Atyanti Isworo*, Wahyu Ekowati, Asep Iskandar and Lutfatul Latifah
School of Nursing, Jenderal Soedirman University, Purwokerto, Central Java, Indonesia
*Corresponding Author:
Atyanti Isworo
School of Nursing, Jenderal Soedirman University
Purwokerto, Central Java, Indonesia
Tel: +62-(081) 845-7292
Fax: +603-22823114
E-mail: atyanti.isworo@gmail.com
Received Date: 23 December 2017; Accepted Date: 22 March 2018; Published Date: 28 March 2018
Citation: Isworo A, Ekowati W, Iskandar A, Latifah L (2018) Family Involvement Programmes on the Metabolic Response of Diabetic Patients. Health Sci J. Vol. 12 No. 2: 556.
Copyright: © 2018 Isworo A, et al. This is an open-access article distributed under the terms of the creative commons attribution license, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
DOI: 10.21767/1791-809X.1000556
Keywords
Empowerment; Family; Blood glucose; Diabetes; Glycated hemoglobin
Introduction
Diabetes is one uncured chronic disease, yet may be controlled. This controlling effort requires the patients’ compliance. It may distress the patients. However, many patients have poor compliance. Based on a research, the noncompliance average of the diabetic patients includes on diet which is not appropriate to the food planning by 35-75%, inappropriate insulin use by 20-80%, inaccuracy in recording and checking the blood glucose by 30-70%, poor foot care by 23- 52% and non-compliance to the physical exercise by 70-81% [1].
Compliance is closely related to complication and blood glucose control. It means that if the compliance is good then the complication risk may decrease and the blood glucose control may also become good. One effort to improve compliance is by involving the family. Diabetic patients require support in managing their disease. Diabetes requires an individual to have support improvement [2]. Family support is significantly related to the functional status, in which the body function may improve better with the adequate supports [3] or diabetes health status and self-care improvement [4].
Family support is related to self-care. Furthermore, Belgrave et al. [5] stated that family support is significantly related to the positive health behaviors by complying the health activities [5]. The cross-sectional study on 95 adult Hispanic patients who require insulin explores the family support and diabetes self-management. The results show that the participants are only slightly satisfied with the assistance they have already received for self-care, personal care and financial assistance, yet the family support is strongly not related to selfmanagement [4].
Family support has a simultaneously positive influence on the psychosocial health. Thus, health care intervention should involve the family support. White et al. shows that the greater the family support is accepted then the better the psychosocial adaptation to disease may become [6].
However, the phenomena show that the family feels that taking care the family members with diabetes may become a burden, not only physical but also psychic and emotional. The phenomena taking place in the hospital show that the patients expressed their sadness and surprised since their husband/ wife care no more because of feeling bored. One study explains that a negative support given by the family is the strongest predictor due to the worsening stress and disease status [7]. The other study mentions that patients with nonsupportive family for the diabetes may have the chances of 10,925 times to have poor blood glucose level [8].
Due to the significant influence of family support on health status of diabetic patients, the efforts to improve the family support are considered necessary. The purpose of this research is to figure out the influence of family empowerment model on the metabolic control of diabetic patients.
Method
The design of this research is a quasi-experimental preposttest control group design. Family empowerment model is implemented to the respondents who are divided into control and intervention group. The research samples are the diabetic patients at the age of 40-60 years old, having length of suffering period 5-10 years, are able to read and write, graduating from Senior high school education level and even Higher education, not yet experience complications (stroke, kidney failure and heart failure). Exclusion criteria: widow/ widower, patients do not live with the family. The research samples are 30 patients who are equally divided into intervention group (15 respondents) and control group (15 respondents). The scheme is completely described in Figure 1.
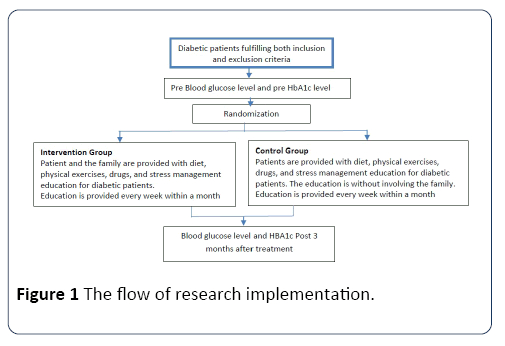
Figure 1: The flow of research implementation.
Results
The research results include the respondents’ characteristics (age, sex, education level, and occupation) as well as blood glucose and HbA1c level (Tables 1-3).
Table 1 Respondents’ characteristics (age, gender, education level, occupation).
| Characteristic |
Intervention group (N=15)
n (%) or mean ± SD |
Control Group
(N=15)
n (%) or mean ± SD |
p value |
| Sex |
| Male |
6 (40%) |
7 (46.7%) |
0.526 |
| Female |
9 (60%) |
8 (53.3%) |
| Education level |
| Senior High School |
12 (80%) |
12 (80%) |
1 |
| Higher Education |
3 (20%) |
3 (20%) |
| Occupation |
| Housewife |
6 (40%) |
5 (33.3%) |
0.135 |
| Labor |
2 (13.3%) |
2 (13.3%) |
| Civil Servant |
1 (6.7%) |
0 (0%) |
| Retired person |
2 (13.3%) |
1 (6.7%) |
| Entrepreneur |
3 (20%) |
3 (20.0%) |
| Employee |
1 (6.7%) |
4 (26.7%) |
| Anti-diabetic drug consumption |
| Metformin |
5 (33.33%) |
4 (26.67) |
1 |
| Sulfonilurea |
1 (6,67%) |
1 (6.67) |
| Metformin+Sulfonilurea |
9 (60%) |
10 (66.66) |
| Age |
53.9 ± 4.5 |
51.9 ± 6.1 |
0.265 |
| BMI (kg/m2) |
24.7 ± 5.6 |
23.9 ± 4.4 |
0.339 |
Table 2 Mean differences of blood glucose and HbA1c level before and after treatment in the intervention and control group.
| Respondent |
Mean |
SD |
N |
p value |
| Intervention group |
| Blood Glucose Level |
Pre |
277.46 |
39 |
15 |
0 |
| Post |
200.86 |
36.78 |
|
|
| HbA1c |
Pre |
10.13 |
0.639 |
15 |
0.04 |
| Post |
8.37 |
0.95 |
|
|
| Control group |
| Blood Glucose Level |
Pre |
244.86 |
46 |
15 |
0 |
| Post |
224.93 |
54.56 |
|
|
| HbA1c |
Pre |
9.47 |
1.06 |
15 |
0.002 |
| Post |
9 |
1.05 |
|
|
Table 3 Decrease differences of blood glucose and HbA1c level between those in the intervention and control group.
| Respondent |
Mean |
SD |
n |
p value |
| Blood Glucose Level |
-75.4 |
37.81 |
15 |
0 |
| of Intervention Group |
-19.53 |
33.44 |
|
|
| Blood glucose level of control group |
| HbA1c of Intervention Group |
-1.77 |
0.7 |
15 |
0 |
| HbA1c of Control Group |
-0.47 |
0.48 |
|
|
Discussion
The research results show that family empowerment influences the blood glucose and HbA1c level. This empowerment model involves families in the diabetic management. Families are directly involved in assisting the diabetic patients, starting from providing information, emotional, award, instrumental and network support.
Family involvement in diabetic treatment management may improve body health and create positive impacts [6]. The diabetic patients may obtain positive feelings and experiences that life may steadily go on when supported by the surrounding environment. The existence of a model which provides examples of healthy life style, behavior reinforcement, encouragement and meaningful people influence are factors coming from the external environment which may influence health.
Furthermore, the family involvement in handling the diabetic patients may protect them from the negative impacts caused by the disease and the required treatment [9]. Those negative impacts may become stressful conditions for the diabetic people. Physiologically, when someone is in a stressful condition, amygdala sends information to locus coeruleus triggering the autonomous system and then transmitted to the hypothalamus which results in CRF secretion. Regarding to the blood glucose level, as the response to CRF, the pituitary anterior secretes adrenocorticotrophic hormone (ACTH) in blood. ACTH is transported to the adrenal glands. ACTH stimulates the cortisol production in the adrenal cortex. Cortisol is secreted in the bloodstream. Cortisol may influence the blood glucose level increase through gluconeogenesis, protein and fatty catabolism. In addition, cortisol may also inhibit the glucose uptake by the body cells that cartisol may influence the blood glucose level [10,11].
Adequate family support positively influences catecholamines and the oxytocin-suppressed salivary cortisol level which may cause the decrease of glucose level [12]. When the blood glucose control is good, the HbA1c level may be decreased. Schafer et al. revealed that the supportive and non-supportive behaviors of the family members related to the metabolic compliance and control on the diabetic individuals. They conclude that individuals with higher nonsupportive family behavior level have lower compliance and poor metabolic control [13].
Conclusion and Recommendation
Family involvement plays a crucial role in self-management compliance and metabolic control. This findings of this study suggested that participation of family would be important aspect of diabetes care.
Acknowledgment
This research was supported by Institute for Research and Community Services Jenderal Soedirman University. The author’s thank Nia, Putri Wulan, Putri Diah Ratih and Endah Purwaningsih for their dedicated work in collecting data in this article. We are also immensely grateful to the anonymous reviewer for their comments of this article.
22213
References
- Delamater AM (2000) Improving patient adherence. Clinical Diabetes 24: 71-77.
- Guthrie DW, Guthrie RA (2002) Nursing management of diabetes mellitus: Guide to the pattern approach. Springer Publishing Company, New York.
- Fang WS (2007) Effectiveness of self-management for person with type 2 diabetes following the implementation of a self-efficacy enhancing intervention program in Taiwan.QuenslandUniversity of Technology, Queensland.
- Dimkovic N, Oreopoulos DG (2000) Chronic peritoneal dialysis in the elderly: A review. Peritoneal Dialysis International.
- Williams KE, Bond MJ (2002)The roles of self-efficacy, outcome expectancies and social support in the self-care behaviors of diabetes. Psychol Health Med 7: 127-141.
- Taylor SE (2006) Health psychology (6thedn.).McGraw Hill Book Company, Singapore.
- Pardamean E, Dharmady A (2003) Depression and negative effect of psychosocial stressor between controllable and uncontrollable diabetic mellitus at CiptoMangunkusumo National General Hospital. MajalahKedokteranAtma Jaya 2: 61-66.
- Isworo A (2009) The relationship of depression and family support to blood sugar levels of patients with type 2 diabetes in Sragen Hospital.
- Sarafino EP (2004) Health psychology: Biopsychosocial interaction (2nd edn.). John Willey & Sons Inc., New York.
- Guyton, Hall (1996) Texbook of medical physiology (9th edn.). W.B.Saunders Company, Philadelphia.
- Smeltzer, Bare (2008) Brunner &Suddarth’s textbook of medical surgical nursing. Lippincott, Philadelphia.
- Heinrichs M, Baumgartner T, Kirschbaum C, Ehlert U (2003) Social support and oxytocin interact to suppress cortisol and subjective responses to psychosocial stress. Biological Psychiatry 54: 1389-1398.
- Skarbek EA (2006)Psychosocial predictors of self-care behaviors in type 2 diabetes mellitus patients: Analysis of social support, self-efficacy, and depression.Texas Tech University, Texas.

