present study acquires a multi-perspective understanding of the nurses’ awareness of and experience in the safety and errors related to high-risk intravenous injection, by converging the opinions of health care professionals directly involved in high-risk intravenous injection safety, i.e., nurses, doctors, and pharmacists. We asked medical personnel directly involved in these procedures (nurses, doctors, and pharmacists) for their perspectives on common errors that occur during injections. Moreover, we performed an in-depth investigation of the problems with injection administration reported by these health professionals.
“Lack of knowledge and awareness of high-risk medications” and “carelessness in controlling the drip speed of high-risk medication” were identified as human-related factors involved in injection error, reflecting a lack of preparedness on the part of the nurses administering drugs. The belief that a lack of knowledge and awareness of medications underlies many injection errors, which was voiced by nurses, doctors, and pharmacists, is supported by Oh & Yoon’s [14] findings that the more aware nurses are of injection errors, the fewer mistakes they make. In addition, nurses and doctors called attention to the patency of the tubes through which high-risk medication is injected; if a proper link is not maintained, the patient’s treatment may be hindered and other adverse effects could result as well. Therefore, nurses must carefully consider the fluid injection speed and the integrity of the tube connection.
In light of the result of a study that stated that there wasa relationship between the nurses’ observation level and risk assessment, nurses’ negligence and mistake, lack of knowledge and experience came to affect the safety of patients. [15,16]
According to Ryou [17] 79% of nursing errors are caused by a “lack of caution.” In other words, 79% of these mistakes could have been prevented had nurses paid more attention. For these reasons, we deem it necessary to establish a safety management system that properly addresses high-risk intravenous medication administration. [18]
The recent trend in coping with errors in the hospital setting is recognizing the problem in the health care delivery system as the cause of error occurrence and focusing on preventive measures by improving the pertinent system. [19]
Additionally, it is suggested that to improve the safety of patients, it is crucial to establish a hospital environment where medical personnel are not criticized or punished for their errors, and efforts should focus on thoroughly analyzing the frequency and causes of actual errors and taking measures to prevent similar errors from recurring in the future. [20,21]
As for the factors associated with injection-related procedures, health professionals reported that most errors were caused by omission of or carelessness in proper injection protocol. Such factors include “injection of the wrong fluids” and “unclear verbal prescriptions from doctors.” “Injection of the wrong fluids” occurred primarily when nurses misplaced the correct fluid after preparing it, usually when multitasking. New nurses are prone to such errors, due to their inexperience with emergency situations. [22] Therefore, hospitals should establish an environment in which the nurse responsible for the initial injection takes responsibility for the entire procedure, including preparing and administering the injection and providing proper nursing care afterwards.
Nurses and pharmacists recognized “unclear verbal prescriptions from doctors” as a frequent cause of errors during emergencies. Doctors blamed such errors on the hospital, which often forces them to give verbal prescriptions. The complex conditions responsible for unclear verbal prescriptions, which likely result in injection errors, reflect the view advanced by Kim, et al. [23] They claim that administration safety errors are related to the organization as a whole, with such errors becoming more frequent when work backs-up or personnel are busy or fatigued. Because errors in high-risk intravenous injection can be fatal for patients, standardized administration procedures for dangerous medications must be carried out [24] and efforts to increase awareness of injection safety among medical personnel must be made.
As for the environmental factors related to injection errors that were reported in our interviews with health professionals, we extracted “inappropriate medication management” and “shortage of medicators and lack of operating experience” as two important concerns. If the fluid injection rate of a medication is adjusted without using the appropriate device, a patient’s movements can influence the injection speed; in this case, the expected effect of a drug may not be achieved, potentially influencing a patient’s treatment plan. This finding is consistent with previous research that reports excessive injections can result in critical harm. The pharmacists in our study, however, pointed out that some nurses are simply heedless of safety procedures, leading to inappropriate medication management. According to Park [25] , nurses can be learn about anticancer drugs through a variety of different channels. Therefore, appropriate education regarding the safety regulations of high-risk medications should require for all medical personnel. Hospitals should also organize their own injection safety guidelines for high-risk medications, along with periodic evaluations and educational supplementation. [26] Besides, the improvement of computer systems regarding drugs for high-risk intravenous injection would reduce the errors likely to occur at the prescription stage. Additionally, improvements of the injection environment, such as special management of high-risk drugs, patient recognition bracelets, application of barcode systems for certain drugs [27] , establishment of injection error reporting systems and organization safety culture in which analysis data are shared, and efforts for standardization through injection nursing QI activities, would be helpful as practical solutions.These will likely prove crucial efforts in increasing both patient and medical personnel safety. The results of our study can be used as baseline data for future research aimed at developing indices of quality improvement and improving the management of intravenous injections of high-risk medications.
Conclusion
Drug administration is one of a nurse’s most important tasks. No nurse wishes to commit an error while administering medication, thereby threatening patient safety. To prevent such accidents, the causes of errors must be identified so that hospitals can begin to establish prevention systems. In our study, focus group interviews were conducted with medical personnel familiar with the administration of injections in clinical settings. Our goal was to verify the causes of nurses’ errors in administering high-risk intravenous medications. We found that human, procedural, and environmental factors all contributed to injection errors. Identifying systemic factors at the organizational level that foster medical errors, altering human behaviors that contribute to injection mistakes, and improving elements of the work environment to promote safety will be essential steps in establishing a framework for safe, high-risk intravenous injections.
Acknowledgement
This study carried out with financial support by Institute of Nursing Research, KoreaUniversity in 2011.
2735
References
- Yang SH, Son YH, Paik HJ, Won JS, YooJH, JeonMY. Fundamentals of Nursing. Seoul: Hyunmoonsa; 2009.
- Tissot E, Cornette C, Limat S, Jacquet M. Observational study of potential risk factor of medication administration error. Pharm World & Sci: PWS. 2003;25(6):264-268.
- Medical Institution Accreditation Standards of Investigation. Korea Institute for Healthcare Accerditation Decision Rules. Seoul; 2011.
- Choi BK.A study on nurses’ and pharmacists’ exposure to antineoplastic agents in hospitals [thesis] . [Seoul] : Seoul National University, 1999.
- Kim KY. Development guideline for prevention &management of the extravasation [thesis] . [Seoul] : Yonsei University, 2008.
- Kim YM, Kil YK, Min J, Jung YY, Choi EK. Safety care. Seoul: Korean Nurses Association; 2009.
- Polovich M, White JM,& Kelleher LO.Chemotherapy and biotherapy: guidelines and recommendations for practice.2nd ed. Pittsburgh, PA; 2005.
- Abbott PA. Research in patient safety/error reduction: A nursing perspective. Session presented at post-conference for 8th International Congress in Nursing Informatics, Rio De Janeiro, Brazil; 2003.
- Choi JH, Lee KM, Lee MA. Relationship between Hospital Nurses' Perceived Patient Safety Culture and Their Safety Care Activities. J Korean Academy of Fundamentals of Nursing 2010;17(1):64-72.
- Kreuger RA. (1994). Focus groups: a practical guide for applied research. 2nd ed. Thousand Oaks, CA: Sage Publications, Inc. 1994.
- Hiesh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15:1277-1288.
- Spradley J. The ethnographic interview. New York: Holt, Rinehart, & Winston. 1979.
- SandelowskiM. The problem of rigor in qualitative research. Adv Nurs Sci1986:8(3): 27-37.
- Oh CA, Yoon HS. Perception and Experience of Medication Errors in Nurses with less than One Year Job Experience. Journal of Korean Acad Fundam Nurs 2007;14(1):6-17.
- Kettles AM, Moir E, Woods P, Porter S, Sutherland E. Is there a relationship between risk assessment and observation level? J Psychiatr Ment Health Nurs. 2004;11:156-164.
- Ann SH. Analysis of risk factors for patient safety management.J Korean Acad Nurs Admi. 2006;12(3):373-384.
- Ryou SY. A Study on Medication Errors and Preventives [thesis] . [Seoul] : Chung-Ang University; 2000.
- Hofler LD. Public reporting patient safety, and quality improvement the need for legalprotections.J Nurs Admi. 2005;35(4):161-162.
- Curtin LL. When negligence becomes homicide.Nurs Manag. 1995;28(7):7-8.
- Kohn LT, Corrigan JM, Donaldson MS. (Eds.). To err is human: building a safer health system. Washington, DC: NationalAcademy Press; 1999.
- Page AE. Keeping patients safe: Transforming the work environment of nurses. Institute of Medicine, Washington, DC: The National AcademiesPress, 2004.
- Kang JH, Kang HY, Kwon SH, Kim BR, Kim IS, Park MH, et al. Patient safety and nursing. Seoul: Hyunmoonsa; 2010.
- Kim EK, Kang MA, Kim HJ. Experience and Perception on Patient Safety Culture of Employees in Hospitals, J Korean Acad Nurs Adm 2007;13(3):321-334.
- Lee BY. Development and evaluation of nursing infobuttons on medication to prevent medication administration errors [thesis] . [Incheon] : Inha University; 2010.
- Park JS. Clinical nurses' level of compliance and related factors with work practice guidelines for personnel dealing with cytotoxic drugs [thesis] . [Daejeon] : Daejeon University; 2003.
- Cho HW, Yang JH. Relationship between Perceived Patient Safety Culture and Patient Safety Management Activities among Health Personnel, Journal of Korean Academy of Fundamentals of Nursing 2012;19(1):35-45.
- Kang MA, Kim JE, An KA, Kim Y, Kim SW. Physicians' perception of and attitudes towards patient safety culture and medical error reporting. Korean J of Health Policy and Adm 2009;15(4):110-135.

