Keywords
Food service, hospital, evaluation, personnel, HACCP
Introduction
Hospitals seek to be efficient and competitive in the fields of quality care and cost management, aiming in the highest performance. This specific trend of hospitals is due to reasons like organisation complexity, increasing specialization, competition and the importance of patient safety. [1] Several researchers have studied the Total Quality Management (TQM) in relation to health. In a study involving 31 managers from 31 hospitals in northern Louisiana, found that the problems associated with implementing TQM, included the involvement and commitment of the management, the involvement of employees and the inability to connect to the patients’ satisfaction . [2] Also, a survey conducted in 67 hospitals in Korea showed that the most important factors relating to the application of TQM, is the adoption of Information Technology (IT) systems and the use of scientific skills. [1]
In a study contacted at seven hospitals of Missouri USA it was discovered that the clinical dietician and the personnel involved in the catering services, have different perspectives with regard to the TQM implementation. [3] It seems that education, cooperation and communication are essential elements for the personnel working in the food service department of the hospitals.
The systems of production and distribution of meals can have a significant impact on the food intake of hospital patients who are likely to develop malnutrition. [4,5] A survey to compare the central distribution system (plated system) to the satellite distribution system (bulk trolley system) found that with the central distribution system there was a larger quantity of unconsumed food compared to the satellite system. [6] In another study at Hammersmith Hospital in London 3 types of systems of meal distribution were investigated. [7] The systems were a central distribution system as a reference system, a system of satellite distribution and a system similar to the previous one with the exception that patients could have a free choice. The results showed a significant increase in energy and the amount of protein consumed by the two satellite systems of distribution compared with that of central distribution, which only exhibited higher rates in food waste. [7]
In hospitals, the consequences of food borne infections can range from annoying to life-threatening for a patient, since they can lead up to death in vulnerable groups. [8-10] These incidents could be avoided simply by proper implementation of Hazard Analysis Critical Control Points (HACCP). Employees who handle food may be responsible for food borne infections, as well as factors related to the amount of people and their training in the kitchen or the lack of support from managers. [11-14] A study conducted at the Necker-Enfants Malades Hospital in Paris, confirmed that to ensure the quality and safety of the meals is necessary to control the time and temperatures at each stage. [15] In the U.S., a survey conducted on 865 long-term care facilities, revealed that only 3 follow state recommendations for the prevention of Listeria monocytogenes, while 9% reported that they offer soft cheese from unpasteurised milk. [16] However, cases of salmonellosis in hospitals due to harmful food have been recorded in Greece. Specifically in July 2005 at the University Hospital of Heraklion incidents were recorded due to Salmonella enterica serovar enteritidis. [17] The Salmonella enterica was detected in patients, employees (including 2 asymptomatic employees in food services) and processed cheese that was in the freezer.
The aim of the present study was the evaluation of food safety management systems implementation, as well as the general evaluation of the total quality management systems in Greek hospitals. For this purpose 11 hospitals of Attica were selected to participate in the study and the sample came from the personnel of the nutrition department.
Methods
The questionnaires for the hospital staff were specific and involved information about the hospital itself. Those questionnaires were flagged with the job description of each employee, both for identification reasons and in order to find out if there are different attitudes in shaping the opinion about this hospital. The questionnaires were targeted for dietitians, public health officers, food technologists, as well as the head-chef or the chef in charge of the morning shift. It consists of 26 questions, with Yes/No answers or with a 5 grade Likert scale. Most questions concerned the quality of services and food safety standards. In total, thirty employees in the field of hospital nutrition participated through personal interviews with the assistance of undergraduate students of Harokopio University and Athens Technological Educational Institute. In the appendix the questionnaire for the interview is presented.Prior the interviews the general manager was contacted in order to acquire approval for this research. The interviews were performed after the receipt of the signed letter of approval by the general manager. The personnel was orally inquired if it consents for the interview.
Overall, for this purpose eleven hospitals of Attica were selected to participate in the study (Agios Savvas, Aretaio, Sismanoglio, Janio, Metaxa, Asklipieio Voulas, Laiko, Erythros Stavros, A. Siggros, G. Genimmatas, Elpis). The sample came from the high rank personnel of the nutrition department (dietician, head-chef, food technologist) and the public health officer of the hospital. The study was performed during the period from September 2009 until April 2010. The anonymity of the volunteers was ensured through coding of the questionnaires. The descriptive statistics were performed with the software PASW 18.0 for Windows (SPSS Inc. 2009).
Results
The participation per hospital in questionnaires reaches 6.7% for Aretaieio, 13.3% for Sismanoglio, 23.3% for Janio, 30% for Metaxa, 40% for Asklipiio Voulas, 50% for Laiko, 56.7% for Erythros Stavros, 66.7% for Agios Savas, 73.3% for A. Syggros, 90% for G. Genimmatas, and 100% for Elpis. The 44.8% of the hospitals participating in this study implement the central distribution system, while 55.2% the satellite system. The HACCP system is implemented only in the 30% of the participating hospitals (question 20).
A very small percentage (10%) uses external catering services in an everyday basis, while 63.3% of the participants stated that they never use external catering. The distribution of the trays to the patients is done in a 33.3% with open trolleys and in 66.7% with closed ones. A percentage of 63.6% of the personnel declared that the closed trolleys are not isothermal.
As seen in Table 1, the temperature of the cold plates is considered good in a percentage of 44.8%; the temperature of the hot plates is considered very good in a percentage of 43.3%, while 40% of the personnel think that the way of food preparation very much fulfils the prerequisites for the hygiene standards.

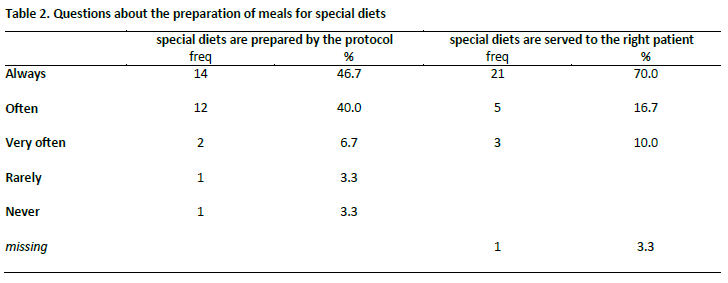
As seen in Table 2, 46.7% of the participants think that the proper production according to the guidelines in a special diet is always controlled, while in the question if there is control of the serving to the right patient, 72.4% think that there is always control and 62.1% think that no one from the food department deals with matters other than food.
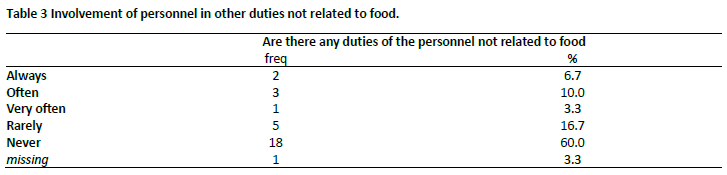
As seen in Table 3, 6.7% of the personnel have also other than food related duties. In a percentage of 90% there is support on informatics, while in a percentage of 67.9% it serves for logistics and in 65.5% for the documentation of the nutritional schemes. The food-borne allergies go undocumented in 82.1% of the cases and also food sampling carried out in 65.5% of the cases. Finally in a percentage of only 56.7% there are records kept for the food storage in low temperatures.
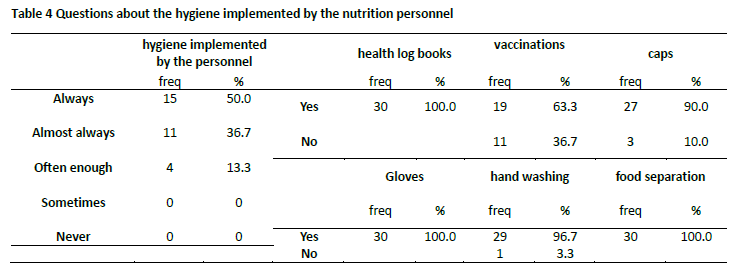
As seen in Table 4, the hygiene regulations are implemented by 50% of the personnel, health is checked with individual health log books, 63.3% of the personnel have been vaccinated, while almost everyone uses proper hygiene like caps and gloves, meticulous hand washing and separation of food.
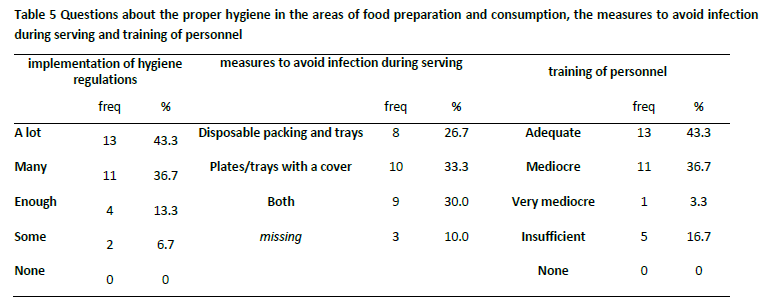
As seen in Table 5, in a percentage 43.3% a lot of the hygiene regulations are implemented. In the framework for implementation of measures for avoiding transmittable infections, 39.6% use disposable packing and trays, while 37% use plates and trays with a cover. A rate of 43.3% thinks that the training in quality issues is adequate, while 36.7% thinks it is mediocre.
According to a percentage of 80% there is always quality control during the receiving of the raw materials and in a percentage of 63.3% the suppliers of food products are accredited for food safety management. Regarding the presence of employees that feel unwell, in 88% of the cases the diseased employee is relieved of his duties until he/she is better.
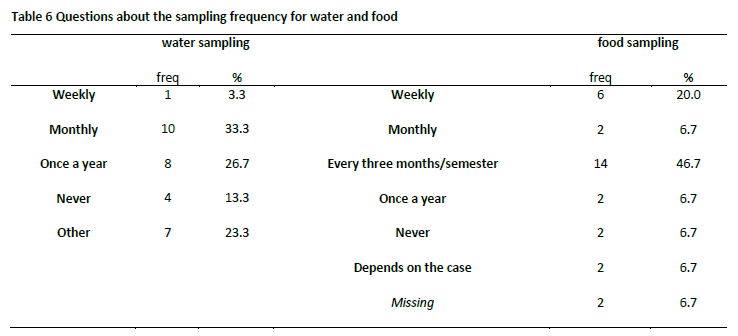
As seen in Table 6, in a 33.3% there is sampling of water once in a month, followed by a rate of 26.7% that samples water once in a year. Sampling of food is carried out every three months or semester in a 46.6%, while the sampling for raw materials is 86.7% and for the end products is 60%. Within 74.1% of the participating hospitals there is a recording system for food borne infections.
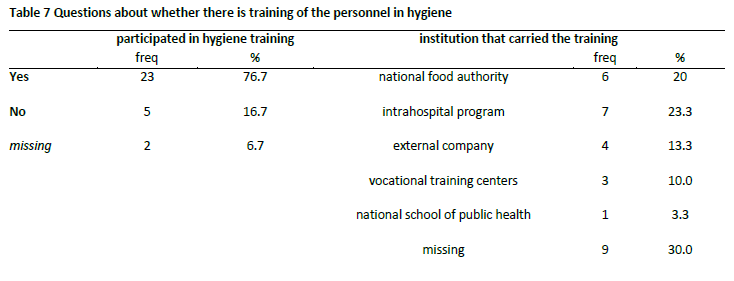
As seen in Table 7, 82.1% of the participants states that there have been efforts of training in matters of hygiene mostly from the EFET, the national food control authority, by a percentage of 27.3%. A percentage of 83.3% of the personnel states that there is a guide of good hygiene practices available.
Discussion
The personnel of the Nutrition Department in the participating hospitals were often sceptic during the interview about the lack of commitment from the top management in relation to the implementation of HACCP, and the insufficient personnel training on proper hygiene practices and special diets. The majority of the hospital personnel had a positive response to our survey. However, in some hospitals not all the preset managerial positions were available. The serving system implemented in the majority of the participating hospitals is the satellite one, which merits more disadvantages than advantages from the central serving system. Several researchers have related patient satisfaction with the serving system. In a survey carried out in a large university hospital of United Kingdom, found out that the patients were generally more satisfied with the steamplicity system (a cook-chill system). [18] Another survey in England concluded that patient satisfaction is reinforced by the possibility to choose at the point of serving, which is only feasible with the satellite serving system (bulk trolley system). Temperature control and food structure seems to be better in the satellite system. [19] Patient satisfaction, however, seems to be enhanced by the serving of intermediate snacks, at times other than those of the standard meals. [20]
Regarding the meal serving time and temperature control, the requirements are generally fulfilled; nevertheless it is important to mention that most of the hospitals do not have isothermal distribution trolleys. Specifically, the distribution of trays to patients is carried mostly with closed trolleys, which are not isothermal. This is of particular importance since the temperature is just as critical as taste and appearance, preventing or encouraging the patients to consume their meal, along with the provision of adequate food variety or a meal choice. [21,22] Sampling of food or meals is carried usually every trimester.
With regard to special diets, only half of the personnel believe that there is always a control for the correct preparation of a special diet, based on specific standards. Regarding serving the right meal to the right patient (avoiding serving errors), most of the personnel believes that it is always controlled. The two thirds of the staff in the nutritional department are not involved in tasks not related to food that may affect the safety of the patients. Food allergies are usually not recorded and sampling of foods or meals is not documented. However, the temperatures of refrigerators for food storage are recorded.
There have been efforts for training by the national food control authority in one out of three the hospitals. According to the results of our investigation, it appears that hygiene training - at least by official authorities - lacks in the non-medical personnel of the Greek hospitals. The importance of training for the personnel upon the implementation of good hygiene practices, as well as a general psychological approach to the patients, is highlighted.
There is a doubtful perception that hygiene regulations are applied by the food service personnel. Disposable cutlery is not often used. Dishes and trays are not covered with a lid in every hospital. An interesting finding is that the HACCP system is implemented only to one out of three hospitals in the study. One of the most plausible reasons for that is that there are no specific standards for Greek hospitals. Regardless the requirement for HACCP implementation by the legislation, national authorities did not enforce the law. Neither the hospital administration was keen to apply food safety standards in the same way that standards for the intensive care unit or the surgery ward are implemented.
The method of this study has certain limitations. The answers to the questions are subjective and cannot be verified with audits or sampling. The personnel of the food service department is not used at taking part in such kind of surveys. The number of persons that consented to the interview is part of the actual food service personnel that is working at the selected hospitals. However the proposed questionnaire has simple questions that require straightforward answers and can be used for further research.
Conclusion
To summarize all the above, the lack of commitment by the management, the poor prerequisite programs, the inadequate staff training, the wrong allocation of working tasks, the poor documentations and record keeping related to food safety, the lack of effective evaluation of suppliers, and of course the fact that medical services are always first priority, while food services are last, result to the overall negative profile of hospital food in Greece. In very few questionnaires there were proposals for improvement by the staff, which focused on human resources, infrastructure to implement a HACCP, and the lack of motivation for the personnel to attend training programs.
The results of this study show that the personnel in Greek hospitals have the availability and potential to offer better food services to hospitalized patients. Finally, the results indicate the importance of total quality systems that could be applied in hospital food service, together with medical or nursing services.
Measurement of the opinion of the personnel about the provided food services within a hospital can further lead to continuous improvement of the hospital nutrition.
2737
References
- Lee TY, Yeh ML, Chen HH, Lien GH. The skill mix practice model for nursing: Measuring outcome. J Adv Nurs 2004; 51(4): 406-413.
- Lin B, Clousing J. Total quality management in health care: a survey of current practices. The TQM Magazine 1995; 6: 69-79.
- Chong Y, Unklesbay N, Dowdy R. Clinical Nutrition and Foodservice Personnel in Teaching Hospitals have Different Perceptions of Total Quality Management Performance. J Am Diet Assoc 2000; 100(9): 1044-1049.
- Mcwhirter JP, Pennington CR. Incidence and recognition of malnutrition in hospital. Br Med J 1994; 308: 945-948.
- Mowe M, Bosaeus I, Rasmussen HH, Kondrup J, Unosson M, Irtun O. Nutritional routines and attitudes among doctors and nurses in Scandinavia: a questionnaire based survey. Clin Nutr 2006; 25(3): 524-532.
- Wilson A, Evans S, Frost G. A comparison of the amount of food served and consumed according to the meal service system. J Hum Nutr Diet 2000; 13(4): 271-275.
- Wilson A, Evans S, Frost G, and Dore C. The effect of changes in meal service systems on macronutrient intake in acute hospitalized patients. Food Serv Technol 2001; 1: 121-122.
- Joseph CA, Palmer SR. Outbreaks of Salmonella infection in hospitals in England and Wales 1978-1987. Br Med J 1989; 298: 1161-1164.
- Wall PG, Ryan MJ, Ward LR, Rowe B. Outbreaks of salmonellosis in hospitals in England and Wales: 1992-1994. J Hosp Infect 1996; 33(3): 181-190.
- Meakins SM, Adak GK, Lopman BA, O’Brien SJ. General outbreaks of infectious intestinal disease (IID) in hospitals, England and Wales, 1992-2000. J Hosp Infect 2003; 53(1): 1-5.
- Lund B, O’Brien S. Microbiological safety of food in hospitals and other healthcare settings. J Hosp Infect 2009; 73(2), 109-120. 12.Mair Thomas, Norman D. Noah, G.E. Male, M.F. Stringer, Margaret Kendall, R.J. Gilbert, et al. PhillipsHospital outbreak of Clostridium perfringens food-poisoning. Lancet 1977; 309(8020): 1046-1048.
- Pollock AM, Whitty PM. Crisis in our hospital kitchens: ancillary staffing levels during an outbreak of food poisoning in a long stay hospital. Br Med J 1990; 300(6721): 383-385.
- Pennington TH. When food kills. Eds., Oxford University Press, Oxford,2003.
- Réglier-Poupet H, Parain C, Beauvais R, Descamps P, Gillet H, Le Peron JY, et al. Evaluation of the quality of hospital food from the kitchen to the patient. J Hosp Infect 2005; 59(2): 131-137.
- Nelson, Jennifer M. Bednarczyk, Robert; Nadle, Joelle Clogher, Paula; Gillespie, Jennifer; Daniels, Allison, et al. Foodnet survey of food use and practices in long-term care facilities. J Food Prot 2008; 71(2): 365-372.
- Maraki S, Ladomenou F, Samonis G, Galanakis E. Long-term trends in the epidemiology and resistance of childhood bacterial enteropathogens in Crete. Eur J Clin Microbiol Infect Dis 2012; 31: 1889–1894
- Edwards JSA, Hartwell HJ. Hospital food service: a comparative analysis of systems and introducing the ‘Steamplicity’ concept. J Hum Nutr Diet 2006; 19(6): 421-430.
- Hartwell HJ, Edwards J, Beavis J. Plate versus bulk trolley food service in a hospital: comparison of patients’ satisfaction. Nutr 2007; 23(3): 211-218.
- White M, Wilcox J, Watson R, Rogany A, Meehan L. Introduction of a patient-centred snack delivery system in a children’s hospital increases patient satisfaction and decreases foodservice costs. J Food Serv 2008; 19(3): 194-199.
- Watters C, Sorensen J, Fiala A, Wismer W. Exploring patient satisfaction with foodservice through focus groups and meal rounds. J Am Diet Assoc 2003; 103(10): 1347-1349.
- Porter J, Cant R. Exploring hospital patients’ satisfaction with cook-chill foodservice systems: a preliminary study using a validated questionnaire. J Food Serv 2009; 20(2): 81-89.

