Keywords
Breast cancer; Cost of living; Economic burden; Financial difficulties
Introduction
Breast cancer is a female problem which is increasing worldwide especially in developed countries [1]. The disease affects women in both physical and mental level due to the symbolism of the breast. When breast is removed, both women’s body image and their psychology are affected. On the other hand, cancer as an only meaning frightens people because it is a threat to life. The possibility of early diagnosis combined with the treatment, increase both the 5-year and the 10-year survival. At the same time patients are even more scared and worried because of the need for ancillary therapies which are associated with adverse effects [2,3]. The disease and its treatment cause tension and require lifestyle changes associated with the cost of living. So the question arises as to whether and to what extent the cost of living is influenced among women with early stage breast cancer who undergo adjuvant therapy over a period of one year after the initial treatment.
With the average cost of living, is meant the value in money for purchasing goods and services to meet the women’s needs and the plans required for their survival.
These are needs in regard to clothing, footwear, cosmetics, physical fitness, hairdo, leisure activities, travelling, communications, public spectacles, nutrition and health [4].
According to Perry et al., [5] experiences of women with breast cancer vary in different stages of disease progression. Generally, the initial diagnosis is accompanied by feelings of denial, anxiety, anger, sadness, fear, and sometimes, panic. Breast cancer is a disease which threatens women's life, but nowadays thanks to the improvement of antitumor drugs and early diagnosis due to mammography, it has become a chronic disease. But on the other hand it changes a patient’s life of the patient in several and significant ways. Frequently there is a need for adjuvant therapy, such as radiotherapy and chemotherapy, so a patient is forced to visit a hospital at regular intervals. This means that a patient has a lot of expenses which cannot be covered by the insurance company, such as travel and hotel expenses or even parking cost, while they are in hospital receiving treatment [6-9].
A reasonable question arises as to how patients react in terms of living costs. Some of them may cut down on expenses they used to make at the time of diagnosis due to the emerging needs of the disease and treatment. However, it is very possible that they are prone to increase living costs as a way of handling their problem and because at the same time they feel that life is getting shorter.
Aim
To estimate, the change in the cost of living for patients with early stage breast cancer during the first year, after diagnosis.
Methodology
The material of the study consisted of 181 patients aged 28-88 years with stage II breast cancer, 114 of whom, were admitted to the District Hospital "Agios Savvas", while 67 to a private Infirmary.
Selection criteria in the survey were the following: Women with stage II breast cancer who would need to undergo adjuvant therapy after the initial surgical intervention. Women who had not been hospitalized before for the same disease and they also had good communication skills.
The collection of material was based on a questionnaire containing questions about the cost of living for these women.
This questionnaire was constructed and validated in the Laboratory of Demography, Faculty of Nursing, at the University of Athens. It includes demographics, marital status, education level, employment status, compulsory insurance coverage and the costs for living expenses such as clothing and footwear costs, costs for personal needs (hairdresser, esthetician, fitness, cosmetics), health (vitamins or supplements for another disease), public entertainment (visits to the theater and cinema), participation in social events (visits to coffee shops, restaurants, attendance at weddings, christenings or visiting friends, receiving friends at home), transportation (costs for petrol, two-day trips), communication (frequency and costs of telephone calls using home and mobile phones), and costs for tobacco use (number of cigarettes per day and purchase cost).
Permission was asked and obtained from Hospitals Ethics’ Committee, in order to get in touch with the patients.
The data collection which concerned a convenience sampling began in May 2006 and ended in June 2008. The data collection of the study was conducted by the researcher through interviews at two times apart: at the time of diagnosis and first admission to the hospital two days prior to surgery (first estimate) and a year later, when the patients arrived at the hospital for the follow-up examination (second estimate). One of the 181 patients died during the first year after diagnosis and four patients stated that they wished to discontinue with the study. The approach to patients for their participation in the study sample was as follows: after study of medical records in order to meet the criteria for participation in the study sample, patients were approached and informed about its purpose and objectives. Following informed consent procedures, the patients were interviewed.
Statistical Analysis
The normality of quantitative variables was checked using the Kolmogorov-Smirnoff test. Apart from the variable “age” all the other variables did not follow the normal distribution. For those variables which do not follow the normal distribution, Wilcoxon statistical test in pairs was used.
In quantitative variables, the average, the median, the standard deviation and percentages were calculated. The qualitative variables were calculated as percentages.
All statistical tests were performed at a significance level a=0.05. For the statistical analysis, the statistical package SPSS (15) was used.
For the statistical analysis, the results were used as they were collected. For the presentation of the results, however, they were grouped in several variables as follows:
The variables relating to the frequency of purchase goods and services in the past three months grouping was as follows: 0, 1, 2, 3, and ≥ 4.
The variables relating the cost of buying goods and services in the past three months, grouping was as follows: 0, 1-100, 101-200, 201-300, 301-400, 401-500, ≥ 501.
The variables studied are presented in Table 1.

Results
The average values of the quantitative variables related to the cost of living in the time before and during the year after diagnosis revealed the following results (Tables 2-5).
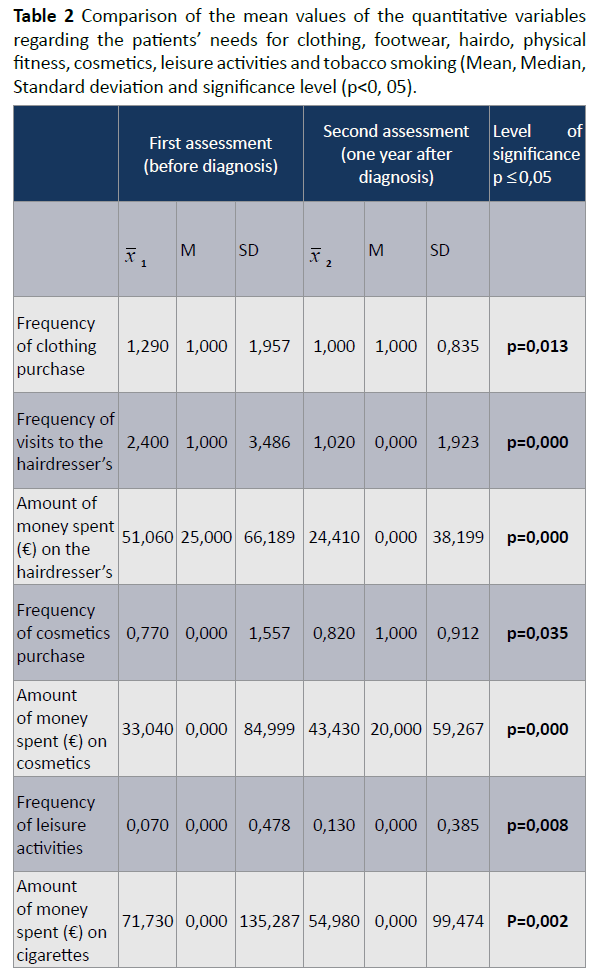
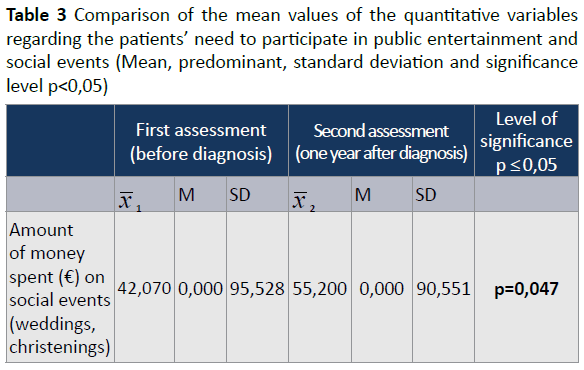
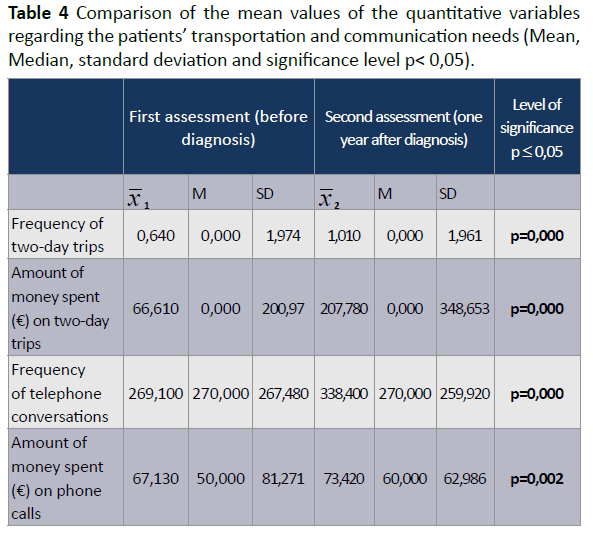

Table 2 shows the comparison of the mean values of the quantitative variables in the cost of living, which also refer to patients’ external appearance, at the time of the first estimation (before diagnosis) and at the time of the second estimation (one year after diagnosis of the disease).
Table 2 shows that:
• The frequency of purchasing clothing was decreased at the time after diagnosis of the disease (2=1,00) compared to the time before diagnosis of it (1=1,29) and shows a statistically significant difference (p=0,013).
• The frequency of visits to the hairdressers’ was decreased at the time after diagnosis of the disease (2=1,02) compared to the time before diagnosis of it (1=2,40) and shows a statistically significant difference (p=0,000).
• The frequency of expenditure on visits to the hairdressers’ was decreased at the time after diagnosis of the disease (2=24,41) compared to the time before diagnosis of it (1=51,06) showing a statistically significant difference (p=0,000).
• The frequency of cosmetics purchase was increased at the time after diagnosis of the disease (2=0,82) compared to the time before diagnosis of it (1=0,77) and appears statistically significant difference (p=0,035).
• The frequency of expenditure on visits to cosmetic stores was increased at the time after diagnosis of the disease (2=43,43) compared to the time before diagnosis of it (1=33, 04) shows a statistically significant difference (p=0,000).
• The frequency of involvement with leisure activities was increased at the time after diagnosis of the disease (2=0,13) compared to the time before diagnosis of it (1=0,07) and shows a significant difference p ≤ 0,05 (p=0,008).
• The frequency of the number of cigarettes the patients smoked during a day was decreased at the time after diagnosis of the disease (2=4, 20) compared to the time before diagnosis of it (1=5,53), and shows statistically significant difference (p=0,000).
• The Frequency of cigarette expenditure was decreased at the time after diagnosis of the disease (2=54,98) compared to the time before diagnosis of it (1=71,73), and shows statistically significant difference (p=0,002).
Table 3, shows the comparison of the mean values of the quantitative variables regarding the patients’ need to participate in social events and public entertainment.
Table 3 shows that:
• The frequency of expenses for participation in social events was increased at the time after diagnosis of the diseases (2=55,20) compared to the time before diagnosis of it (1=42,07) showing a statistically significant difference (p=0,047).
Table 4 shows the comparison of the mean values of the quantitative variables regarding the patients’ transportation and communication needs.
Table 4 shows that:
• The frequency of a two-day excursions was increased at the time after diagnosis of the disease (2=1, 01) compared to the time before diagnosis of it (1=0,64) showing a statistically significant difference (p=0,000).
• The frequency of expenditure on two-day trips was increased at the time after diagnosis of the disease (2=207,78) compared to the time before diagnosis of it (1=66,61) showing a statistically significant difference (p=0,000).
• The frequency of telephone calls was increased at the time after diagnosis of the disease (2=338, 40) compared to the time before diagnosis of it (1=269,10) showing a statistically significant difference (p=0,000).
• The frequency of expenditure on telephone calls was increased at the time after diagnosis of the disease (2=73,42) compared to the time before diagnosis of it (1=67,13) showing a statistically significant difference (p=0,002).
Table 5 shows the comparison of the mean values of the quantitative variables regarding the patients’ health needs at the time before diagnosis of the disease and one year after it.
Table 5, shows that:
• The frequency of purchasing vitamins or dietary supplements was increased at the time after diagnosis of the disease (2=0, 28) compared to the time before diagnosis of it (1=0, 09), and shows a statistically significant difference (p=0,000).
• The frequency of expenditure on vitamins or dietary supplements was increased at the time after diagnosis of the disease (2=8, 03) compared to the time before diagnosis of it (1=2, 94), and shows a statistically significant difference (p=0,000).
Discussion
Study results cannot be compared with others since there is no such data in the Greek and international literature. Therefore, these results represent a first attempt to estimate the cost of living from this point of view. In the first year after diagnosis of the disease, there is a decrease in the frequency of clothing purchase by patients (p=0,013), without any reduction in expenditure for this purpose (p=0,209). Given the modifications required in clothing (special bras, prostheses, comfortable clothing), one would expect an increase in spending to meet those needs. Thus, patients may have made cheaper purchases compared to what they used to in order to cover these extra costs. During the data collection, the patients repeatedly emphasized the great difficulty to meet the emerging needs arising from the diagnosis and treatment of their disease. At the same time, other financial requirements arise, such as the need of transportation from home to hospital for treatment or follow-up (petrol, parking and hotel accommodation expenses, as these are referred by other studies. Similar results were seen in study of Arozullah et al. [6].
Study results showed that the visit to the hairdresser’s and their cost were significantly reduced (p=0,000) and (p=0,000), respectively. This finding was expected given the fact that chemotherapy causes hair loss which although reversible, leads patients to limit the visits to the hairdresser’s. On the contrary the frequency of visits to cosmetic stores and the expenditure on cosmetics stores one year after diagnosis was increased significantly (p=0,035) and (p=0,000), respectively. The fact that the disease affects negatively the body image leads patients to the purchase and use of cosmetics for improving their perception of themselves and their psychological well-being. Their involvement with leisure activities increased significantly (p=0,008), while the amount of money spent for this reason was not increased. Being involved with leisure activities improves the individual’s psychological state. The frequency of tobacco use was reduced (p=0,000) as well as the cost of buying cigarettes (p=0,002). This finding was expected given the fact that smoking is a harmfulness habit and is in agreement with another study [10].
There was an increase in the cost of participation in social events (p=0,047), without any significant difference in the frequency of patients participation in such events (p=0,811). The international literature shows that patients restrict their social activities, [11,12] however the present study showed an improvement in the patients’ social functioning. The financial burden due to the disease and its treatment, justifies the above finding. The frequency of two-day trips increased significantly as well as the amount of money spent on them (p=0,000) and (p=0,000), respectively. This finding could be explained by the fact that, people usually follow the modern demanding way of life and neglect themselves. The diagnosis of breast cancer makes patients think that such activities help them cope with their difficult health condition. It was also found that in the first year after diagnosis not only the frequency of telephone calls was increased (p=0,000), but also the amounts of money spent for this purpose (p=0,002) [13-15]. This finding could be explained by the women’s need to communicate more without necessarily going out of their house, given that the fatigue and hard feeling to adapt themselves socially and psychologically in the disease. The international literature shows similar findings [16-19]. There was also an increase in the purchase frequency of vitamins and dietary supplements (p=0,000), as well in the amounts of money spent for this purpose (p=0,000). Cancer and adjuvant therapies cause fatigue in patients and affect their physical functionality right after treatments This finding is supported by other research studies as well [20,21]. Moreover, the international literature shows that women with breast cancer turn to alternative therapies or herbal supplements [22,23]. This finding is in agreement with the results of other research studies.
Conclusions
This study is the first of its kind in Greece and aims to create a database and a reference field for further studies on the cost of living and health-related quality of life for patients with breast cancer in early stages.
The financial difficulties are an additional parameter to patient’s situation which must not be underestimated. Women amid financial difficulties increase the costs related to the improvement of their altered physical image rather than the emerging needs because of breast cancer.
The diagnosis of breast cancer makes patients think that leisure activities may help them cope with their difficult health condition.
Women use the telephone because they feel the need to communicate more without necessarily going out of their house given their fatigue and hard feeling to adapt themselves socially and psychologically in the disease.
Women with breast cancer turn to alternative therapies and herbal supplements, as they think they might help.
Limitations of the Study
The weaknesses and limitations of this study are based on the sampling methodology, the sample size and the used scale of measurement.
Despite the original design for repeated measurements, the study was conducted at two times apart, due to the nature of the disease of cancer as patients after completion of their treatment had to return home, in various parts of Greece. Moreover, patients showed no willingness to complete the questionnaires, most probably because of their emotional state, during the time of treatment.
Furthermore, the sample came from the largest cancer hospital in Athens (Agios Savvas) and a private Infirmary due to easy accessibility to these institutions. These centers were an important source for the selection of the particular sample, but this fact does not exclude the possibility that there was some type of selection bias (selection bias). The results might be different if used larger numbers of sub-groups were used. Although unequal sample sizes are very common in different studies, it is considered that relative importance of variables between subgroups cannot be accurately interpreted. In addition, under these circumstances, sampling was "opportunity" and not "shuffle", as well as voluntary. For the above reasons, the study results cannot be generalized.
Another limitation of the study is related to the "bias information» (information bias). The scale of data collection was based on selfreports so as no effect or behavior could not have been verified objectively. It is assumed that researchers can never be completely sure of the honesty of the responses. There is also the possibility that the results are affected by the poor level of information about patient's disease and prognosis, a phenomenon which is very common in Greece.
Finally, it should be noted that the interpretation of the results need to be considered with caution due to the direct comparisons with other studies which are complicated by differences in the research design, method, type, size of the study population and other factors.
6532
References
- Alipio BC, David FC, Isabel RS, Juan CNM. Manuel AE. Comparison of batch, stirred flow chamber, and column experiments to study adsorption, Desorption and transport of carbofuran within two acidic soils. Chemosphere. 2012; 88(1): 106-120.
- Arnaud B, Richard C, Michel S. A comparison of five pesticides adsorption and Desorption processes in thirteen contrasting field soils. Chemosphere. 2005; 61(5): 668-676.
- Chunxian W, Jin-Jun W, Su-Zhi Z, Zhong-Ming Z. Adsorption and Desorption of Methiopyrsulfuron in Soils. Pedosphere. 2011; 21(3): 380-388.
- Chunxian W, Suzhi Z, Guo N, Zhongming Z, Jinjun W. Adsorption and Desorption of herbicide monosulfuron-ester in Chinese soils. J Environ Sci. 2011; 23(9): 1524-1532.
- Christine MFB, Josette MF. Adsorption-desorption and leaching of phenylurea herbicides on soils. Talanta. 1996; 43(10): 1793-1802.

