Keywords
Healthcare waste management practice, healthcare workers, healthcare facilities
Introduction
In waste management; healthcare wastes hold higher priority due to their hazardous nature. According to World Health Organization (WHO) some part of healthcare wastes are considered most hazardous that can affect human health and pollute the environment badly [1-4]. In a working environment that have unsafe health care waste management practices may result an exposure to infectious wastes by Healthcare workers (HCWs), patients, clients that could in turn create infection due to blood borne pathogens [1-3].
In the preceding time, many efforts have been directed toward proper and safe management of hazardous healthcare waste for less developed countries by different organizations, particularly WHO.5 However, inadequate management practices are often implemented in most healthcare facilities (HCFs) particularly in developing countries [6,7]. A number of studies on healthcare wastes management reported that health and environmental risk posed by healthcare waste can be reduced by having careful planning, proper guideline and full participation of HCWs [8-13].
Many findings in developing countries on healthcare wastes management revealed that segregation, collection of waste using recommended color coding container and storage of waste in isolated area were not satisfactory [11,12,14,15]. Personal protective equipment and accessories were not provided and not used by HCWs [14]. Moreover, healthcare wastes originating from HCFs dumped either into their backyard in a simple pit or put in open garbage to bins on the roads. Few studies done on healthcare waste management in Ethiopia indicated that there was no waste segregation in most studied HCFs [15-17]. Healthcare wastes were stored, transported, treated and disposed inappropriately at all surveyed HCFs [17].
In Ethiopia, now a day, HCFs are becoming greater than ever to address the basic health needs of the society and to achieve the Millennium Development Goal (MDG). Previous studies focused on healthcare waste management at facility level without identifying the role of each actor on healthcare waste management practices such as HCWs, waste handlers and health managers. Credible evidence show that Healthcare waste management practices of HCWs across Ethiopian health institutions is inadequate. This research revealed the gap of healthcare waste management practices of HCWs at healthcare facilities of Gondar town that could be used as baseline information to draw appropriate strategy.
Method and Material
Study design, area and population: A cross sectional survey was employed. The study was carried out in HCFs of Gondar town, Northwest Ethiopia, from April to May 2011. The town is divided into 12 areas having, 30 private and 5 governments HCFs which provide different healthcare services such as health promotion, preventive, curative, and rehabilitative for the surrounding community. Full time employee healthcare workers in those HCFs were the study population.
Sample Size and Sampling Procedure: A single population proportion formula was used to calculate the sample size considering an assumption of proportion 50%, 95% level of confidence and 5% margin of error. The final sample size of this study was 263 including 10% none response rate. Reduction formula was used as total number of HCWs in Gondar town was less than 10,000 populations. A total number of 578 and 46 HCWs were working in government HCFs and private clinics, respectively. The number of HCWs to be included from each healthcare facility was determined in proportion with the total number of HCWs found in each facility. Further proportional allocation within each healthcare facility was done to address all segments of health professionals. Then, sampling frame consisting of all HCWs in each HCF was obtained from each HCF administration offices and simple random sampling technique was used to select HCWs.
Operational definitions: Knowledge of the respondent’s (on healthcare waste type, manuals and diseases transmitted with contact of infectious waste) is measured based on the bloom’s criteria. Respondents with a higher knowledge, answered correctly greater than 80% of knowledge questions; respondents with a moderate knowledge, answered correctly in between 60-79% of knowledge questions; those who answered correctly less than 59% were considered as respondents that have low knowledge [18].
Healthcare waste management practice of healthcare worker’s is measured and assessed as practice if the respondent is doing all the four indicators for healthcare waste management practice (always using gloves during handling of waste, segregate wastes with the available containers, treating infectious wastes and using always the available waste bins).
Data collection tools: Questionnaires and field observation check list were prepared from WHO recommendation assessment tool and were used to describe the healthcare waste management practices of HCWs in healthcare facilities. The questionnaire included questions about demographic characteristics, as well as knowledge, and practices of HCWs about healthcare waste management. The practice of healthcare waste at provider level was assessed by asking four questions which had yes or no response. A score of 1 was assigned to the answer “yes” and a score of 0 assigned to “no” answers. The total scores of practice questions ranged from 0 to 4. If the HCW was scored four out of four questions he/she considered as practiced. Observational checklist was used to collect the real practice on waste segregation, wastes collection material, treatment of infectious wastes. This is aimed to support the quantitative findings and to provide additional information about the healthcare wastes management practice and working conditions, as well as to identify the main hazards to human health and safety as well as to the environment, resulting from the existing practices.
Data quality assurance: The questionnaire was prepared originally in English and translated to Amharic (native language) and back to English by different language experts to ensure the accuracy of the questions. Training was given for data collectors and supervisors. Pre testing of questionnaire was made to assess the validity of the questions in out of the study area. On spot-checking and reviewing the completed questionnaires were made by principal investigator and supervisors on daily bases to ensure completeness and consistency of the information collected.
Data analysis: Questionnaires first were coded and data were entered and analyzed with Statistical Package for the Social Sciences version 16 software. Descriptive statistics were computed. Binary logistic regression and multivariate analyses were used to identify predictor variables for practice of healthcare providers.
Ethical clearance: Ethical clearance was obtained from the Ethical Approval Committee of University of Gondar. A formal letter was given to each HCFs and permission was secured at all levels. Informed consent was taken from each study participants and their responses were kept confidential.
Results
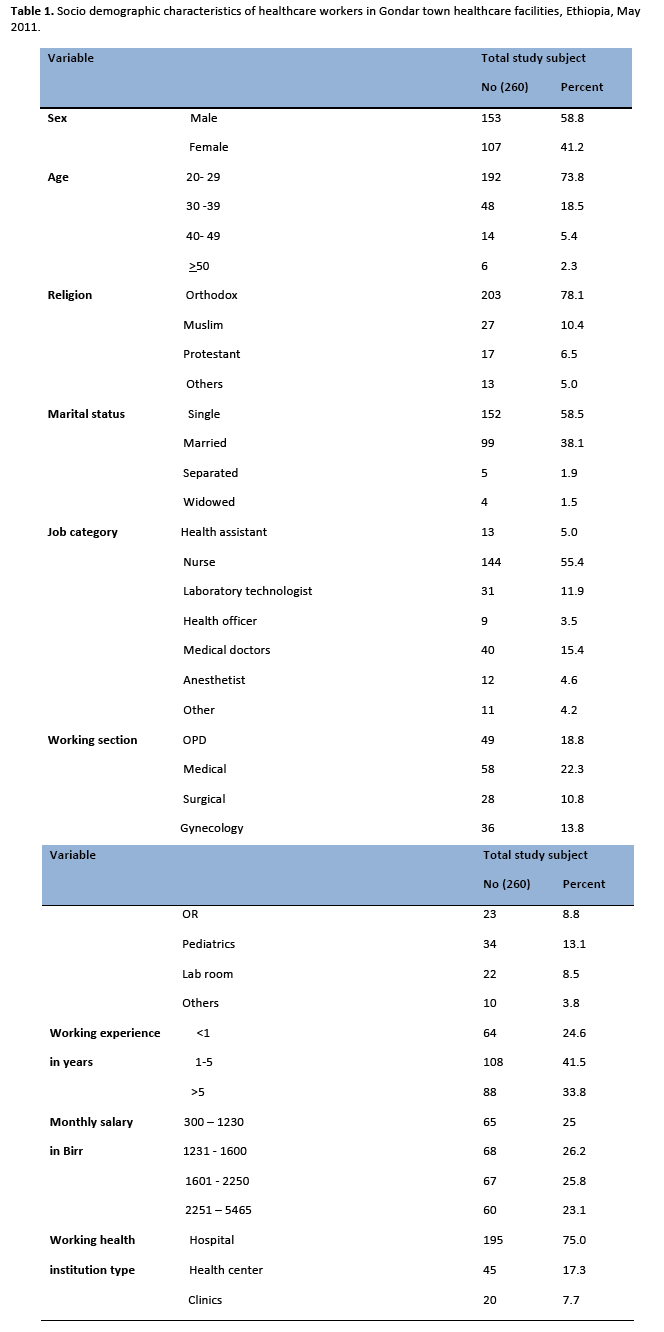
A total of 260 HCWs were participated in the study. One hundred fifty three (58.8%) were males. The mean age of the respondents was 28 + 6.4 years. One hundred fifty two (58.5%) were single and 203 (78.1%) were Orthodox Christian by their religion. The majority of respondents were nurse (144, 55.4%), working at medical ward (58, 22.3%) and had worked one up to five years (108, 41.5%). Income of the respondents ranged from 300 to 5465 birr ($ 17 to 321) and the overall average was 1851 ± 881($ 109 ± 52). The majority of the respondents, 195 (95.0%) were working in hospitals and the least, 20 (7.7%) were working in clinics (Table 1).
Of the total respondents, 78(30%), 99 (38.1%) and 83 (31.9%) had higher, moderate and lower knowledge on diseases transmission with healthcare waste, respectively. However, the majority (202, 77.7%), 45 (17.3%) and 13 (5%) had low, moderate and higher knowledge on healthcare waste types and color coding containers for healthcare waste and the responsibility of healthcare waste segregation, respectively.
Two hundred fifty two (96.9%) of the HCWs did not access to any guideline documents. One hundred thirty eight (53.1%) of HCWs did not take any training about healthcare waste management. The prevalence rate of needle stick and a sharps injury in the preceding 12 months was 65 (25%). Of this, 6 (9.6%) of the injuries were occurred during handling of healthcare wastes. One hundred nine (49.1%) of respondents reported that there was no safety instruction at their work environment.
Healthcare waste management practices of respondents
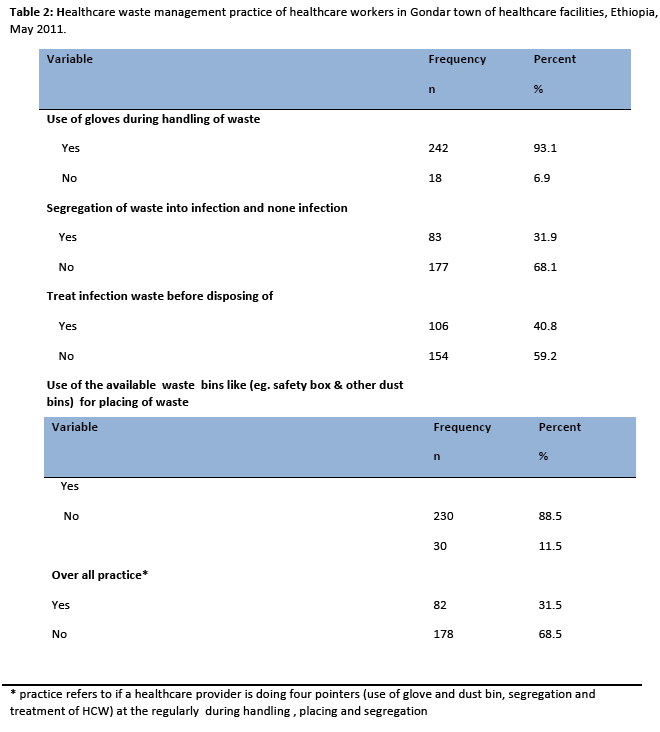
HCWs reported that 82 (31.5 %) of them were doing healthcare waste management practice. Two hundred forty two (93%) of the respondents used gloves during handling of healthcare wastes. Only 106 (40.8%) of respondents treated infectious wastes with sterilization, and disinfection before disposing off. Only eighty three (31.9%) of respondents segregated wastes by type at point of generation. Most of the respondents, 230 (88.5%) used the available waste bins for placing of healthcare wastes (Table 2).
Factors associated with healthcare waste management practice
In multivariate logistic regression analysis, healthcare institutions type, training on healthcare waste, knowledge on healthcare waste type and knowledge on diseases transmission via healthcare waste had a significantly associated with healthcare waste management practice. Healthcare workers who worked at health centers {AOR: 3.10, 95% CI: (1.33, 7.25)} and clinics {AOR: 4.95, 95% CI: (1.72, 14.29)} were 3.10 and 4.95 times more likely to practice healthcare waste management than healthcare workers who worked at hospitals, respectively (Table 3).
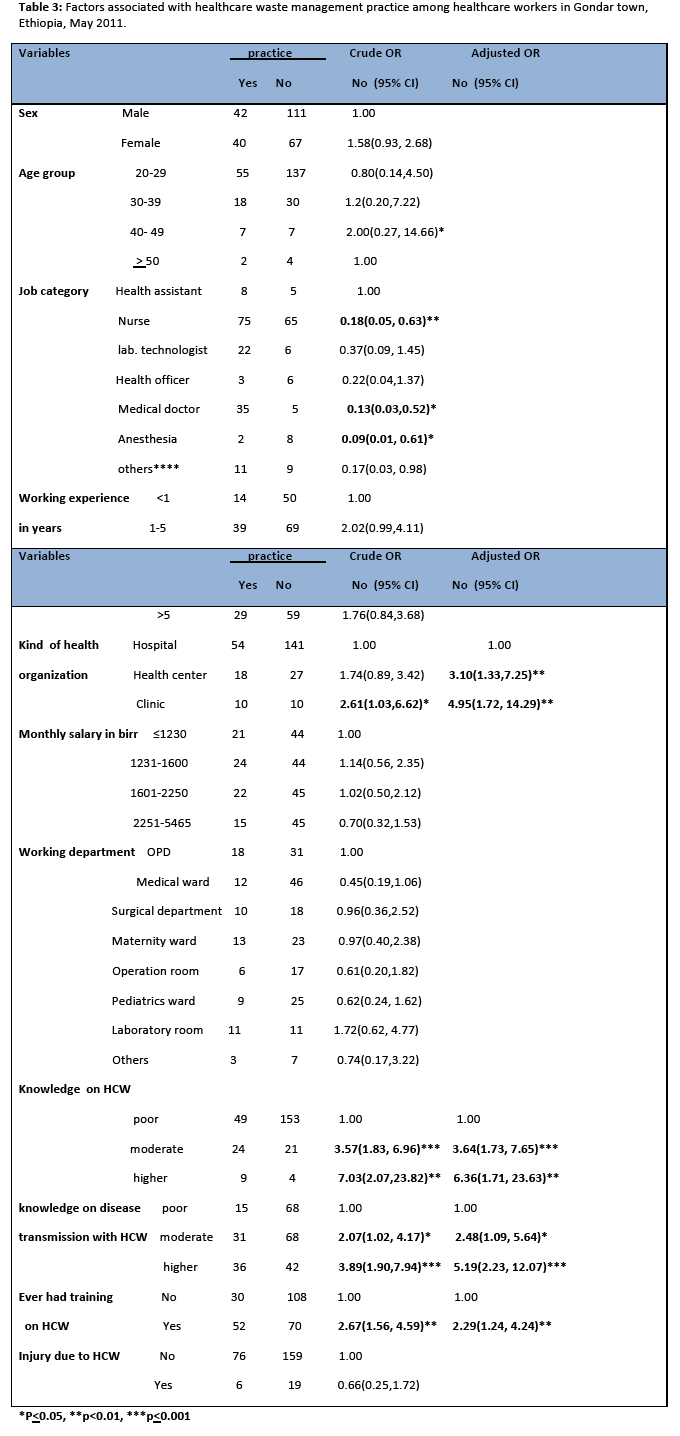
This study claimed that those who had higher knowledge about the type of healthcare waste were 6.38 times [AOR: 6.38, 95% CI: (1.71, 23.63)] and moderate knowledge were 3.64 times [AOR: 3.64, 95% CI: (1.73, 7.65)] more likely to practice healthcare waste management compared with HCWs who had low knowledge. Similarly, those who had higher knowledge on diseases transmission with healthcare waste were 5.19 time [AOR: 5.19, 95% CI: (2.23, 12. 07)] and moderate knowledge were 2.48 times [AOR: 2.48, 95% CI: (1.09, 5.64)] more likely to practice healthcare waste management than HCWs who had low knowledge about diseases transmission through improper healthcare waste management (Table 3).
Training on healthcare waste was remained a significantly associated with healthcare waste management practice after adjusting in multivariate analysis. Healthcare workers who took training on healthcare waste were 2.29 times more likely to practice healthcare waste management than their counter parts who didn’t take training on healthcare waste management [AOR: 2.29, 95% CI: (1.24, 4.24)] (Table 3).
Qualitative results from observational checklists revealed that all surveyed HCFs didn’t have appropriate and adequate color coded containers and plastic bags for healthcare wastes collection but in one section (laboratory room) of one surveyed HCFs had different labeled punctured proof plastic containers for collection of infections and noninfectious waste. All HCFs had perforated dustbins to collect healthcare wastes and in some sections punctured proof safety boxes were used to collect sharp wastes. The overall site observation in all surveyed HCFs had no adequate and appropriate labeled containers for collection of healthcare waste. There was no any guide line for healthcare waste management in one of the surveyed HCFs
The type of healthcare waste transportation methods employed by HCFs and other human-related healthcare activities was surveyed. It was found that healthcare wastes were transported manually to the backyard disposal site of the HCFs in nine out of eleven surveyed HCFs. However, some section of two surveyed HCFs healthcare wastes were transported using wheeled trolleys or carts. In general the means of transportation of healthcare waste in all surveyed HCFs was not in line with the WHO recommended standard.
Of the eleven surveyed HCFs, some section of the five HCFs had an attempt to treat infectious waste before dispose of using either barakina or alcohol. In one of the surveyed HCFs, autoclave was used to treat biohazard waste at their laboratory rooms. The waste was treated on-site by using either open burning or controlled incineration in all surveyed HCFs. All surveyed HCFs used open burning to treat dressing materials and three out of eleven used incinerators to treat sharp wastes.
It was found that all surveyed HCFs didn’t have a temporary storage area for healthcare wastes. Healthcare wastes were stayed in each section of HCFs and took to the back yard disposal site within twelve hours. However, in maternity section of five surveyed HCFs pathological wastes were taken into placenta pit after the healthcare services had been completed.
The survey results also showed that all HCFs dispose of their waste in unsanitary way. The final disposal locations for most HCFs didn’t meet the standards of WHO requirements. Some of the buried disposal sites were constructed either near to water bodies, or wards, or residential area. Open burning and incinerator were the common methods of disposing of healthcare wastes in all surveyed HCFs. Only six out of eleven HCFs had incinerator which are made from breaks and these incinerators had poor efficiency due to lack of regular maintenance and the air inlet parts were blocked with ash. Ash disposal pit were not employed for those HCFs which had incinerators. All HCFs had placenta pit to dispose placenta.
Discussion
It is known that WHO has prepared healthcare waste guideline manual to ensure safe healthcare waste management. Moreover, Quality and Standard Authority of Ethiopia (QSAE) in 2004 and Ministry of Health (MOH) in 1997 had prepared guideline on handling and disposal of waste materials within HCFs [19]. In this study, the majority (96.9%) of HCWs did not have any guideline documents on healthcare waste management. Moreover, the qualitative result of this study confirms that there was no healthcare waste management document at the working area in one of the surveyed healthcare facilities. This result is similarly with the study done in Ethiopia in 2007 indicated that this document was not there in one of the surveyed HCFs [20]. A study done in Ethiopia in 2009 reported that the availability of this document was 15% of the surveyed HCFs [15]. In North Jordan, 29% of the surveyed health facilities have polices on healthcare waste but only 10% of them had formal guideline on healthcare waste management [21]. However, the accessibility of healthcare waste management documents for healthcare professional in South Africa was 91% which is different from the result of this study [22]. This difference may be due to lack of regular supervision and enforcement of standard practice by responsible body.
This study revealed that 20.8% of respondents knew about the existence of the WHO manual on safe management of healthcare waste. This result is inconsistent with the study done in South Africa about 46% of HCWs knew the existence of the WHO manual on healthcare waste.22 The finding of classification of healthcare waste by WHO in this study were known by 11.2% of the respondents and color coding of waste bins were known correctly by 10.0% of HCWs. This finding is different from the study done on assessment of biomedical waste management in Ludhiana, India indicated that 95.8% HCWs knew classification of healthcare waste and color coding system was known by 93.7%.23 This difference may be due to the degree of emphasis of HCFs on healthcare waste management, on job training and the accessibility of healthcare waste management documents in the working environment.
This study revealed that greater than 99% of HCWs agreed that improperly managed healthcare wastes can transmit infection for HCWS and patients. This result is consist with the study done in South Africa indicated that most of HCWs (98.5%) agreed that improper management of healthcare waste could lead to the transmission of infections among HCWS and patients [22]. Similarly, the result of other studies; the awareness of HCWs in Ludhiana, India (92.1% - 98.0%) in 2011 was consistent with this finding but the awareness of HCWs in Srinagar, India (86%) was lower than the results of the current study [23,24]. This difference may be due to the time gap of the study.
Healthcare waste management practices at healthcare provider level are some of the important practices in the process of waste management that can be affected by the knowledge and the risk perception of healthcare providers [23-25]. Proper placing of waste in the ward with appropriate containers requires the ensuring of adequate materials for collection of healthcare waste. In this study 31.9% of healthcare providers reported that they segregated waste by their type with the available dust bins. This result is lower than the study done in South Africa and India indicated that 97% and 67% of HCWs segregated healthcare waste into readily available waste bins, respectively [22,26]. This difference could be explained by the ensuring of different types of containers in HCFs by responsible body and the low enforcement of the regulatory body.
Qualitative results of this study showed that all surveyed HCFs (eleven) had no adequate, labeled and appropriate collection containers for collection of all types of healthcare wastes. Five out of eleven surveyed health facilities (45%) had puncture proof container to collect sharp wastes and the rest had used plastic containers to collect sharp wastes. Poor segregation of waste in this study is comparable with the study in Hawassa city of Ethiopia and the study done by Making Medical Injection Safer United States Agency for International Development (USAID) in 2009 in Ethiopia where wastes were segregated in 46% (32 of the 72) of the surveyed HCFs [17,19].
Majority of the respondents (93.1%) in this study used gloves during handling of healthcare wastes and 89 % of the HCWs used available containers for healthcare waste collection. This result is similar with the study done in South Africa, 95% of the HCWs used gloves during handling of healthcare waste.22 In this study 40.8% of the respondents treated infectious wastes with different methods before disposing off which is inconsistent with the study done in South Africa most respondents (90%) treated infectious healthcare waste before disposing of [22]. This difference may be due to the availability of treatment methods with the HCFs, sense of responsibility by HCWs and regular supervision of the responsible body.
In this study 53.1% of the HCWs did not take any training on healthcare waste management. HCWs reported that 31.5 % of them were doing healthcare waste management practices where as 68.5% did not perform healthcare waste management practices. This finding is incomparable with other studies in India most HCWs were in accordance with the prescribed rules and standards of the hospital [23]. This could be due to the budget allocation of HCFs, the accessibility of healthcare waste management document and on job training. Beside this, qualitative findings reported that all surveyed HCFs had no adequate number of containers and biohazard bags for healthcare waste management. This finding is in agreement with study done in Hawassa city of Ethiopia and Nigeria [17,27].
Different studies stated that hospitals generate high amount of healthcare waste due to patient flow and invasive procedures which in turn influence on healthcare waste management practice at HCWs level than health centers and clinics [17]. Thus healthcare waste management practices in hospital required commitment of HCWS, adequate financing, regular supervision and enforcement [17,21,22,27]. This study also revealed that those who worked at health center and clinics were 3.10 and 4.95 times more likely to practice healthcare waste management than HCWs worked in hospitals.
Findings of different studies reported that knowledge on healthcare waste type and diseases transmission through contact of infectious waste had an influence on practice of healthcare waste management [17,19,24,25,27,28]. Similarly this study claimed that those who had higher and moderate knowledge on healthcare waste type were 6.38 and 3.64 times more likely to practice healthcare waste management than those who had low knowledge on healthcare waste type, respectively. Moreover, this result indicated that those who had higher and moderate knowledge on diseases transmitted with contact of infectious wastes were 5.19 and 2.48 times more likely to practice healthcare waste management than those who had low knowledge on diseases transmitted with contact of infectious wastes, respectively.
Many literatures indicated that regular training of HCWs on healthcare waste management had a great role on practices of healthcare waste management [17,21,22,24,25,27,28]. This study also indicated that those who took training on healthcare waste management were 2.29 times more likely to apply healthcare waste management practice than their counterparts.
Conclusion
The overall findings of this study indicated that the majority of HCWs did not apply the recommended healthcare waste management practice set by WHO. Moreover, the current healthcare waste management practice in studied health facilities was managed improperly and can pose a risk for human health and the environment. Segregation of wastes was not practiced in all surveyed HCFs and by majority of HCWs. Also, inadequate supply of color coded containers, lack of guideline for healthcare waste management, and low commitment of HCWs were observed. Furthermore, knowledge on healthcare waste type, knowledge on diseases transmitted with contact of infectious wastes, training and availability of guideline documents were significantly associated with healthcare waste management practices of HCWs.
Recommendation
Regular training on healthcare waste management should be given to HCWs to improve the current practices. Regular supportive supervision of wards and other areas of HCFs by senior administrators should be done to ensure compliance of safe healthcare waste management. Segregation of waste should be done at point of generation. Healthcare facilities should have healthcare waste management guideline and further research should be carryout on risk assessment..
2931
References
- Johannessen LM, Dijkman M, Bartone C, Hanrahan D, Boyer MG, Chandra C: Health Care Waste Management Guidance Note. Washington DC: World Bank; May 2000.
- Sawalem M, Selic E, Herbell JD: Hospital waste management in Lybia: A case study. Waste Management 2009; 29: 1370-75.
- Pruss A, Giroult E, Rushbrook P: Safer management of wastes from health care activities. World Health Organization, Geneva, 1999.
- Akter N: Medical waste Management Review Environmental Engineering program January 2000.
- Shinee E, Gombajav E, Nishimura A, Hamajima N: Health waste management in the capital city of Mongolia. Waste Management 2008; 28: 435-44.
- World Health Organization. Healthcare waste management, WHO October 2004; Fact sheet No.281
- Patwary MA, O’Hare WT, Street G, Elahi MK, Hossain SS, Sarker MH: Quantitative assessment of medical waste generation in the capital city of Bangladesh. Waste management 2009;29(8): 2392-2397.
- Silva CE, Hoppe AE, Ravanello MM, Mello N: Medical wastes management in the south of Brazil Waste Management 2004;25(6):600-605.
- Blenkharn JI: Standards of clinical waste management in UK hospitals. Journal of Hospital Infection 2006; 62: 300-303.
- Blenkharn JI: Standards of clinical waste management in hospitals – Second look, Journal of Hospital Infection 2007; 121: 540-545.
- Mostafa GMA, Shazly MM, Sherief WI: Development of a waste management protocol based on assessment of knowledge and practice of healthcare personnel in surgical departments. Waste Management 2007; 29 (1): 430-439.
- Coker A, Sangodoyin A, Sridhar M, Booth C, Olomolaiye P, Hammond F: Medical waste management in Ibadan, Nigeria: Obstacles and prospects. Waste Management 2008;29(2): 804-811.
- WHO (World Health Organization) (2005a): Healthcare waste management. Genva: WHO. Feb. 26, 2009. Available online from: URL: [www.healthcarewaste.org]
- Patwary MA, O’Hare TW, Sarker MH: Assessment of occupational and environmental safety associated with medical waste disposal in developing countries: A qualitative approach. Safety science 2011;49(8-9):1200-1207.
- MMIS (Making medical injection safer): Evaluation of injection safety and health care waste management in Ethiopia. 2009 final report.
- Solomon D: Healthcare waste management in Ethiopia in 2005: A review. Ministry of labor and Social Affairs, Addis Ababa, Ethiopia.
- Deneke I, Aquiet M, Desalegn B, Atebha H. Assessing the management of healthcare waste in Hawassa city, Ethiopia. Waste management and research 2011; 29(8):854-862.
- Blooms BS. Taxonomy education objectivities: the classification of educational goals by a committee of college and university examiners. 1956. New York: longman, green.
- Disease Prevention and Control Department, Federal Ministry of Health Ethiopia: Infection prevention guidelines for Healthcare Facilities in Ethiopia. Addis Ababa, Ethiopia 2004
- Azage M, KumieA.Healthcare waste generation and its management system: the case of health centers in West Gojjam Zone, Amhara Region, Ethiopia. Ethiopian Journal of Health Development 2010; 24(2):119-126.
- Abdulla f, Qdais HA, Rabi A. Site investigation on medical waste management practice in northern Jordan. Waste management 2008; 28(2):450-458.
- Ramokate T, Basu D: Healthcare waste management at an academic hospital: knowledge and practices of doctors and nurse. South African Medical Journal 2009;99(6): 444-450.
- Mathew SS, Benjamin AI, Sengupa P: Assessment of biomedical waste management practices in a tertiary care teaching hospital in Ludhiana. Healthline 2011; 2(2):28-30.
- Wasee Q, Hassan G, Baba A, Kadri SM, Nazi K: Awareness of biomedical waste management amongst staff of the governemtn S M H S hospital, Srinagar A Tertiary level hospital in Kashmir valley. JK-Practitioner 2007; 14(1):60-66.
- Rao PH. Report: Hospital waste management-awareness and practices: a study of three states in India. Waste management and research 2008;26: 297-303.
- Shafee M, Kasturwar NB, Nirupama N: Study of knowledge, attitude and practices regarding biomedical waste among paramedical workers. Indian Journal of Community medicine 2010; 35:369-370.
- Abah SO, Ohimain EI: Healthcare waste management in Nigeria: A case study. Journal of Public Health and Epidemiology 2011;3(3): 99-110.
- Gehan MA, Mostaf MM, Shazly M, Wafaa IS: Development of a waste management protocol based on assessment of knowledge and practice of healthcare personnel in surgical departments. Waste Management 2009;29(1): 430-439.

