Keywords
Indigenous knowledge; Local people; Medicinal plants; Traditional medicine; Wonchi district
Abbreviations: IK: Indigenous knowledge; MM: Modern Medicine; MP: Medicinal plants; TM: Traditional Medicine; TMPU: Traditional Medicinal Plant Use
Introduction
Ethno-botany studies the interaction between human and plants [1,2]. Since earlier time the daily livelihood of human depends on plants [1]. The humans indigenous knowledge on plant use come into view from the time when human experienced how to use plants; they get several benefits to fulfill their basic needs like food, shelter, fire wood, drugs and other several uses [1,3,4].
In the indigenous community of most developing countries traditional medicine plays a vital role in addressing health care needs of rural people and urban poor’ because modern medicine unable to meet the health care need of the community, so that the role of traditional medicine would not be diminished for the reason that it is culturally practicable and expected to remain reasonably priced [5,6]. The knowledge of traditional medicine in most cases has been remained through oral sharing experience. The traditional medicinal plant related information is less likely to be distorted since it is retained by healers as secrete. Thus, it is not easily reached to the public [7,8].
Due to the reason that the modern health care system unable to meet the health need of the community, majority of peoples of developing world including Ethiopian still depend on traditional plant medicine [9,10]. Although there is a substantial global interest in using the accumulated knowledge of traditional plant medicine to the well fare of the human population, related studies were scanty [11]. Thus, this study is aimed to assess the indigenous knowledge of medicinal plant use among local communities of Wonch District, Western Ethiopia.
Statement of the problem
Traditional medicine is an ancient form of health care practices since before appearance of scientific medicine. It has played and continues to have important role in providing curative services to very large number of people particularly in the rural areas of almost all countries of Africa. It is the custom of many people because of its accessibility teven in most remote areas, particularly in the community where care is given at low cost to patients in their home [11].
In many parts of Ethiopia, considerable numbers of researches have been done on the knowledge of traditional plant medicine [12]. Like in other parts of country, in the current study area, the knowledge on medicinal plants use become lesser and lesser due to its secrecy, unwillingness of young generation to gain the knowledge, influence of modern education, religious and awareness factors, which all results in gradual disappearance of indigenous knowledge on medicinal plants (Researcher long term direct observation). But there was no scientific research that had been done on the indigenous knowledge of community on the use of traditional plant medicine in the study area. Therefore, this study is aimed to identify the traditional medicinal plant species and associated knowledge of the community about their use in the study area. The finding of this study will help various stakeholders to document information related to indigenous knowledge towards traditional medicinal plant use before their total loss. That in turn helps to maintain the overall traditional medicine activities for the future generation. In addition, the finding of this study provided base line information for further study in the area.
Materials and Method
Descriptions of the Study area and period
This study was conducted in February 20 to May 25, 2019. In wonchi district. Wonchi is one of the Districts in the Southwest Shoa Zone, Oromia Region, Ethiopia, which is located 124 km away from Addis Ababa with the area coverage of 460,516 hectare and the altitude range between 1798m to 2118m above sea level. The district has a population of 119, 736 with almost equal gender ratio of 49.8% male and 50.2% female. Regarding Orthodox constitute more than half (58.9%) followed by Protestants (39.6%) [13]. Ecologically the district is divided in to dega/ high land/ (40%) and woinadega or mini land (60%). Due to variation in altitude and topographical features, the wonchi district vegetation shows three different zones, namely: Afro-montaneforest, sub alpine and afro-alipine) vegetation [14,15].
Regarding vegetation the common plant species of the study area include: Achyranthes- aspera, Albizias-chimperiana, Alchemilla-pedata, Apodytesdimidiata, Bruceaantidysenterica, Dombeya-torrida, Embeliaschimperi, Erica -arborea, Festucagil-bertiana, Lobelia rhyncho-petalum,Hagenia-abyssinica, Hypericumrevolutum, Jasminumabyssinicum, Juniperusprocera, Kniphofiafoliosa, Lobelia giberroa, Maytenusar-butifolia, Millettia-ferruginea, Nuxiacongesta, Oleacapensis, Oleaeuropaea subsp. caspidata, Papaneasimensis, Pittosporumviridiflorum, Prunusafricana, Phytolacadodicandra, Salix subserrata, Scheffler-aabyssinica, Thymus-schimperi and Zehneri-ascabra Vegetation [16].
Study design
Field survey design was employed to collect information about the indigenous knowledge of traditional medicinal plant use of from local people in the study area. During the survey, both quantitative and qualitative data were collected.
Reconnaissance surveys
Preliminary survey was conducted from February 20- 25, 2019. During the preliminary survey general information about the study area were gathered. Sampling technique, Kebeles to be selected, informants and study sites were determined bases on the information preliminary survey.
Study site selection
From a total 23 Kebeles in the District, nine study Kebeles were selected purposively based on availability of key informants following the recommendation of government officials, stakeholders, and religious leaders during reconnaissance survey. The sampled Kebeles are (Belbela, Dimtu, Fite, Harowanch, Kurfogute,Lemenmetahora, Mitiwelga, Sonkolekake, Waldotelfa).
Informant Selection
A total of 198 informants were selected. From these 27 were key informants (3 informants per Kebele) were selected purposively and 171 of them were general informants (19 per Kebele) were selected randomly (lottery method). Age range of informants selected for the study were from 20 to 80 who lived 5 year and above in the study area. The size of the sample depends on the available fund, time and other reasons and not necessarily depends on total population [17].
Data collection method
Semi-structured interview, observation and guided field walks with informants were employed [18]. Interview was based on a checklist of questions prepared beforehand in English and translated to local languages (Afaan Oromo). Information regarding indigenous knowledge of medicinal plants use was recorded at the spot. Guided field observation was made to cheek the availability of the plant in the area, to know the habit and habitat of the plant. Focus group discussion was also made to get more information about medicinal plants use, the associated indigenous knowledge and reliability of the information collected during individual interview.
Data analyses
Descriptive statistics was used to analyze the data. The results were summarized and displayed in narrative and tables/figures/ by using frequency and percentage. The most useful information gathered about medicinal plants that was presented in descriptive statistics include name of the plant, methods of preparation, route of application, disease treated, and parts used and the habit of the plant.
In addition, ethnobotanical scoring and ranking methods were used to analyze medicinal plants in the area. From these, Paired-wise comparison was used to analyze the effectiveness of five medicinal plants used to treat malaria using six selected key informants. The number of pairs was calculated using the formula n (n-1)/2 [1]. Where, n, is number of medicinal plants to be analyzed.
Informant consensus was used to analyze ten most frequently mentioned traditional plants in the study area. Preference ranking was also used to analyze six medicinal plants claimed to treat hypertension.
Informant consensus factors (ICF)
This method is used when healers and other randomly used informants claim a particular MP to be used for some general disease categories. ICF is a good measure of assessing efficacy of MPs for categorical disease at least in the context of the indigenous people of the area, and it is a means to find out the most common disease of the study area in the context of their experience. In order to evaluate the reliability of information recorded during the interview, informants were contacted at least two times for the same ideas and the validity of the information was proved and recorded. Consequently, if the idea of the informant deviated from the original information, it was rejected since it was considered irrelevant information. As a result, only the relevant ones were taken into account and statistically analyzed [17].
Preference ranking
In this study area a total of fourteen medicinal plants claimed to treat malaria. Preference ranking activities were carried out following Martin [1]. These were for the most preferred medicinal plants. Accordingly, twenty seven randomly selected key informants were asked to rank six medicinal plants which are used for treatment of wound, based on high frequency of disease reported by randomly selected informants, they were selected for the preference ranking exercise of six most important medicinal plants. The values given for this application ranged from six (for the highest important) to one (for least important). Finally, total score were identified and the rank of each species was stated by numeric values. These helped to indicate the most effective medicinal plants for wound.
Paired comparison
It was applied to determine the most important plant species for stomach ache based on the information perceived by the informants. The number of pairs was calculated by the formula, n (n-1)/2, where n is the number of items. After identifying five plant species which have high use value to stomachache treatment by preference ranking, paired comparison was carried out after randomizing both sequences of the pairs and others within each pair. The sequence of pairs was randomized by numbering the pairs from 1-10 in alphabetical order and pulling numbered slips out of that, while the order within each pair was done by flipping a coin. If the original order of the species was maintained for head, but the order was switch around for tails. Finally, the numbers were added for all respondents giving on over all scores which were ranked for the species [1].
Ethical approval
Written ethical clearance was obtained from the Research and Ethical committee of the Department of Biology Gondar University. A formal letter was written to Wonci district health and agriculture office from department of Biology. On the basis of this, permission was obtained from the district health and agriculture office and each kebele administration to conduct the study. Written informed consent was sought and obtained from every participant who decided to take part in the study. They were assured about the confidentiality of their responses.
Results and Discussion
Socio-demographic characteristics of respondent’s
A total of 198 informants including 27 key informants were selected. Most (77.8%) of the respondents were males. Around half (51.5%) of respondent’s age range was from 40-60. Majority (86.86%) of the participants was married. Almost all religious leader respondents were followers of Orthodox Christian. Regarding educational status from all respondents 20.7% were illiterate. Number of farmers’ respondents predominated (33.33%) other respondents while NGO workers are lower in number (5.05%) (Table 1).
| Variables |
Response option |
Frequency |
Percentage (%) |
| Sex |
Male |
154 |
77.77 |
| |
Female |
44 |
22.23 |
| Age |
20-40 |
14 |
7.07 |
| |
41-60 |
102 |
51.51 |
| |
61-80 |
82 |
41.41 |
| Marital status |
Single |
12 |
6.06 |
| |
Married |
171 |
86.86 |
| |
Windowed |
15 |
7.57 |
| Religion |
Orthodox Christian |
142 |
71.71 |
| |
Muslim |
27 |
13.63 |
| |
Waqefata |
25 |
12.62 |
| |
Others |
4 |
2.02 |
| Education |
Illiterate |
41 |
20.7 |
| |
Primary |
67 |
33.8 |
| |
High school and above |
90 |
45.5 |
| Occupational status |
Farmers |
66 |
33.33 |
| |
Merchants |
25 |
12.62 |
| |
Government employee |
36 |
18.18 |
| |
NGO worker |
10 |
5.05 |
| |
Others |
61 |
30.8 |
Table 1 Socio-demographic characteristics of respondents wonchi district 2019(n=198).
Medicinal plant composition and habitats
A total of 93 medicinal plants belonging to 86 genera and 51 families were documented from the study area. Out of these, 50 species (53.76%) were noted to treat only human ailments while 3 species (2.23%) were used to treat livestock ailments and 40 species (43.01%) were used to treat both human and livestock ailments. In terms of species composition, family Asteraceae was represented by a highest number of medicinal plants species (7 species) followed by Solanaceae (6 species), Lamiaceae and Euphorbiaceae (5 species each) (Figure 1).
Figure 1 Map of the Study Area.
From the total of 93 medicinal plant species documented in the district, 60 species (64%) were collected from the wild/natural vegetation and this indicated that there is a significant harvesting pressure on the wild plant source of the study area. The remaining percent, constitute 6 species (7%) were collected both from cultivated and wild vegetation whereas 27 species (29%) were collected from cultivated fields (Figure 2). This is consistent with the findings of previous study that showed traditional medicinal plants were harvested mostly from wild vegetation followed by home gardens [18] (Table 2).
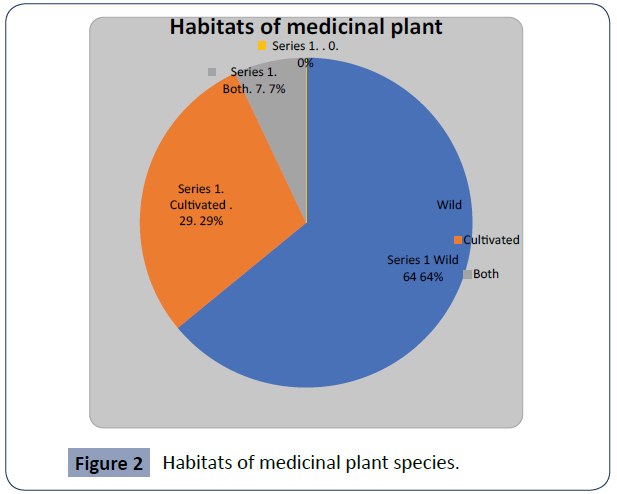
Figure 2 Habitats of medicinal plant species.
| Respondents |
Male |
Female |
Total |
Percentage (%) |
| Farmers |
26 |
7 |
33 |
16.66 |
| Merchants |
16 |
9 |
25 |
12.62 |
| Religious leaders |
26 |
6 |
32 |
16.16 |
| Health care workers |
26 |
10 |
36 |
18.18 |
| Traditional plant medicine users |
46 |
8 |
54 |
27.27 |
| Traditional plant medicine healers |
14 |
4 |
18 |
9.1 |
| Total |
154 |
44 |
198 |
100 |
Table 2 Distribution of informant groups by number.
Informant consensus
Informant consensus analysis was performed on ten most frequently mentioned species and the result showed that Citrus limon had the highest informant agreement which is mentioned by 82 (41.41%) informants followed by Acacia abyssinica which is reported by 70(35.35%) informants. Verbascumsinaticum had got least informant agreement (25.25%) from the top ten species followed by Vernoniahymenolepis with 25.75% informant consensus (Table 3).
| Species name |
No. of reports |
Percentage (%) |
Rank |
| Citrus limon |
82 |
41.41 |
1st |
| Acacia abyssinica |
70 |
35.35 |
2nd |
| Rumex nervous |
67 |
33.83 |
3rd |
| Achyranthesaspera |
65 |
32.82 |
4th |
| Daturastramonium |
58 |
29.29 |
5th |
| Bruceaantidysenterica |
57 |
28.78 |
6th |
| Calpurnia aerea |
55 |
27.77 |
7th |
| Kalanchoepetitiana |
53 |
26.76 |
8th |
| Vernoniahymenolepis |
51 |
25.75 |
9th |
| Verbascumsinaticum |
50 |
25.25 |
10th |
Table 3 Informant consensus for ten most frequently mentioned traditional plant medicines.
Medicinal plant parts used and habits
Out of the total 93 medicinal plants collected from the study area, 34 (36.56%) were herbs species followed by 31 (33.33%) shrubs species (Figure 3). This may be due to a high level of abundance of these habits in the study area compared to tree and climber species. Relatively high number of herbs and shrubs for the medicinal purpose has also been reported previous [19- 22]. In contrast, the findings of some other studies revealed that shrubs were the most used ones [18,23,24].
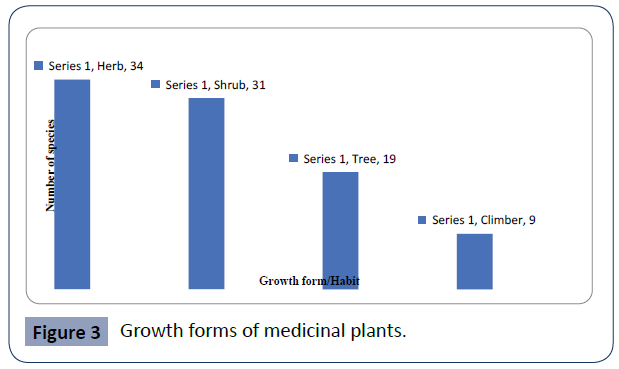
Figure 3 Growth forms of medicinal plants.
The study showed that the widely used plant part for the preparation of the remedies in the study area were leaves (28,40%) followed by roots (13,18.57%) and seeds (9,12.86%). Plant parts such as stem, bark, fruit, and bulb were also reported for the remedy preparations (Table 4). The findings of the study showed that many plant parts were used for the preparation of the remedies in the study area. This finding is similar to the results of other ethno-medicinal studies [19,25,26] who had reported that leaves were the most cited plant parts used in remedy preparations. But a study conducted in Konso special wereda revealed that roots were the most used plant parts [27].
| Plant parts used |
The frequency of each uses |
(%) |
| Leaf |
28 |
40 |
| Root |
13 |
18.57 |
| Seed |
9 |
12.86 |
| Root and leaf |
7 |
10 |
| Stem |
6 |
8.57 |
| Bark and fruit |
4 |
5.71 |
| Above ground, bulb, tuber, fruit, and seed |
2 |
2.86 |
| Flower, rhizome, latex, root bark and shoot |
1 for each |
1.43 for each |
| Total |
70 |
100 |
Table 4 Knowledge of participant regarding Plant parts used in the preparation of the remedies.
Knowledge difference reported by informants
Regarding age most (94.62%) of medicinal plants were reported by elders, while only 10.75% of them were reported by younger age groups (20-40 years). This might be due to elder’s long year observation from medicinal plant practitioners and due to younger’s unwillingness to share such traditional medicine related knowledge. Some previous studies also showed similar finding and justified the reason as healers holding traditional medicine related issue as secrete, modern education also affect younger’s negatively in receiving knowledge from elders, rapid changing of culture to western also played its role [10,19,28-30]. Regarding occupation traditional plant medicine healers (key informants) are more knowledgeable than others, Almost all (96.77%) of TMP were reported by traditional healers followed by farmers (84.94%) while, few medicinal plants (21.50%) were reported by merchants (Table 5). This might be expected as medicinal plant healers are practitioners and their job depends on medicinal plants use and giving medicine for users, they had well-developed knowledge on plant species used to treats ailments ingredients and diluents used to prepare herbal medicine. However, it was also found that some of the key informants were not willing to report all the ingredients used to prepare particular herbal medicine. It was seen that the ingredient that could not be mentioned by one key informant was mentioned by another to prepare herbal medicine for the same ailments. Similarly farmer’s daily life is around garden and forest area this may help them to know more medicinal plants. The other studies also indicate this truth [31].
| Based on age |
|
Based on occupation |
|
Based on sex |
|
|
Based on religion |
Based on educational status |
|
| Age group |
No of TMP (%) |
Occupation (%) |
No of TMP (%) |
Sex |
No of TMP (%) |
Religion |
No of TMP (%) |
Educational. Level |
No of TMP (%) |
| 20-40 |
10 (10.75) |
Farmers |
79 (84.94) |
Male |
80 (86.02) |
Christian |
35 (37.63) |
Uneducated |
57(61.29) |
| 41-60 |
50 (53.76) |
Merchants |
20 (21.50) |
Female |
45 (41.85) |
Muslim |
56 (60.21) |
Able to read and write |
30(32.25) |
| 61-80 |
88 (94.62) |
Religious leaders |
47 (50.53) |
|
|
Waqefata |
70 (75.26) |
12 complete |
15(16.12) |
| |
|
Healthcare worker |
10 (10.75) |
|
|
Others |
5 (5.37%) |
10 complete |
9(9.67) |
| |
|
Healers |
90 (96.77) |
|
|
|
|
Diploma |
10(10.75) |
| |
|
|
|
|
|
|
|
Degree |
13(13.97) |
Table 5 Number of Medicinal plants reported by informants.
Regarding religion of informant Waqefata reported more TMP (75.26%) followed by Islamic religion followers (60.21%). While, Christianity followers reported less TMP (37.63%) next to others religion followers (5.37%) (Table 4). This might be due to the fact that waqefata religion followers follow their religion around home garden, forest, river, ponds, and stream. More TMP (86.02%) were reported by males but, females reported less traditional medicinal plants (41.85%) (Table 5). This might show that males move from place to place for their day to day life activity while females daily activity is around home. Other studies conducted in Ethiopia demonstrated similar results [32].
More TMP (61.29%) were reported by illiterate while literate reported less (38.71%). This may confirms that modern education and exposure to modernization limits the knowledge on traditional medicine. Similar result were reported in different studies conducted in various areas in the world [10,32] (Table 5).
Indigenous knowledge transfer on medicinal plants use
Most informants (60.60%) get knowledge about medicinal plant use from their parents; others (18.68%) from their friends and the rest (20.70%) get knowledge about TMP from other knowledgeable elders. The highest percentage (91.91%) of informants do not have written document about medicinal plant use practice, but few of them have written document (8.09%) (Table 6). The knowledge sources on how to use herbal medicine, dosage and antidotes, especially traditional medicinal use, vary from person to person. The findings showed that the sources of ethnobotanical knowledge are basically the family members (father, mother, brother and sister) friends and neighbors. On the same note, most of the informants around Gimbi town (Western Ethiopia) acquired traditional knowledge on medicinal plants from their parents and/or close relatives [33].
| Transfer of TPMU knowledge |
Development of traditional plant medicine use knowledge |
| Sources |
Number of informants |
Percentage (%) |
Way |
No. of informants |
Percentage (%) |
| Parent |
120 |
60.60 |
Direct observation |
108 |
54.54 |
| From friends |
37 |
18.68 |
Listening |
81 |
40.90 |
| Other knowledgeable elders |
41 |
20.70 |
Trial and error |
7 |
3.53 |
| |
|
|
Observing animals |
2 |
1.01 |
*TMPU: traditional medicinal plant use.
Table 6 knowledge Transfer and ways of development of traditional plant medicine use knowledge.
The desire of the local people to transfer and share their knowledge vary from one place to another in this study area as most were interested to transfer their knowledge to all their children and others to the first son, brothers and sisters, or friends. On the other hand, most of the key informants from both districts were willing to share their knowledge on use of traditional medicinal plants to the first son while few to all their children. In general, traditional healers show maximum secrecy in handling medicinal plant knowledge and the tendency of the local people to transfer the traditional medicinal practices knowledge is mostly to a chosen close person.
Ethnobotanical knowledge of medicinal plants of the study area was shown to be transferred from the older people to younger generations at household level, This knowledge is not existent in written form, their losses or distortion at every transfer is inevitable. Similarly previous studies [33] showed that traditional healers believed traditional medicine is effective if done within a family or with close relatives. This might be attributed to healers non volunteerness to show their practice to other individuals so they kept secret their knowledge and transfer only to their nearest family. This could also be attributed to the impact of modernization (access to school and modern health facilities) and the very poor system of sharing indigenous knowledge on medicinal plants with the younger generation.
It is obvious that those educated people consider traditional use of medicinal plants as harmful and backward and prefer to go to modern health facilities. Although those illiterate informants, prefer to use TMPs from healers because its cost is cheap (Table 6). The finding is similar for other cultural groups in Ethiopia [29,30,32,35-37].
Almost all (54.54%) of respondents developed their knowledge by direct observation from practitioners and others (40.90%) by listening, (3.53%) by trial and error and the rest (1.01%) by observing animals (Table 6) similarly, the result of previous study revealed similar findings [23,38].
Medicinal plant knowledge, use and transfer of knowledge to the young generation could be affected by religious, beliefs, modernization, acculturation, and environmental change [37- 40]. Ethnomedicinal knowledge diminishes with death of elderly knowledgeable members of the community since only a few young people are willing to acquire the knowledge [29]. In a similar fashion, the respondents in the study site also reported that the transmission of traditional knowledge is disrupted, because of modernization and rapid changes in people’s lifestyle. Indigenous people revealed that gathering and processing of many medicinal plants were restricted to traditional medicinal practitioners and their trainees. At family level, it is restricted to the elders followed by elder son or daughter or their trustworthy person when the mother or the father is getting old or near to die [29]. First-born children in the family are the main holder of responsibility in keeping the information and they are successor of their parents as well. Few others share to trustworthy and lovely neighbors and other blood relation persons. Exchange and knowledge sharing are also common among intimate key informants. The death of elderly custodians of certain traditional knowledge will mean loss of certain practices unless they are passed on to younger generations since folk knowledge among the wonch people like many traditional tribes, is orally transmitted.
It is observed that more than in oral or written communication skill transfer of knowledge system is in their beliefs and norms. However, in the study area, knowledge has been transferred from one generation to the next through the interaction of the communities.
A major problem observing during the study was that few of highly traditional skilled and knowledgeable persons are rigid to tell information even if, their knowledge was shared to the researcher by following different ethnobotanical methods. This is because, first, it is a means of income generation and their livelihood depends on the income they get out of it. Second, they believe that the medicinal plant is less effective in treating a certain ailment if everybody knows it. On the other hand, most of the time knowledgeable persons were locally said to be ‘mortuu’and or ‘Xonquyii’. They were also condemned as ‘sir mash’ (root excavators), and ‘ballasasabduu’ (leaf collector). Because of the above mentioned difficulties, the traditional medicine practitioners had forced to keep their knowledge and practices in secret. Nevertheless, farmers, students and other educated inhabitants are free to secrete out the information.
In comparison with males, females are sensitive and afraid of the taboo words forwarded by the local people. That is why the number of female informants in the study area was less than males’. This is consistent with previous study [30,40,41] (Table 6).
Conclusion
A study on medicinal plant indigenous knowledge in the area revealed that different level of knowledge with regard to traditional plant medicine use, i.e. difference in age, sex, work and education level has impact on the knowledge of the use of traditional plant medicine. Moreover, the result of this study revealed that, the knowledge of community about traditional plant medicine use is believed to be decline from time to time. Most medicinal plants collected and identified were herbs and all plant parts were used for preparation of remedies. However, the use of medicinal plants for multiple purposes is leading to depletion in an alarming rate. This is worthy because of some of the uses (Agricultural expansion, firewood, construction, forage, charcoal.) are the major destructive.
Threats that erode indigenous knowledge usually comes from secrecy, oral-based knowledge transfer, the unwillingness of young generation to gain the knowledge, unavailability of the species, the influence of modern education and awareness factors are the major ones.
The results of this study also showed that cultivation of plant species in and around home gardens for different purposes have great contribution to the conservation of medicinal plants and the associated knowledge.
Recommendations
• Based on the results of the study, the following recommendations are forwarded to the responsible stakeholders.
• Integrated conservation and management program on medicinal plants focused on awareness development and active involement of local community, governmental and non gevrmental bodies shall be practiced in the district.
• Raising awareness of community especially young generation on the traditional medicinal plants use and hence, documentation of the medicinal plants of the area needs to be continued.
• Avoid uprooting of the plant species for medicinal purpose particularly before its flowering, fruiting and/seeding. If possible, it is better to use other parts of the medicinal plants such as leaves instead of root to protect them from the risk of extinction
• Establishing traditional healers associations by providing supports like land, fund and assistances for cultivations of medicinal plants in the district would help to conserve medicinal plants and to transfer knowledge.
• The government should create possible conditions and include to the teaching curricula about traditional plant medicine use/enhance collaboration of traditional medicine with modern/
• The insights of religious institution and health care institution should be positive and work together with traditional healers who treat by using traditional medicinal plant medicine.
Declarations
Ethical approval
Written ethical clearance was obtained from the Research and Ethical committee of the Department of Biology Gondar University. A formal letter was written to Wonci district health and agricultureoffice from department of Biology. On the basis of this, permission was obtained from the district health and agriculture office and each kebele administration to conduct the study. Written informed consent was sought and obtained from every participant who decided to take part in the study. They were assured about the confidentiality of their responses.
Consent for publication
Not applicable.
Availability of data and materials
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Competing interests
The authors declare that they have no financial and non-financial competing interests.
Author contributions
GM was involved in the conception, design, analysis, interpretation, report and manuscript writing.
Acknowledgments
I extend my deepest gratitude to those who participated in the study for their time to provide relevant information. I wish to extend my thanks to data collectors and supervisors. I also indebted to all those who apply their effort.
40372
References
- Martin GJ (1995) Ethno botany: A method Manual. Chapman and Hall, London, pp: 265-270.
- Balick MJ, Cox PA (1996) Plants, people and culture: The science of Ethnobotany. New York, Scientific American Library, USA, pp: 228.
- Cotton CM (1996) Ethno botany: Principles and Applications. John Wiley and Sons Ltd., Chichester, England, pp: 347-374.
- Teketay D (2001) Deforestation, Wood Famine and Environmental Degradation in Ethiopia’s Highland Ecosystems: Urgent Need for Action. Northeast African Studies 8: 53-76.
- WHO (1979) The promotion and development of traditional Medicine. Technical Report Series 622, WHO, Geneva.
- Jansen PCM (1981) Spices, Condiments and Medicinal plants in Ethiopia, their Taxonomy and Agricultural Significance. Center for Agricultural Publishing and Documentation, Wageningen, Netherlands, pp: 327.
- Debela A, Abebe D, Urga K (1999) An overview of traditional medicine in Ethiopia: Prospective and Development Efforts. In: Ejigu T (Editor). J Ethiop Med Pract.
- Abebe D (1986) Traditional Medicine in Ethiopia. The attempt being made to promote it for Effective and letter utilization. SINET Ethiop J Sci pp: 61-69.
- Dawit, Ayelu A (1993) Medicinal plants and Enigmatic Health practice of Northern Ethiopian. Publishing House, Addis Ababa, Ethiopia.
- Gedife T, Hahn H (2003) The use of Medicinal Plants in self-care in rural central Ethiopia. J Ethnopharmacol 87: 155-161.
- 11. Addis G, Abebe D, Urga K (2001) A Survey of Traditional medicinal Plants in Shirka Ditrict, Arsi Zone, Ethiopia. Ethiop Pharm J 19: 30-47.
- Lata A, Etana T (2014) Assessment of knowledge, attitude and practice on practice on traditional medicine in lag hare dire dawatown, Ethiopia.
- Federal Demographic republic of Ethiopia (2008) Central statistics Agency (CSA), Agricultural sample survey. Addis Ababa, Ethiopia.
- Woldu Z (1999) Forest in the vegetation types of Ethiopia and their status in the geographical context. In: Edwards S, Demissie A, Bekele T and Haase G (Editors). Institute of Biodiversity Conservation and Research (IBCR), Addis Ababa, Ethiopia.
- Masresha G (2014) Diversity, Structure and Regeneration Status of Vegetation in Simien Mountains National Park, Northern Ethiopia: PhD. Dissertation. Addis Ababa University, Addis Ababa.
- Belay J (2016) Ethnobotanical Study of Traditional Medicinal Plants used by Indigenous People of Jigjiga district, Somali Regional State, Ethiopia: MSc.Thesis. Haramaya University, Haramaya.
- Alemayehu G (2010) Ethnobotanical Study of Medicinal Plants used by Local communitiesOfMinjar-Shenkora District, North Shewa Zone of Amhara Region, Ethiopia. J Med Plants Stud 3.
- Yineger H (2005) A Study on the Ethno botany of Medicinal Plants and Floristic Composition of the dry afro Montana Forest at Bale Mountains National Park, Ethiopia: M.Sc. Thesis. Addis Ababa University, Addis Ababa, Ethiopia.
- Beyene T (2015) Ethno botany of Medicinal Plants in Erob and GulomahdaDistricts,eastern Zone of Tigray Region, Ethiopia: PhD. Dissertation. Addis Ababa University, Addis Ababa, Ethiopia.
- Regassa T (2016) Vascular Plant Diversity and Ethnobotanical Study of Medicinal and wild edible Plants in Jibat, Gedo and Chilimo Forests, West Shewa Zone of Oromia region, Ethiopia: PhD. Dissertation. Addis Ababa University, Addis Ababa, Ethiopia.
- Tesfaye T (2016) Use and Management of Medicinal Plants by People of Melka Belo District, East Hararghe, Oromia Region, Ethiopia: M.Sc. Thesis. Haramaya University, Haromaya, Ethiopia.
- Chekole G, Asfaw Z, Kelbesa E (2015) Ethnobotanical Study of Medicinal Plants in the environs of Tara- Gedam and Amba Remnant Forests in Libo Kemkem District. J Ethnobiol Ethnomed 11.
- Tamene S (2011) An Ethnobotanical Study of Medicinal Plants In Wondo Genet natural Forest and Adjacent Kebeles, Sidama Zone, SNNP Region, Ethiopia. Addis Ababa University, Addis Ababa, Ethiopia.
- Amenu E (2007) Use and Management of Medicinal Plants by indigenous People EjajiArea (ChelyaWereda) West Shewa, Ethiopia: An Ethnobotanical Approach, M.Sc Thesis. Addis Ababa University, Addis Ababa, Ethiopia.
- Kuma M (2014) Use and Management of Medicinal Plants by Indigenous People of Jima Rare District in Oromia Region, Ethiopia: M.Sc. Thesis. Haramaya University, Haramaya.
- Gebre T (2007) An ethno botanical study of medicinal plants in konso special district, Southern nations, and nationalities and people’s regional state, Ethiopia M.Sc.Thesis. Addis Ababa University, Addis Ababa, Ethiopia.
- Fassil H (2003) A qualitative understanding of local traditional knowledge and medicinal plant use. IK Notes 52: 1-4.
- D Hunde, Asfaw Z, Kelbessa E (2004) Use and Management of Ethnoveternary Medicinal Plants by Indigenous People in Boosat, Welenchitiarea. Ethiopia J Biol Sci 3: 113-132.
- Lulekal E, Asfaw Z, Kelbessa E, Van Damme P (2013) Ethnomedicinal Study of plants used for human ailments in Ankober District, North Shewa Zone, Amhara Region, Ethiopia. J Ethnobiol Ethnomed 9: 63.
- Berhe (1995) Women Lead in Protecting Food Germ plasm and Herbs for Health in Ethiopia (unpublished). Report Submitted to Earth Care Africa, Nairobi, Kenya.
- Awas T, Demissew S (2009) Ethnobotanical study of medicinal plants in Kafficho people, southwestern Ethiopia. In: Plant Diversity in Western Ethiopia: Ecology, Ethnobotany and Conservation. The University Foundation for Student Life (Sio), University of Oslo, Norway, pp:1-15.
- Etana T (2007) Use and conservation of traditional medicinal plants by indiginous people in Gimbidistirct, western wollega, Ethiopia, M.Sc. thesis. AAU, Ethiopia.
- Fullas F (2001) Ethiopian Traditional Medicine: Common Medicinal Plants in Perspective Edition. Fekadu Fullas: Iowa, Ethiopia.
- Giday M, Ameni G (2003) An Ethnobotanical Survey on Plants of Veterinary Importance in two Woredas of Southern Tigray, Northern Ethiopia. SINET Ethiopian J Sci 26: 123-136.
- Bekalo TH, Woodmatas SD, Woldemariam ZA (2009) An ethnobotanical study of medicinal plants used by local people in the lowlands of Konta special Wereda, Southern Nations, Nationalities and People Regional State, Ethiopia. J Ethnobiol Ethnomed 6: 25.
- Kidane B, van der Maesen LJG, van Andel T, Asfaw Z (2014) Ethnoveterinary medicinal plants used by the Maale and ari ethnic communities in Southern Ethiopia. J Ethnopharmacol 153: 274-282.
- Kassa Z (2009) An ethnobotanical study of medicinal plant biodiversity of trees and Shrubs in JelduWereda, Western Shoa, Ethiopia. M.Sc. Thesis Addis Ababa University, Addis Ababa, Ethiopia.
- Cunningham A (1996) People, Park and Plants use recommendations for multiple use zones and development alternatives around Bwindi: Impenetrable National Park, Uganda. In: People and Plants: Working Paper, UNESCO, Paris, pp: 18-25.
- Mesfin T, Lemma M (2001) The role of traditional herbal medicine and its constraint in the animal health care system in Ethiopia. In: Medhin Z, Abebe D (Editors). Conservation and Sustainable use of medicinal plants in Ethiopia, Institute of Biodiversity, conservation and research, Addis Ababa, Ethiopia, pp: 22-28.
- Etana B (2010) Ethnobotanical Study of Traditional Medicinal Plants of GomaWoreda Jima Zone of Oromia Region, Ethiopia: M.Sc. Thesis. Addis Ababa University, Addis Ababa, Ethiopia.

