Robert Oziegbe Akhigbe1, Anthony Chukwuka Ugwu2, Michael Promise Ogolodom3*, Nnenna Ihua4, Beatrice Ukamaka Maduka5 and Bolaji Israel Jayeoba6
1Rovina Medical Diagnostic Services, Lagos State, Nigeria
2Department of Radiography and Radiological Sciences, Faculty of Health Science and Technology, Nnamdi Azikiwe University Anambra State, Nigeria
3Rivers State Hospitals Management Board, Port Harcourt, Rivers State, Nigeria
4Department of Medical Laboratory Science, Rivers State University, Port Harcourt, Nigeria
5Department of Medical Radiography and Radiological Sciences, University of Nigeria Enugu Campus, Nigeria
6Nigerian Air Force Reference Hospital, Nigerian Air Force Base, Port Harcourt, Rivers State, Malaysia
*Corresponding Author:
Michael Promise Ogolodom
Rivers State Hospitals Management Board
Port Harcourt, Rivers State
Nigeria
Tel: +234803997393
E-mail: mpos2007@yahoo.com
Received date: 18 January 2019; Accepted date: 29 January 2019; Published date: 05 February 2019
Citation: Akhigbe RO, Ugwu AC, Ogolodom MP, Ihua N, Maduka BU, et al. (2019) Evaluation of Chest Radiographic Patterns and Its Relationship with Hematological Parameters in Patients with Pulmonary Tuberculosis in Lagos Metropolis, Nigeria. Health Sci J Vol.13.No.1:628.
Copyright: © 2019 Akhigbe RO, et al. This is an open-access article distributed under the terms of the creative commons attribution license, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Keywords
Chest radiographic patterns; Hematological parameters; Pulmonary tuberculosis
Introduction
Pulmonary Tuberculosis (PTB) is a contagious bacterial infection that mainly involves the lungs, but may spread to other organs and is caused by the bacteria Mycobacterium tuberculosis [1-3]. The disease spreads by droplet infection when people suffering from PTB (Pulmonary Tuberculosis) expel bacteria, for example by coughing. Tuberculosis (TB) is a major cause of morbidity and mortality throughout the world [4]. One third of the world’s population is infected with the TB bacillus [4]. The WHO cites TB as the single most important fatal infection, with around 8.8 million new cases and 1.4 million deaths per year with 95% in developing countries [4]. Tuberculosis is a major public health problem in Nigeria with an estimated prevalence of 616 cases per 100,000. Nigeria ranks first in Africa and eleventh among the 22 high TB burden countries in the world [5-7]. No fewer than 460,000 cases of tuberculosis are reported annually in Nigeria [4]. Patients with pulmonary tuberculosis may present with protean clinical manifestations and its diagnosis may prove quite difficult sometimes. But, since it is a curable disease, accurate diagnosis is essential. The definitive diagnosis of pulmonary tuberculosis is commonly the isolation of the tubercle bacilli from the patients’ sputum, either by direct microscopy or by culture. Chest radiography has been used over the years for the diagnosis of pulmonary TB. However, it is limited by modest specificity and a high interobserver variability in radiological reports [4]. Cohen et al. [8] found a sensitivity of 73%-79% and a specificity of 60%-63% in a high risk population. Similar results were found by Kisembo et al. [9] who compared the diagnostic value of typical TB symptoms (cough, sputum production, fever, weight loss, night sweats, hemoptysis, anorexia, and dyspnea) with chest radiograph in TB prevalence survey. A simplified scoring system has been recently proposed for reliable diagnosis of TB on chest radiograph [1]. The features on chest radiograph include: upper lobe opacities, cavities, unilateral pleural effusion and mediastinal and hilar adenopathy (Figure 1). Pulmonary tuberculosis may produce reversible abnormalities of peripheral blood. Tuberculosis can cause diverse hematological abnormalities such as anemia, increased erythrocyte sedimentation rate and thrombocytopenia [3,10,11]. Hematological abnormalities have been associated with TB and response to drug therapy [5,12,13]. The rate at which new TB cases occur varies widely, even in neighboring countries, apparently because of differences in health care systems and the changes associated with TB have been incompletely investigated [14,15]. Hematological profiles are those parameters of the blood forms (red blood cells, white blood cells and platelets) with normal range or value as reference for any value to know whether or not they are normal [13,16]. Rise in hemoglobin and hematocrit levels are used as markers reflecting response to treatment in pulmonary TB patients [5,13,16]. Decrease in platelet count and in white cell count and reduction in Erythrocyte Sedimentation Rate (ESR) were regarded as good indicators to observe drug response and disease control. Previous study has shown that anaemia, raised ESR, peripheral leucocyte count and neutrophilia are the most common hematological manifestations associated with PTB [17]. Pulmonary tuberculosis is a major public health concern in Nigeria where there are approximately 616 cases of TB per 100,000 people. However, rates vary dramatically by area of residence and socioeconomic class [3,4]. The morbidity of tuberculosis has direct relationship with hematological indices and could also manifest as presentations on chest X-ray [1,5,13,16]. To the best of our knowledge there is no documented study evaluating hematological parameters in patients with pulmonary tuberculosis and their relationship with chest X-ray patterns in Lagos Metropolis, Nigeria. Therefore, this study was designed to investigate the relationship between the various chest radiograph patterns and hematological parameters in patients with pulmonary tuberculosis in Lagos Metropolis. The following specific objective was also assessed; to investigate the correlation between chest radiographic patterns and hematological parameters such as (Hb, WBC, platelet count and ESR).
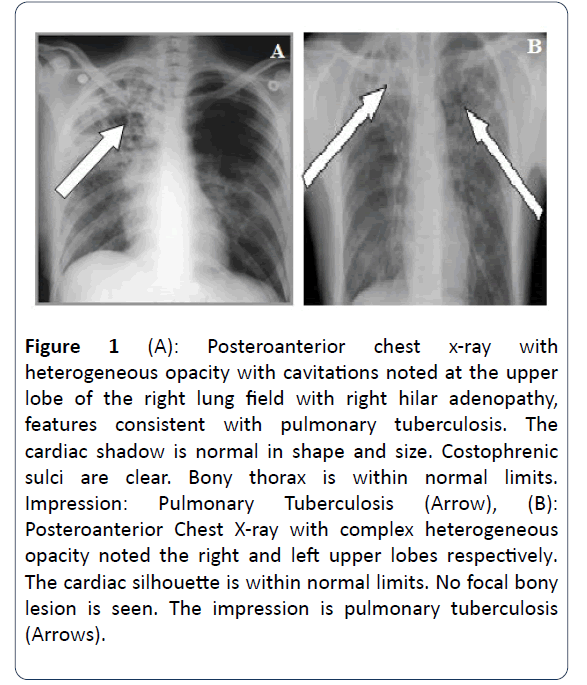
Figure 1 (A): (A): Posteroanterior chest x-ray with heterogeneous opacity with cavitations noted at the upper lobe of the right lung field with right hilar adenopathy, features consistent with pulmonary tuberculosis. The cardiac shadow is normal in shape and size. Costophrenic sulci are clear. Bony thorax is within normal limits. Impression: Pulmonary Tuberculosis (Arrow), (B): Posteroanterior Chest X-ray with complex heterogeneous opacity noted the right and left upper lobes respectively. The cardiac silhouette is within normal limits. No focal bony lesion is seen. The impression is pulmonary tuberculosis (Arrows).
Materials and Methods
This is prospective cross sectional study which was a collaborative work that involved the Radiology department, Medical laboratory department and the TB clinic at the Badagry general Hospital. The TB status of the subjects was confirmed by culture of the sputum for Mycobacterium tuberculosis. The anthropometric variables (Height in meters, weight in kg, and Body mass index BMI in kg/m2) for all the subjects were measured and recorded. All confirmed TB subjects at the time of diagnosis were subjected to chest X-ray investigation, ESR measurement and Full blood count analysis. The reports were recorded with the subject’s biodata and anthropometric variables (Height, weight, BMI). Chest X-ray with standard protocol and parameters were performed by a licensed Radiographer using GE static X-ray unit with an erect bucky stand. Chest radiographs were interpreted by two independent certified consultant radiologists. The Full blood count to determine hematological parameters such as Packed Cell Volume (PCV), White blood cell count and platelet count used in this study was conducted by council certified Medical Laboratory scientist using SWELAB Haematology analyzer (Manufactured by Sysmex Corporation Kobe, Japan). The inclusion criteria includes; confirmed TB patients aged 18-65 years at the TB clinic within the study period, all confirmed TB patients who consented to participate in the study and those that did not meet the inclusion criteria were excluded. A total of 181 subjects formed our sample size calculated using Yamane’s Formula [18] using non-probability sampling method based on the study inclusion criteria.
In accordance with Helsinki Declaration, approval for this study was obtained from the Human Research Ethical Committee (HREC) of the Lagos University Teaching Hospital. The procedure was explained to the subjects including the study aims and written informed consent was obtained from each subject before enrolling into the study. Data collection was done using structured proforma and were analyzed using Statistical Package for Social Sciences SPSS (Version 21) software. The statistical analysis was performed using both descriptive and inferential (Correlation analysis and Chisquare) statistical tools with statistical significance set at p<0.05.
Results
Table 1 demonstrates the anthropometric variables between the male and female participants. Significant difference was observed in Age (Male=34.77 ± 9.23 years; Females=32.16 ± 8.72 years; t=-3.249, p=0.001), Weight (Male=48.89 ± 13.02 kg; Female=45.08 ± 8.24 kg; t=-9.039, p=0.000) and BMI (Male=19.37 ± 2.66 kg/m2; Female=17.00 ± 4.12 kg/m2; t=-8.478, p=0.000). No significant mean difference was found in height. Table 2 shows frequency distribution of hematological parameters of the participants. All the participants had elevated ESR, 98.8% showed reduced PCV, 71.2% of the participants had raised lymphocytes count while about 95% of the participants recorded normal platelet count.
| Parameters |
Group |
Mean ± SD |
t-value |
p-value |
| Age (years) |
Male |
34.77 ± 9.23 |
-3.249 |
0.001 |
| Female |
32.16 ± 8.72 |
| Height (m) |
Male |
163.07 ± 6.26 |
-1.635 |
0.103 |
| Female |
162.08 ± 7.19 |
| Weight (kg) |
Male |
48.89 ± 13.02 |
-9.039 |
0 |
| Female |
45.08 ± 8.24 |
| BMI (kg/m2) |
Male |
19.37 ± 2.66 |
-8.478 |
0 |
| Female |
17.00 ± 4.12 |
Table 1 Sex distribution of anthropometric parameters studied.
| Hematological Indices |
Graded Ranges |
n (%) |
| ESR (mm/hr) |
Normal Range |
0-20 |
- |
| High Range |
>20 |
181 (100%) |
| Hb (g/dl) |
Normal Range |
11.5-16.5 |
5 (2.76%) |
| Low Range |
<11.5 |
176 (97.24%) |
| Lymphocytes (%) |
Normal Range |
20-40% |
49 (27.07%) |
| Low Range |
<20% |
3 (1.66%) |
| High Range |
>40% |
129 (71.27%) |
| Platelets /cmm |
Normal Range |
150000-450000 |
172 (95.03%) |
| Low Range |
<150000 |
9 (4.97%) |
| High Range |
>450000 |
- |
| PCV (%) |
Normal Range |
37-52 |
2 (1.1%) |
| Low Range |
<37 |
179 (98.89%) |
Table 2 Distribution of hematological indices among tuberculosis patients n=181.
Chi-square result showed statistically significant difference in distribution of tuberculosis patients in the various age ranges (χ2=74.792, p=0.000). The highest percentage of tuberculosis patients was found in age category below 30 years, and the least percentage in age category above 50 years (Table 3). Chi-square result showed statistically significant difference in distribution of tuberculosis patients in the various body weight categories (χ2=90.740, p=0.000). The highest percentage of tuberculosis patients was found in the normal body weight category (60.2%) and the least percentage in the overweight category (2.8%). 37% of the patients were in the underweight category (Table 4). The result of correlation analysis of the hematological parameters and the various patterns of chest radiographs showed that there was no statistically significant correlation between ESR (r=-0.649, p=0.16), WBC (r=-0.325, p=0.53) PCV (r=0.0549, p=0.26), Hb (r=0.488, p=0.33), platelets (r=-0.193, p=0.71), lymphocytes (r=-0.283, p=0.59), esosinophils (r=0.380, p=0.46) and basophils (r=-0.587, p=0.22) and the various patterns of chest radiographs studied, but there was a statistically significant correlation between the various patterns of chest radiographs identified in this study and monocytes (r=0.879, p=0.02) (Table 5 and Figure 2). There was no statistically significant relationship between the various patterns of chest radiographs identified in our study and the hematological parameters with test statistics (χ2=30.000, p=0.22) (Table 6).
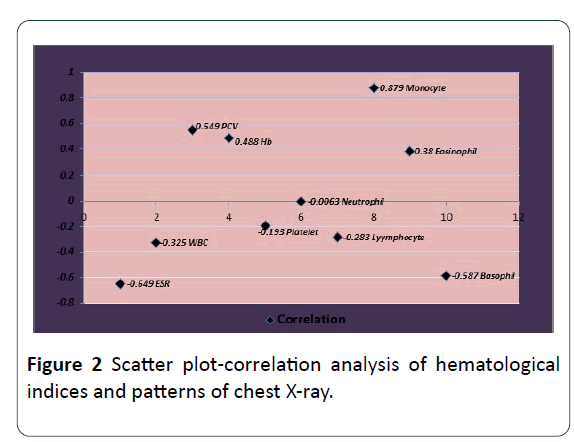
Figure 2 : Scatter plot-correlation analysis of hematological indices and patterns of chest X-ray.
| Age range |
Frequency n (%) |
χ2 |
p-value |
| ≤ 30 years |
75 (43.4) |
74.792 |
0 |
| 31-40 years |
68 (39.3) |
| 41-50 years |
18 (10.4) |
| >50 years |
12 (6.9) |
Table 3 Age distribution of participants.
| Weight Category |
Frequency n (%) |
χ2 |
p-value |
| Underweight |
67 (37) |
90.74 |
0 |
| Normal weight |
109 (60.2) |
|
|
| Overweight |
5 (2.8) |
|
|
Table 4 Body weight distribution of participants.
| |
Correlation |
P-value |
Remark |
| Hematological Indices |
Patterns of chest X-ray |
|
| ESR |
-0.649 |
0.16 |
N/S |
| WBC |
-0.325 |
0.53 |
N/S |
| PCV |
0.549 |
0.26 |
N/S |
| Hb |
0.488 |
0.33 |
N/S |
| Platelet |
-0.193 |
0.71 |
N/S |
| Neutrophil |
-0.0063 |
0.91 |
N/S |
| Lymphocyte |
-0.283 |
0.59 |
N/S |
| Monocyte |
0.879 |
0.02 |
Sig |
| Eosinophil |
0.38 |
0.46 |
N/S |
| Basophil |
-0.587 |
0.22 |
N/S |
Table 5 Correlation analysis of hematological indices and patterns of chest X-ray.
| |
Patterns of chest X-ray |
| Hematological Indices |
X2 |
Df |
p-value |
Remark |
| |
30 |
25 |
0.22 |
N/S |
DF=Degree of Freedom, χ2=Chi Square, N/S=No significant
Table 6 Chi Square showing relationship between hematological indices and patterns of chest X-ray.
Discussion
Consolidation was the most common chest radiographic patterns of tuberculosis in this study followed by cavitation and the least was pleural effusion. This finding is in agreement with the studies conducted by Akhigbe et al. [6] Wilcke et al. [19] and Nagwa [20]. On the contrary, Ahidjo et al. [21] and Marchie et al. [22], reported different findings from our report. Only three patients presented with normal chest radiograph in our study, this is contrary to the report by Ahidjo et al. [21] where he reported 28% normal chest radiograph. This variation may be attributed to immuno-supression in the subjects studied. In our result only six patterns of TB manifestation were identified (consolidation, cavitation, lymphadenopathy, pleural effusion, Fibrosis and normal). Additional patterns such as hilar and mediastinal adenopathy, milliary pattern and pleural thickening were identified by other researchers. This discrepancy in our findings may be ascribed to the nature of the subjects studied, the geographical variations and the imaging modality used for this study when compared to findings of other studies done with computed tomography and other imaging modalities.
In this study, 98% and 100% of the subjects had anemia and elevated ESR respectively. The platelet counts of the TB subjects in this study were within normal range. Previous studies revealed low percentage of anemia among TB patients when compared to the high percentage of anemia noted in this study. A similar study conducted in sub-Saharan Africa reported 88% in HIV positive and 77% in HIV negative TB subjects [23]. Although the last previous study reported slightly high prevalence of anemia, our study reported 97%.The differences in our findings could be attributed to HIV status, sample size and geographical variations. Our result also revealed that the PCV value was low among TB patients and this is consistent with the findings in other studies conducted by Awodu et al. [24], Agarwal et al. [25] and Nwankwo et al. [26] whereas Akpan et al. [16] and Saria et al. [27] reported higher PCV values in their findings. Akpan et al. [28] attributed the result of their study to the local diet in Calabar which consist of leafy vegetables and sea food such as fish, snails, crayfish and periwinkle when compared to staple diets which consist of little or no vegetables and seafood, found in places like Kano and Benin towns in Nigeria. The overall discrepancies between our findings and previous studies as regards the prevalence of anemia among TB patients could be ascribed to their dieting patterns which vary geographically. In this study, we discovered that there was no statistically significant correlation between the hematological parameters with exception of monocytes and the various patterns of chest radiographs identified. No statistically significant relationship between the variables studied was also noted in this study.
Conclusion
Pulmonary tuberculosis is a disease affecting predominantly males of the young productive age. Greater numbers of the subjects studied were males with a mean age of 33 yrs. This represents the economic power house of the population. Consolidation was the most prevalent chest radiographic finding in pulmonary tuberculosis subjects in this study. There was no statistically significant correlation between the various chest radiographic patterns and ESR, WBC, PCV, Hb, platelets, lymphocytes, eosinophil’s and basophils, but there was a statistically significant correlation between the various chest radiographic patterns and monocytes in our study. There is no statistically significant relationship between chest radiographic patterns and the hematological parameters evaluated in this study.
24084
References
- Sauders E (2007) Robbins basic pathology. (8th Edn.). Cambridge Press, London, pp: 516-520.
- Iseman MD (2000) A clinician’s guide to tuberculosis. Philadephia: Lippincot, Williams and Wilkins.
- World Health Organization (2011) Global tuberculosis control: Epidermiology, Strategy, Financing. Geneva.
- Akhigbe RO, Ugwu AC, Ogolodom MP, Maduka BU, Jayeoba BI (2019) Abnormal chest radiographic patterns in patients with pulmonary tuberculosis in Lagos State Nigeria: A single center study. Int J Med Health Res 5: 36-40.
- Akpan PA, Okafor IM, Anakebe S (2017) Altered protein and iron levels of patients with active tuberculosis in a Nigerian reference health facility. Afr J Clin Exp Microbiol 18: 174-178.
- Cohen R, Muzaffar S, Capellan J, Azar H, Chinikamwala M (1996) The validity of classic symptoms and chest radiographic configuration in predicting pulmonary tuberculosis. Chest 109: 420-423.
- Kisembo HN, Boon SD, Davis JL, Okello R, Worodria W, et al. (2012) Chest radiographic findings of pulmonary tuberculosis in severely immunocomprised patients with the immunodeficiency virus. Br J Radiol 85: e130-e139.
- Andrew NC (2004) Anaemia of inflammation: The cystokine-hepcidinlink. Th J Clin Invest 113: 1251-1253.
- Damburam A, Garbatic MA, Yusuph H (2012) Serum proteins in Health and in patients with Pulmonary TB in Nigeria. J Infect Dis Immun 4: 16-19.
- Morris CD, Bird AR, Nell H (1989) The hematological and Biochemical changes in severe pulmonary tuberculosis. Q J Med 73: 1151-1159.
- Okafor IM, Eyo AO, Okon EA, Akpan PA (2013) Some Hematological Parameters of Tuberculosis infected Nigerians: A study in Calabar, Nigeria. Global J Pure App Sci 19: 95-100
- Singh KJ, Ahluwalia G, Sharma SK, Saxena R, Chaudhary VP, et al. (2012). Significance of hematological manifestations in patients with tuberculosis. J Assoc Physicians India 49: 788-794.
- Sobero R, Peabody J (2006) Tuberculosis control in Bolivia, Chile, Colombia and Peru: why does incidence vary so much between neighbors? Int J Lung Tuberc Dis 10: 1292-1295.
- Akpan PA, Akpotuzor JO, Akwiwu EC (2012) Some hematological parameters of tuberculosis (TB) infected Africans: The Nigerian Perspective. J Natural Sci Res 2: 50-56.
- Devi U, Mohan RC, Srivastava VK, Rath PK, Das BS (2003) Effect of iron supplementation on mild to moderate anaemia in pulmonary tuberculosis. Br J Nutr 90: 541-550.
- Yamane Y (1967) Statistics: An introductory Analysis (2nd edn.). Harper and Row, New York. pp: 23-34.
- Wilcke JTR, Askgaard DS, Jensen NB, Dossing M (1998) Radiographic spectrum of adult Pulmonary Tuberculosis in a developed country. Respir Med 92: 493-497.
- Nagwa A (1997) Radiological and clinical pattern of pulmonary tuberculosis in selected TB clinics in Khartoum, University of Khartoun.
- Ahidjo A, Yusuph H, Tahir A (2005) Radiographic features of pulmonary tuberculosis among hiv patients in Maiduguri. Niger Ann Afr Med 4: 7-9.
- Marchie TT, Akhigbe OT (2010) Comparing the level of CD4 T lymphocytes, to pulmonary features of tuberculosis in HIV patients in a local hospital. Niger J Clin Prac 13: 254-259.
- VanCrevel R, Ottenhoff THM, Van der Meer JWM (2002) Innate immunity to Mycobacterium tuberculosis. Clin Microbiol Rev 15: 294-309.
- Awodu OA, Ajayi IO, Famodu AA (2007) Hematological variables in Nigeria pulmonary tuberculosis patients undergoing therapy. Clin Hemorheol Microcirc 36: 267-275.
- Agarwal R, Malhotra P, Awasthi A, Kakkar N, Gupta D (2005) Tuberculous dilated cardiomyopathy: an under-recognized entity. BioMed Central Infect Dis 5: 29.
- Nwankwo EOK, Kwaru A, Ofulu A, Babashani M (2005) Hematological changes in tuberculosis in Kano, Nigeria. J Med Laboratory Sci 14: 35-39.
- Saria T, Aminur R, Hoque FMA (2012) Patient’s knowledge and attitude towards tuberculosis in an urban setting. Pulmonary Med 2012: 1-5.
- Akpan PA, Akpotizor JO, Akwiwu EC (2012) Some hematological parameters of tuberculosis (TB) infected Africans: The Nigerian perspective. J Natural Sci Res 2: 50-56.

