Key words
Nursing care rationing, missed care, focus group
Introduction
Prioritization or rationing of health services by different approaches or at different levels, seems inevitable in all health care systems because of the limited resources and economic constraints. From the nursing point of view, when there is scarcity of resources, nurses are forced to limit their attention across their patients, using their clinical judgment to prioritise assessments and interventions [1]. Therefore rationing in nursing care can be defined as “withholding or failure to carry out necessary nursing tasks due to inadequate time or staff, thereby increasing the risk of negative patient outcomes and contributing to reduced quality of care” [2] (p.228). The issue of rationing is relatively new in the nursing agenda and it has been developed within the patient safety movement and quality of care. Research on nursing care rationing has followed several methodological approaches. Most studies present similarities as to the elements of nursing care being missed and these include: patient teaching and discharge planning, ambulation, hygiene, feeding, surveillance, and care documentation [3-7]. It is also apparent from the empirical data that nurses prioritise according to medical needs and medical urgency [8-12]. Other authors have evaluated the quality of nursing care on the basis of nursing care deficiencies and found that quality care ratings by nurses and patient safety were significantly related to the rates of unfinished care [6,13,14]. A different approach was followed by researchers who have examined the ethical and moral perspective of rationing highlighting the principles of justice and equality of care and value considerations [15-17]. Focus group approach in rationing research has been used for the development of a questionnaire [4] to understand how nurses delegate tasks [5,18], in comparative studies in the USA and Canada [19], but there is little or no explanation on how the researchers used the methodology to approach the subject in a group setting, and collect the data. What makes rationing of nursing care a “sensitive issue” is that although most nurses are fully aware that care is missed, they do not openly acknowledge or discuss it. Nurses are usually reluctant to report any omissions in care and are not always willing to report cases of uncompleted tasks particularly if perceived as a deficiency in their practice or abilities [4,20]. There is also evidence that not meeting patients’ needs can be very frustrating for individual nurses and rationing may add an ethical burden on them causing value conflict and moral distress [4,11]. According to Kalisch [21] the open acknowledgement of care omitted can lead to feelings of guilt, powerlessness and fear; such emotional response is validated by the reaction of nurses when the concept of rationing is introduced to them via focus groups. Nurses react to rationing with emotions like anger, sadness and frustration, describing low self esteem because they are not providing quality care [21]. Focus-group methodologists [22] argue that the involvement in a group interview can provide security for participants and thus encourage interaction and self disclosure especially when these experiences are familiar and shared by the other group members. These issues have lead to the decision to use a method that would provide a better insight into the nurses’ understanding and interpretations of their experiences and portray the reality of what is happening at bedside nursing. Therefore, the aim of this article was to discuss the methodological issues of the focus group approach when used in the rationing research.
Methods
The focus group discussion was used to explore participants’ individual perceptions of rationing. Focus groups were used as research method in social sciences since 1940’s and later became popular in health care research and incorporated into nursing research as a tool for understanding different phenomena in clinical nursing and education. The focus group approach can provide major insights into attitudes, beliefs and opinions [23] and it’s particularly useful in reflecting the social realities of a culture group, through the language and concepts which structure participants’ experiences. Focus groups were used in very few research projects relating to rationing and the reports focused mainly on the results and not the methodological issues [4,5,19].
The benefit of using this methodological approach is that when it is used in tandem with other strategies, in our case a survey, it may provide further insight into factors associated with rationing and make a significant contribution throughout the research project. The level of rationing found in surveys [1] do not provide adequate information of the underlying processes of rationing. In addition, the principal advantage using focus groups is the opportunity to capitalize on group dynamics and the ability to use participant interaction to gain in-depth data that would not be obtained through individual interviews or other forms of group interviews [24]. It was also expected that when participants hear and see that others have similar experiences, it would legitimate their own feelings and provide an atmosphere for openness and candor [25].
Participants
A total of 17 nurses recruited and participated in the focus groups (group A n=7, group B n=4, group C n=6). The size was based on the ease of group management, to encourage adequate participation by all members. In addition, there is support that group dynamics change when participants want but are not able to describe their experiences when the group size is too big [26].
Purposive sampling was employed to ensure a range of nursing experiences with rationing of nursing care. The groups were homogenous in terms of education and job-level but differed in terms of the number of years in nursing to elicit a range of views related to their experience. Most of the participants of groups A and B came from different wards and did not know each other before the focus groups; on the other hand, the majority of the participants in group C worked in the same ward. In the rationing literature, some authors used a mixed group of registered nurses and nurse assistants [4,27] or registered nurses [5]. The participants in this study worked in surgical and medical wards, nephrology, cardiology, intensive care, oncology and urology units of three different hospitals providing the amount of heterogeneity needed to produce rich information [23]. Although rationing of nursing care is presented mostly as an organizational problem and the views of nurse managers or doctors can enrich the understanding of rationing, it was decided to form homogenous groups at the job level to facilitate comparisons between the nurse-managers-doctors sub-groups (at a later stage) and increase the external validity of comparisons between the subgroups [28]. In addition, maintaining the homogeneity of the groups reduced the possibility that some members, e.g. nurse managers, could dominate the conversation [29] and inhibit discussion because of status distinctions between the participants [28]. In such case, the security provided by the group that would allow the members to express their ideas without fear could be lost.
There are no general rules as to the optimal number of focus groups [28], and there is little consensus as to what is the most appropriate sample size. Other studies using focus groups to explore the issue of rationing, used four groups and 27 participants [4,5]. Three focus groups were conducted for and the decision was based on the homogeneity of the participants [26], since they all were registered bed-side nurses, working in general hospital wards. Another principle that guided the decision of conducting three focus groups was the notion of saturation, a useful concept as interviews can end when no information is being collected [23].
Development of the interview guide
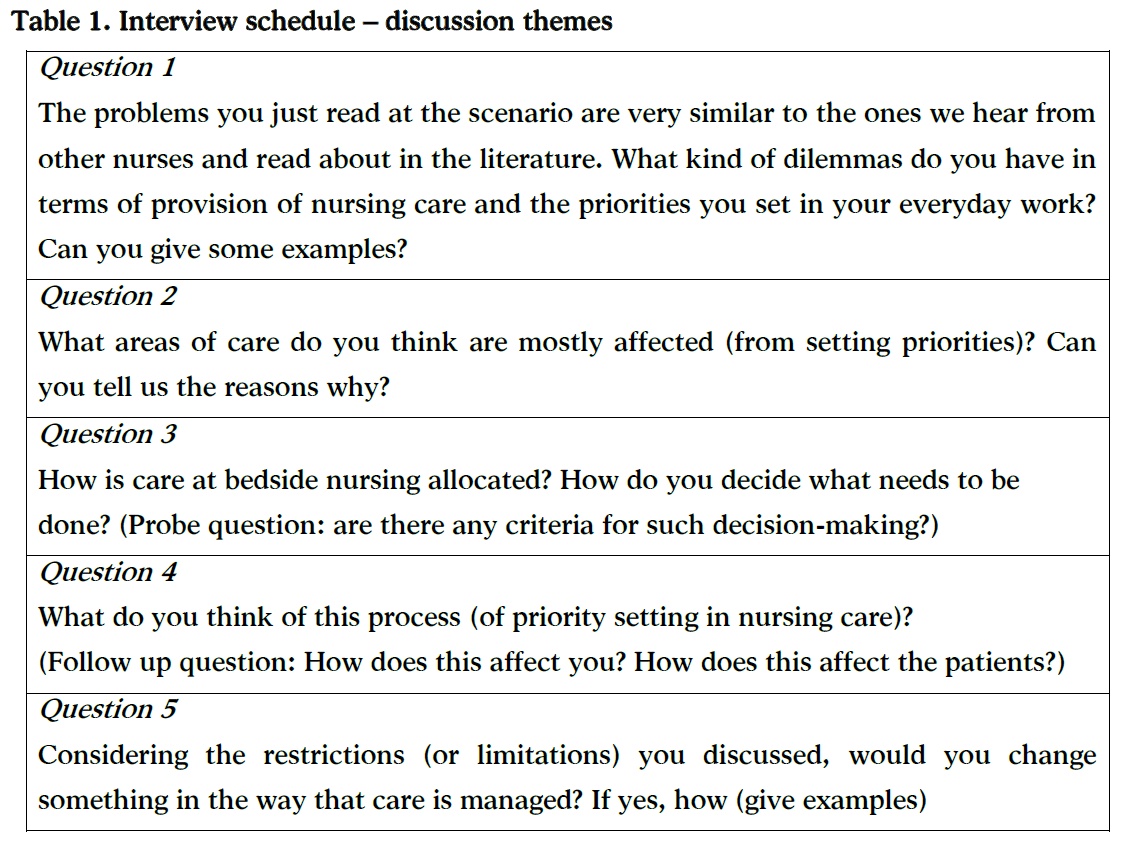
Prior research on care rationing found that nurses may experience feelings of guilt when they omit nursing care, something that it is not easily discussed [4]. It is also found that in nursing research, participants are eager to talk once the topic is mentioned, arguing that they see the group as a form of catharsis or getting a message to someone who might be able to influence the situation [24]. Thus it was decided avoid asking direct questions from the beginning, but instead, to build on the participants’ responses to a given scenario describing a typical day on a busy ward with shortage of staff. The scenario was developed by the principal investigator and discussed with the research team until a consensus was reached. A similar approach was followed in the area of rationing that used three case studies in the form of vignettes aiming to determine nurses’ choices in cutting care hours from specific care dimensions and specific categories of patients [30].
The participants were then asked to think back when they had a similar experience from their daily routine at their ward (the interview schedule –Table 1). They were encouraged to elaborate on the nursing care tasks they would omit, the procedures they would give priority to and explain the reasons that guided their decision. Emphasis was given on the interaction between the group members as a useful way for encouraging discussion and exchange of experiences.
Setting and data collection
The focus groups were conducted by one researcher (PA) who acted as a moderator. The interviews lasted between 60 to 70 minutes and took place at settings convenient to the participants. In particular, two groups were held at the hospital site and the third group at the school of nursing. Data collection was performed between June and September 2011. Each group session was opened with a short introduction asking the participants to introduce themselves. The participants were asked to write to a piece of paper a pseudo name. The paper was kept in front of them throughout the discussion and all participants were asked to refer to each other based on their new names in order to ensure confidentiality. The participants were also asked to say loud their new name before talking in order to record the identity of the speaker during the transcription. The scenarios were distributed at the beginning with a few minutes for the participants to read it before continuing with the questions and discussion. Open questions were used to avoid direction and allow the participants the opportunity to highlight aspects which seemed to be more important to them. The discussion was audio taped and the non-verbal responses and interactions among the group members were observed and written down by an independent observer. At the end of each session, the participants were asked to fill in a questionnaire with demographic information.
The role of the moderator
The role of the moderator is to facilitate the discussion in a non-intrusive way so that the participants are enabled to express their opinions as freely as possible [24].
The moderator was not known to the participants and was not related to nursing in order to reduce social desirability bias and “contamination of the data” [24] aimed to be seen as impartial and objective with no vested interest in the participants’ responses. The role of the moderator was explained and the ground rules were set at the beginning emphasizing confidentiality and respect of opinions. Thus it was possible to create a non-threatening supportive climate that encouraged all members to share views, and facilitate interaction. The moderator encouraged further discussion with probing questions and comments, seeking for clarification, noting non-verbal responses, and summarising without interfering with the dialogue [23]. Ending questions were critical to the study and helped to clarify the main points of participants; a short verbal summary at the conclusion of the discussion allowed verification of the issues raised.
Recording and Analysis of data
Data analysis from focus groups, both at the individual and at group level, is not a well developed methodological issue, and although several guidelines have been suggested there is not a widely accepted process. The little evidence on the analysis process is also reflected in the rationing literature using focus groups [4,5,19]. The data of the current study was analysed based on content analysis (CA) as the study did not aim to develop a theoretical framework. In addition, CA provides a range of systematic, rule-guided techniques to analyse and interpret informational contents of textual data [31,32]. The focus group interviews were tape-recorded and transcribed by the moderator and transcription following certain rules [33]. An immediate debriefing and discussion at the end of the focus groups, among the moderator, the observer and other members of the research team facilitated the analysis process.
The analysis begun as soon as the transcript of the first focus group was completed to provide the opportunity to the moderator to identify any issues that could be improved or modified in the subsequent interviews. An analysis protocol was agreed prior to analyzing the data so as to be carried out in a systematic way [26]. The transcript analysis was divided in three phases [33]: Immersion, reduction and interpretation in order to create new knowledge from raw unordered data. In particular, the transcripts were repeatedly read to achieve immersion. Data were read highlighting words or phrases that captured key thoughts or concepts and creating open codes. The coding was based on inductive analysis without predetermined categories and aimed to examine the latent content of the data i.e. investigate the inferred deeper meanings that could lead to the development of constructs. Concurrently, the researchers noted of emerging impressions, thoughts, and associations with existing literature that could inform further the analysis process. The data from the transcripts were enriched by field notes and notes from the observer, such as participants’ behaviour in order to gain a wider perspective of peoples’ accounts and stories about rationing. Codes were then sorted into sub-categories or themes based on how different codes were related. Similar sub-categories were clustered together into categories and given a definition together with their corresponding sub-categories, codes and extracts from the transcripts. The researchers then checked the emerging categories and their codes for relationships; concurrence; sequence and consequences in relation to the experiences of the participants as well as to the context e.g. group influences and reactions to the discussion. This was an iterative rather a linear process where researchers went back and forth between the data and the coding process to reexamine, discuss and ensure that data interpretation reflected the actual data.
The analysis did not involve any quantification of the data. The detailed results from the focus group will be published in a different article.
Group interaction
A key feature of focus groups is the group interaction among participants that stimulates discussion that might not otherwise emerge. There are some methods that aim to capture the richness of the emerging data by illustrating how participants may change or reinforce their views in the context of group dynamics. Such methods include conversation analysis [34,35]; use of classification categories [36], incorporation of group interaction data into the transcripts [37], and separate analysis of the group interaction data using the same method as for the group data [38]. However, some methods are not very well documented particularly their implementation stage; others illustrate their analysis techniques based on computerized methods which are not widely available thus making it uncertain how to implement such techniques manually and ensuring that group dynamics can be interpreted. In addition, certain approaches require the interviews to be transcribed in particular way e.g. inclusion of detailed accounts of nonverbal communication, recording periods of silences, noting voice pitch in relation to the other voices.
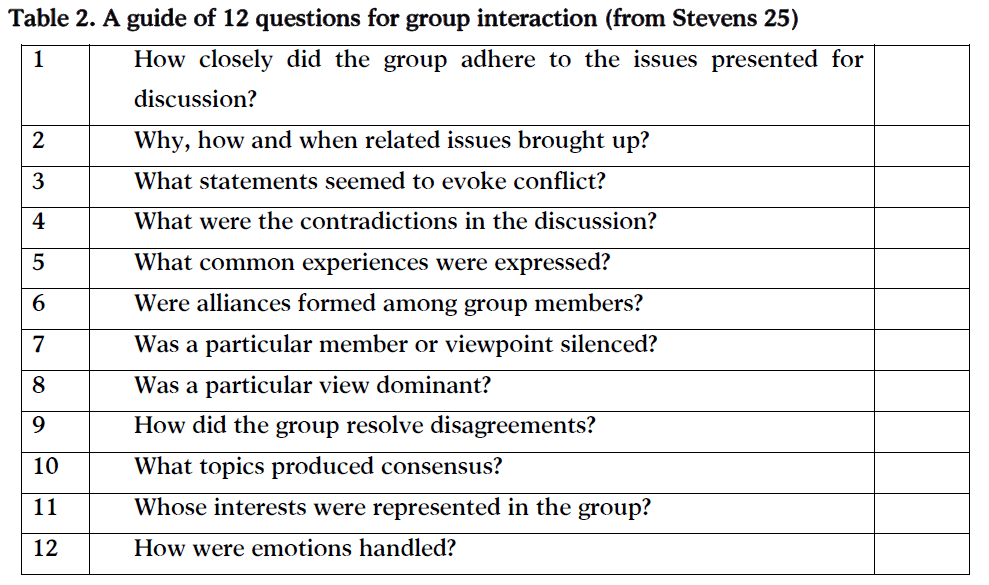
For the purpose of the current study based on the transcribed data and considering the manual coding of the data, group interactions were analysed based on a guide of twelve questions [25] (see table 2). The questions provide an explicit way of understanding how interactions build on one another and whether participants reach some degree of collective experience. The guide is based on Carey’s [39] position that the analysis needs to incorporate a description of the nature of the group interaction or dynamics. These techniques have been criticized for their descriptive contribution rather for a more in-depth analysis of the interaction nature of the data [34,38]. Thus, in some cases in the current study additional analysis techniques were used where feasible to enhance interpretation of group interactions. Reed et al. [29] suggested capturing the sequence of discussion; as topic evolves, ideas and opinions begin to shift or strengthened as individuals reflect on their experiences and listening to others. Extracts from the discussion are presented where debate is visible, when there is an introduction of new ideas, and views are modified, developed, and related back to experiences. The same authors also suggest comparing responses between groups especially if the questions asked differ due to the evolvement of the interview schedule. They highlight issues such as which questions evoked more discussion, the presence of dominant members and their influence on the rest of the group. In addition, Wilkinson [34] suggested examining peoples’ responses in the context of the previous discussion aiming to understand why the speaker said that particular thing, in that particular way, at that particular point in the interaction. The use of these techniques in this study depended on the complexity of the data as the techniques were presented and applied with computerized analysis programs.
Methodological rigour
Several steps were taken in order to ensure the quality of the results. First, the moderator’s involvement and style did not exert a high influence on the control of the process and content of the interview; rather the emphasis was placed on the facilitating interactions between participants [24]. The way the participants answered was carefully observed, clarification was asked on areas of ambiguity and at the end they were asked to verify the summary comments. Secondly, interaction was encouraged as this provides a high level of face validity [26] as participants’ views can be confirmed, reinforced or contradicted within the group discussion [24]. Thirdly, analysis of the data consisted of the four distinct critical qualities: it was done in a systematic way; used verifiable procedures via content analysis; done in a sequential manner; it was continuous thus giving the opportunity of reflection and it was verified by a second researcher [26].
Furthermore, the reliability of the data was implemented by having two researchers independently coding the transcripts and comparing the codes to assess agreement to the core concepts and themes. Internal consistency of coding was applied [40] by having the same researcher acting as moderator in all three focus groups and sharing the primary responsibility in the analysis. Throughout the coding process and analysis process there was continuous communication with the other team member to assess degree of agreement and differences in the coding.
The construct validity of the findings was assessed by comparing the main themes derived from the focus groups to the existing literature on rationing of nursing care, both qualitative and quantitative. In addition, Reed et al. [29] argue that validity refers to the degree to which a procedure reflects what it is supposed to reflect thus ‘focus groups reflect the process of developing a group perspective or position among a group of people’ (p. 770). Thus the whole process of the analysis aimed to show whether a group perspective has been elicited and the process through which individual perspectives were discussed and evolved amongst group members.
The focus methodology used for the exploration of nursing care rationing presents some limitations. Participants in the one of the four groups were drawn from the same ward and they had already have developed relationships, thus could have an impact on group dynamics. Another limitation is that the selection of groups was based on convenience: in groups A and B most of the participants did not know each other where in group C the majority of the nurses worked at the same ward. This differentiation was not based on any evidence – rather it was lead by pragmatic reasons of personnel being available.
Conclusion
As a collection strategy the focus group approach has given the opportunity to obtain rich data; the group dynamics and interaction enhanced data collection and the participants felt free to discuss issues that otherwise would remain hidden. This was facilitated by the homogeneity of the group that in this case worked better than heterogeneous ones. The discussion presented in this article has outlined the methodological underpinnings of the focus group approach in sensitive nursing issues that usually are not fully discussed in research reports. Since focus group approaches are becoming a popular tool in nursing research, a rigorous approach to methodology is necessary to ensure the integrity of research and develop the research knowledge.
3264
References
- Schubert M, Clarke SP, Glass TR, Schaffert-Witvliet B, De Geest S. Identifying thresholds for relationships between impacts of rationing of nursing care and nurse- and patient-reported outcomes in Swiss hospitals: A correlational study. Int J Nurs Stud 2009 7;46(7):884-893.
- Schubert M, Glass TR, Clarke SP, Aiken LH, Schaffert-Witvliet B, Sloane DM, et al. Rationing of nursing care and its relationship to patient outcomes: the Swiss extension of the International Hospital Outcomes Study. International Journal for Quality in Health Care 2008 August 01;20(4):227-237.
- Morin D, Leblanc N. Less money, less care: How nurses in long-term care allocate hours of needed care in a context of chronic shortage. Int J Nurs Pract 2005;11(5):214-220.
- Kalisch BJ. Missed nursing care: a qualitative study. J Nurs Care Qual 2006;21(4):306-313.
- Bittner NP, Gravlin G. Critical Thinking, Delegation, and Missed Care in Nursing Practice. J Nurs Adm 2009;39(3):142-146.
- Lucero RJ, Lake ET, Aiken LH. Variations in nursing care quality across hospitals. J Adv Nurs 2009;65(11):2299-2310.
- Gravlin G, Phoenix Bittner N. Nurses' and Nursing Assistants' Reports of Missed Care and Delegation. J Nurs Adm 2010;40(7/8):329-335.
- Gaudine A, LeFort SM, Lamb M, Thorne L. Clinical ethical conflicts of nurses and physicians. Nurs Ethics 2011;18(1):9.
- Halvorsen K, Førde R, Nortvedt P. Professional challenges of bedside rationing in intensive care. Nurs Ethics 2008;15(6):715-728.
- Halvorsen K, Forde R, Nortvedt P. Value choices and considerations when limiting intensive care treatment: a qualitative study. Acta Anaesthesiol Scand 2009;53(1):10-17.
- Nortvedt P, Pedersen R, Grothe K, Nordhaug M, Kirkevold M, Slettebo A, et al. Clinical Quarterly scientific, online publication by Department of Nursing A’, Technological Educational Institute of Athens Page | 196 Exploring sensitive nursing issues through focus group approaches prioritisations of healthcare for the aged--professional roles. J Med Ethics 2008;34(5):332-335.
- Slettebø Å, Kirkevold M, Andersen B, Pedersen R, Halvorsen K, Nordhaug M, et al. Clinical prioritizations and contextual constraints in nursing homes ? a qualitative study. Scand J Caring Sci 2010;24(3):533-540.
- Sochalski J. Is more better?: the relationship between nurse staffing and the quality of nursing care in hospitals. Med Care 2004;42(2):II-67-II-73.
- Rochefort CM, Clarke SP. Nurses’ work environments, care rationing, job outcomes, and quality of care on neonatal units. J Adv Nurs 2010;66(10):2213-2224.
- Nortvedt P, Hem MH, Skirbekk H. The ethics of care: Role obligations and moderate partiality in health care. Nurs Ethics 2011;18(2):192.
- Tønnessen S, Førde R, Nortvedt P. Fair Nursing Care When Resources Are Limited: The Role of Patients and Family Members in Norwegian Home-Based Services. Policy, Politics, & Nursing Practice 2009 November 01;10(4):276-284.
- Tønnessen S, Nortvedt P, Førde R. Rationing home-based nursing care: professional ethical implications. Nursing Ethics 2011 May 01;18(3):386-396.
- Kalisch BJ. Nurse and Nurse Assistant Perceptions of Missed Nursing Care: What Does It Tell Us About Teamwork? J Nurs Adm 2009;39(11):485-493.
- Bourgeault IL, Armstrong P, Armstrong H, Choiniere J, Lexchin J, Mykhalovskiy E, et al. Everyday experiences of implicit rationing: comparing the voices of nurses in California and British Columbia. Sociol Health Illn 2001;23(5):633-653.
- Attree M. Factors influencing nurses’ decisions to raise concerns about care quality. J Nurs Manag 2007;15(4):392-402.
- Kalisch BJ, Landstrom GL, Hinshaw AS. Missed nursing care: a concept analysis. J Adv Nurs 2009 07;65(7):1509-1517.
- Casey MA, Krueger R. An overview of focus group interviewing. Evidence-based practice manual: Research and outcome measures in health and human services 2004:61-69.
- McLafferty I. Focus group interviews as a data collecting strategy. J Adv Nurs 2004;48(2):187-194.
- Webb C, Kevern J. Focus groups as a research method: a critique of some aspects of their use in nursing research. J Adv Nurs 2001;33(6):798-805.
- Krueger RA, Casey MA. Focus groups: A practical guide for applied research. : Sage; 2009.
- Kalisch BJ, Landstrom G, Williams RA. Missed nursing care: errors of omission. Nurs Outlook 2009;57(1):3-9.
- Freeman T. ‘Best practice’in focus group research: making sense of different views. J Adv Nurs 2006;56(5):491-497.
- Reed J, Payton VR. Focus groups: issues of analysis and interpretation. J Adv Nurs 1997;26(4):765-771.
- Morin D, Leblanc N. Less money, less care: How nurses in long-term care allocate hours of needed care in a context of chronic shortage. Int J Nurs Pract 2005;11(5):214-220.
- Qualitative content analysis [28 paragraphs]. Forum Qualitative Sozialforschung/Forum: Qualitative Social Research; 2000.
- Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res 2005;15(9):1277-1288.
- Forman J, Damschroder L. Qualitative content analysis. Empirical Research for Bioethics: A Primer.Oxford, UK: Elsevier Publishing 2008:39-62.
- Wilkinson S. Analysing interaction in focus groups. Talk and interaction in social research methods 2006:50-62.
- Onwuegbuzie AJ, Dickinson WB, Leech NL, Zoran AG. Toward more rigor in focus group research: A new framework for collecting and analyzing focus group data. International Journal of Qualitative Methods 2009;8(3):1-21.
- Rothwell E. Analyzing Focus Group Data: Content and Interaction. Journal for Specialists in Pediatric Nursing 2010;15(2):176-180.
- Morrison-Beedy D, Côté-Arsenault D, Feinstein NF. Maximizing results with focus groups: Moderator and analysis issues. Applied Nursing Research 2001;14(1):48-53.
- Duggleby W. What About Focus Group Interaction Data? Qualitative Health Research 2005 July 01;15(6):832-840.
- Carey MA. The group effect in focus groups: planning, implementing, and interpreting focus group research. Critical issues in qualitative research methods 1994:225-241.
- Kidd PS, Parshall MB. Getting the focus and the group: enhancing analytical rigor in focus group research. Qual Health Res 2000;10(3):293-308.

