Introduction
It is of great importance to meet physical needs of the individuals with chronic diseases. Especially deterioration in daily living activities and limitation of physical activity cause these patients to feel most uncomfortable [1]. The individual or family with a chronic disease goes through personal and emotional loss owing to loss of self-reliance, self-respect, status in family and independence, rejection and despair [2,3]. Chronic diseases are the cases that require long-term monitoring, control, and care because of the fact that they may lead individuals to be dependent at varying rates in activities of daily living and may cause permanent impairment. Since it is not possible to carry out monitoring and care in hospital environment, they should be carried out at home [4]. For this reason, there is a need for quality home care services. Home care is a part of comprehensive health care process that includes providing health services such as improving health, maintaining health, regaining health, minimizing the effects of a disease or impairment, maximizing the level of independence, providing end-of-life care in the places where the individuals and families live [5].
Amyotrophic Lateral Sclerosis (ALS) is one of the chronic diseases that have an increasing prevalence, and ALS patients are dependent on others and nursed by their relatives at home rather than at a hospital [6]. Amyotrophic Lateral Sclerosis (ALS) is a neurodegenerative disease of unknown etiology that affects the population of motor neurons located in motor cortex, brain stem, and spinal cord. The incidence of ALS in the society is 0.86- 2.4/100.000 and the prevalence is nearly 6/100.000 [4,5,7-9]. Epidemiological predictions show that the incidence of ALS is going to increase in the next ten years, and this increase is going to stem from disease-specific findings rather than economic conditions or health care services [4,10]. Even though ALS can be seen in both genders, it can be observed 1.2-1.4/1 times more among men than women. Moreover, it is stated that there is a slight female preponderance in bulbar-onset ALS, yet there are not consistent data on gender in familial ALS cases [9,11,12].
The fact that ALS patients are looked after by their families causes physical, psychological, social and economic problems for patients and their families [12,13]
The fact that individuals are nursed by their relatives makes them feel physically and psychologically better. However, the studies done indicate that caregivers meet some problems [14,15]. It is highlighted that especially an old-aged caregiver, working life, and inadequate social support may increase the risk [13].
Aim of the Study
The aim of the present study was to explore the home-care needs and quality of life of the patients with Amyotrophic Lateral Sclerosis (ALS), the care-burden and quality of life of caregivers, and the efficacy of nursing education given to caregivers in line with their needs.
Methodology
Research design
This study employed a single-group, quasi-experimental, pretest– posttest design with repeated measures. A sampling selection was not made in the study. The patients and primary caretakers who met the criteria for participation in the study were accepted into our study that lasted from May to November 2007. The criteria for participating in the study were that both the patients and the caregivers should be over 18 years of age, that they voluntarily accepted participating in the study, that they did not have any cognitive and psychological problems and that they were patients who had been diagnosed with Amyotrophic Lateral Sclerosis (ALS) and were cared for by primary caretakers in their own homes.
The study was started by reaching the addresses and telephone information of the patients with ALS who were registered in the neurology clinics of two university hospitals and two research training hospitals in western Turkey. The patients and caregivers were reached by telephone and told about the importance and purpose of the study. The patients and caregivers who agreed to take part in the study were visited in their homes at a time and on a day when they were available.
The study data were gathered in two stages.
First stage
It was aimed in the first stage of the study to determine the participation of patients and caregivers in daily living activities (ADL) and their positions of receiving help, qualities of life and the burden of caregivers and the areas of training for which they felt a need.
In the first interview, patients and caregivers who were visited in their homes filled in “Patient Introductory Form” and “Caregiver Introductory Information Form”. At this stage, the data were gathered through “Daily Living Activities Help/Need Form” of ALS patient to determine the home-care needs of the patients, [8,16] through the “Duke Health Profile” (DUKE) to determine the quality of life of the patients and caregivers before effective nursing education [17,18], through the Caregiver Burden Inventory (CBI) to determine the caregivers’ burden [19]. These forms were filled in by the patients and caregivers themselves or by the researchers in cases where the patient was illiterate or with motor skills disorder during face-to-face interview.
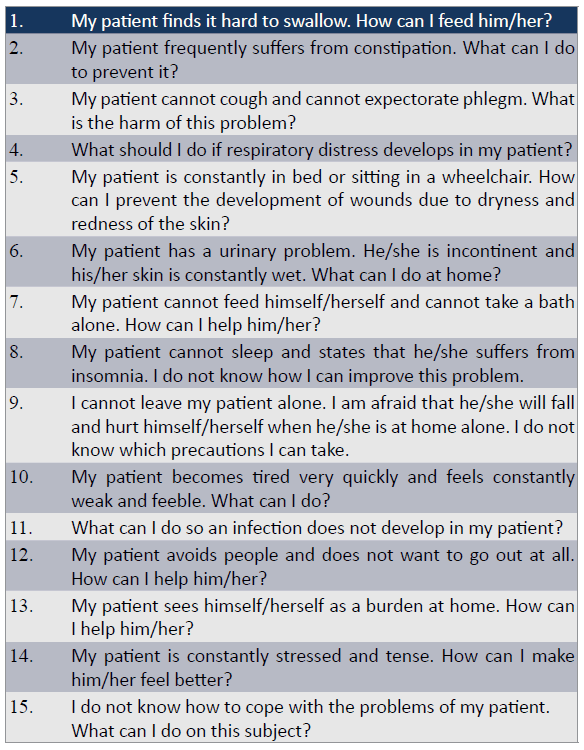
The caregivers were asked to determine the areas they needed to get education about through 16 cards that included important questions and were prepared by the method of card sorting in order to determine the needs of caregivers [20-22]. The problems were prepared according to the nursing diagnosis of NANDA (North American Nursing Diagnosis Association). 15 problems that can be met in the care for ALS patients were written separately on each card and the caregivers were asked to choose the most important one for them. Moreover, they were asked to write another important problem to them which was different from the ones on the other cards on the sixteenth blank card (Box 1). It took approximately 10 minutes for the caregivers to understand the questions included on their cards and to list them in order of importance.
A visual presentation was prepared for caretakers according to the training needs they determined by using the Power Point program. The training given lasted an average of 40 minutes. Furthermore, a booklet titled “Care Guide for ALS Patients and Their Relatives” was prepared by the researchers by scanning the national and international literature and given to the patients and caregivers for their continuous use.
Second stage
At the second stage of the study, the patients and caregivers were given a second visit at least one month after the first one, the CBI and DUKE scales were filled in again by the caregivers, and the effect of education on caregivers’ care-burden and quality of life was evaluated.
Instruments
Daily Living Activities Help/Need Scale of ALS Patients (ADL): It is a form in which the home-care needs of the patients diagnosed with ALS are based on Roper, Logan, and Tierney’s Activities of Daily Living Model (1980-1981-1983) and Gordon’s Functional Health Patterns (1982) [8,16]. Daily Living Activities (ADL) Help/ Need Form of ALS Patient is a form that includes 15 items on a 0-4 point Likert-type scale. For each item, the thing to do is to circle one of the choices that mostly describes the person’s condition: “totally independent”, “uses a device”, “needs human assistance”, “needs device and human assistance”, “completely dependent”. The answers are scored on a scale of 0 through 4. Score interval is 0-60. The fact that the person’s total score is high determines his/her level of participation in daily living activities.
Duke health profile: The “Duke Health Profile” (DUKE) developed by Parkerson (1990) was used in this study and was adapted to Turkish by Kuzu et al. (2004) and the validity and reliability of the scale for the Turkish culture was made. The Duke Health Profile is a 17-item scale. It measures six functional areas including physical health, mental health, social health, general health, perceived health, and self-esteem; and five dysfunctions including anxiety, depression, anxiety-depression, pain, and disability. The scale is scored from 0 to 100. A high score indicates high quality of life; a low score indicates low quality of life [17,18].
Care Guide for ALS patients and their relatives: A booklet titled “Care Guide for ALS Patients and Their Relatives” was prepared by the researchers by scanning the national and international literature related to the subject. Included in the booklet are the physical, social and mental problems experienced due to the ALS disease and the care suggestions for these problems.
Caregiver burden inventory: It is used for determining the difficulties caregivers encounter while taking care of their patients and their state of having difficulty in providing care. Novak and Guest (1989) developed the Caregiver Burden Inventory that measures the five factors of burden (time-dependence, developmental, physical, social, and emotional) considering the idea that burden is multi-dimensional. The Burden Inventory of caregivers was adapted to Turkish by Küçükgüçlü (2004) and the validity and reliability of the scale for the Turkish culture was made [23]. This inventory is a 24-item Likert-type (0-4) scale. Each factor can be scored from 0 to 20. Scoring is done this way: never (0 point), rarely (1 point), sometimes (2 points), quite frequently (3 points), nearly always (4 points). The total score of each individual ranges from 0 to 100. A high score indicates high level of burden; a low score indicates low level of burden [19].
Patient/Caregiver introductory information form: It is a form that is specially prepared for patients and includes demographic information and information on the disease and care.
Statistical analyses
Data were analyzed using the Statistical Package for the Social Sciences ver. 15.0 software (SPSS, Chicago, IL, USA). Descriptive statistics, such as means, standard deviations (SD), and percentages, were used to describe the demographic and clinical characteristics of the participants. The relationship between the variables was assessed using Pearson’s correlation coefficient. Diagnostic group differences in variables were assessed using student t-test or one-way analysis of variance (ANOVA) and Post Hoc test. P<0.05 was considered statistically significant. Cluster analysis was done in order to evaluate the questions on the cards. The ranks of importance have been determined within each other for the cards with the Ward’s method and have been classified as of very importance, of average importance and of less importance.
Research ethics
The study was approved by the Ethics Committee of School of Nursing, ?zmir, Turkey. Permissions were received from the hospitals where the research was carried out. Furthermore, in order to realize the study, written permissions were obtained from the scale authors and patients and caregivers accepting to participate in the study.
Results
Thirty patients were reached within the scope of the study. 76.7% of the patients were male, 73.3% were 46 years old and above, 73.3% were married, and 40.0% were high school graduates (Table 1). Ninety percent of the caregivers within the scope of the study were female, 50.0% of them were 20-45 years old, and 80.0% were married. 43.3% of the caregivers stated that they were high school graduates, 60.1% were retired (Table 1), and 60.0% were the patient’s spouse.
Table 1: Patient and caregiver characteristics
| Characteristics |
ALS patients (n=30) |
Caregivers (n=30) |
Age (years)
Range: 20-45
46 and older |
8 (26.70)
22 (73.30) |
15 (50.00)
15 (50.00) |
Gender, n (%)
Men
Women |
23 (76.70)
7 (23.30) |
3 (10.00)
27 (90.00) |
Education, n (%)
Elementary School graduate
Secondary School graduate
High School graduate
University graduate |
7 (23.30)
5 (16.70)
12 (40.00)
6 (20.00) |
8 (26.70)
9 (30.00)
13 (43.30)
- |
Marital Status, n (%)
Single
Married |
8 (26.70)
22 (73.30) |
6 (20.00)
24 (80.00) |
The ALS diagnosis age of 43.3% of the patients participated in the study was 3-4 years. The patients also stated that they had endocrine-metabolic (20.0%), cardiovascular (16.7%), respiratory system (13.3%) diseases.
Sixty-three percent of the patients stated that their disease affected their economic situation; 46.7 % said it affected their household responsibilities; 36.7% said their work–related responsibilities got affected by it. 86.7% of the patients stated that they needed assistance in their home life and 23.3% in their work life; 76.7% stated that their disease affected their social life, 70.0% said it affected their meeting with friends or relatives, and 63.3% said it affected their sharing thoughts and feelings with their friends and relatives. 93.3% of the ALS patients stated that they got assistance with their care, and 60.0% of the ones who got assistance said that their caregivers were their spouse. 60.0% of the caregivers who took part in the study stated that they gave care to their patients for 6 months to 2 years, 93.3% said that they did not get any help from other family members while giving care, and 30.0% said that they gave care for 13 hours or more per day.
The caregivers were asked to determine the areas they primarily needed to get education about through 16 cards that included important questions and were prepared by the method of card sorting in order to determine the needs of caregivers [20-22] (Questionnaire 1). Therefore, they put the problems on each card in order of importance. As a result of the study, the ones below were respectively determined to be very important questions and problems caregivers most needed to get education about: “My patient finds it hard to swallow. How can I feed him/her? My patient frequently suffers from constipation, what can I do to prevent it? My patient cannot cough and cannot expectorate phlegm. What is the harm of for this problem? What should I do if respiratory distress develops in my patient? My patient cannot feed himself/herself and cannot take a bath alone. How can I help him/ her (Questionnaire 1)?”
The lowest and highest values, mean scores, standard deviation values of the responses given by the caregivers participating in the study to the CBI and its sub-dimensions were calculated. According to this, the pretest and posttest application total mean scores of the scale ranged from 60.13 to 53.23; and standard deviation values ranged from 23.93 to 25.12 (Table 2). The relationship between the pretest and posttest application total mean scores of the CBI was found statistically significant (r=0.93, p=0.00, p<0.05).
Table 2: The distribution of the responses given by the patients and caregivers to the scales used in the study.
| Variables |
Caregivers (n=30) |
Patient (n=30) |
Activities of Daily Living
Help/Need (mean ± S.D) |
20.07 ± 4.07 |
20.13 ± 10.34 |
Duke Health Profile (mean ± S.D)
Pretest
Posttest |
18.07 ± 5.97
20.07 ± 4.07 |
12.67 ± 7.45 |
Caregiver Burden Inventory (CBI) (mean ± S.D)
Pretest
Pretest |
60.13 ± 23.93
53.23 ± 25.12 |
-
- |
Whereas a significant relationship in correlation was not found between the total mean score the patients got in the DUKE scale and the mean score the caregivers got after the pretest application of the DUKE scale (r=0.14, p=0.461, p>0.01), a significant relationship was found between the posttest application total mean scores (r=0.63, p=0.00, p<0.01). According to this result, that the caregivers were given one-to-one education in parallel with their needs increased their quality of life and this also had an effect on the patients. It can be said that the education had a positive effect on the quality of life of both the patients and caregivers.
Questionnaire 1 The list for the problems the caregivers needed education about.
The relationship between the total mean score of the ADL scale of the patients and the DUKE scale total mean scores of them was found statistically significant (r=-0.73, p=0.00, p<0.01). According to these findings, it can be said that the more the patients participated in daily living activities, the higher their quality of life.
As the relationship between the total ADL mean scores of the caregivers and their total CBI mean scores was analyzed, except for the developmental and emotional burden subscales of CBI total mean scores (r=0.298, p=0.110, p>0.05), the relationship among the other item total mean scores was found significant at the end of the pretest application. As a result of the posttest application, the relationship among all the item total mean scores was found significant (p<0.05).
The pretest and posttest application total mean scores of the DUKE scale of the caregivers were found between 18.07 and 20.07; and the standard deviation value was found between 5.97 and 4.07 (Table 2). As the relationship between the pretest and posttest application total mean scores of the DUKE scale of the caregivers was analyzed, a statistically significant relationship was not found (r=0.11, p=0.12, p>0.05).
The lowest and highest values mean scores, and standard deviation values of the responses given by the caregivers and patients to the ADL scale were calculated, and the total mean scores of the scale were found between 20.13 and 20.07; standard deviation values ranged from 10.34 to 4.07 (Table 2).
The relationship between the ADL total mean score of the patients and their DUKE scale total mean scores was found statistically significant (r=-0.73, p=0.00, p<0.01).
While the relationship between ADL total mean score of the caregivers and the pretest of the DUKE scale mean score was not found significant (r=0.30, p=0.10, p>0.05), the relationship between ADL total mean score and the posttest application of the quality of life scale total mean score was found significant (r=0.57, p=0.00, p<0.01).
As the relationship between the ADL total mean scores of the caregivers and their CBI total mean scores was analyzed, except for the pretest CBI application of the developmental and emotional burden subscales total mean scores (r=0.29, p=0.11, p>0.05), the relationship among the other item total mean scores was found significant. As a result of the posttest application of the CBI, the relationship among all the items total mean scores was found significant.
A significant correlation was found between the CBI total mean scores of the caregivers and their gender (t=3.03, p=0.00, p<0.05), their educational status (F=7.25, p=0.03, p<0.05), their need for human assistance (t=0.96, p=0.01, p<0.05), and their status of getting information about ALS (t=1.86, p=0.05, p<0.05).
The relationship among the caregivers’ ADL and DUKE scale total mean scores, their number of kids, their educational status, their social security, their marital status, their professions, where they live, their degree of relationship to the patient, the status of their chronic diseases that affect the treatment, and their need for human assistance was found at the α=0.05 level of significance.
Discussion
The fact that the patients are cared for by their family members makes them feel physically and psychologically better. However, the studies done indicate that caregivers meet some problems while giving care. It is especially highlighted that an old caregiver, his/her social status, and lack of social support may increase this risk. In a study realized by Navaie-Waliser et al. [13] it was found that 36.0% of the caregivers had difficulty in giving care. It was stated that these people gave care for 20 hours or more a week, they had difficulty in giving care, 1/3 of them had a physical health problem after being a caregiver, they offered a more intensive care, they were above 65, and 4/5 of them did not get any help while giving care. The findings of this study accord with the findings of ours. 40.0% of the caregivers who participated in our study stated that they had been giving care for more than 3 years. 93.3% of the caregivers stated that they did not get help from other family members while giving care, and 30.0% said that they cared for their patients for more than 13 hours a day. The difficulties caregivers face makes them suffer from social, physical, mental and economic problems. Especially the restriction of freedom of the caregivers who give care at home affects their state of mind negatively and leads them to suffer from depression [3,14].
In a study on ALS patients and caregivers that was realized by Gaiuthier et al.[24] male patients consisted of 67.7% of the ALS patients. It is determined by comprehensive clinical researches that this disease occurs more frequently in men than women.
This rate ranges from 2.1 to 1.5. [10].It is stated in a study on the care-burden of caregivers of ALS patients that was realized by Chio et al. [25] the patients who participated in the study had been diagnosed with ALS on average for 2-3 years. The results of these studies are consistent with the results of our study.
Ninety percent of the caregivers who participated in the study were female and 60.0% were the spouse of the patient. These data are consistent with the data of the research below. To illustrate, 63.5% of the caregivers were women in a study which was done by Chio et al. [25] on the care-burden of caregivers of ALS patients. In a study done by Gaiuthier et al. [24] on ALS patients and their caregivers, 71.0% of the caregivers were men. It was determined in a study realized by Dramal? et al.[26] that 89.0 % of the caregivers were women, 56.0% were the spouse of the patient, and 84% did not get any education or information about home care for their patients. 76% of the caregivers stated that they did not spare enough time for themselves and this situation afflicted their family lives and social lives [26]. It was determined in Altun et al.[27] study that 78.03% of the caregivers were women, 64.39% were housewives, and 34.85% took responsibility for the care of their spouse. It was also stated that 74.24% of the caregivers generally needed professional help about giving care, and 68.94% were concerned about their patients [27]. 36.7% of the caregivers who participated in the study stated that they did not get any information about ALS disease, they met some problems while giving care, and they needed education about care.
Conclusion
The quality of life of individuals with ALS is low and it was observed that they have difficulty in fulfilling their ADL. Furthermore, it was found that the training given on the subjects of patient care for which a need felt by caregivers was decrease the high burden. In accordance with these findings, decreasing the burden of caregivers for ALS patients will increase the participation of patients in ADL and strengthens the result that will raise the quality of life. Consequently, it can be proposed that studies should be made to reveal how a change in the burden of caregivers after education affects the quality of life of patients. With the results of this study, it is possible to suggest that standard education programs can be composed and that social activity programs for ALS patients and their relatives can be generalised.
Acknowledgements
The authors gratefully acknowledge the ALS patients, their families, and their caregivers, who made this study possible. We would like to thank ?hsan ?engün for his contributions and Ege University Science and Technology Centre (EB?LTEM) for supporting our project.
6878
References
- Dubendorf P (2010) Amyotrophic Lateral Sclerosis. Brunner&Suddarth’s Textbook Of Medical-Surgigal Nursing. Assessmentand Management of Clinical Problems. (12th edn), Lippincott Williams &Wilkins, Philadelphia.
- Bayramova N, Karadakovan A (2004) Hopelessness status of persons with chronical diseases.Ataturk UniversityJournalof Nursing 7: 39-48.
- McLeod JE, Clarke DM (2007) A review of psychosocial aspects of motor neurone disease. J Neurol Sci 258: 4-10.
- O’Brien M (2011) Management of Patients with Motor Neurone Disease. Neuroscience Nursing Evidence-Based Practice. (1st edn), Wiley-Blackwell Publication, Philadelphia
- Karadakovan A (2011) Degenerative and oncological diseases of the nervous system: Amyotrophic Lateral Sclerosis (ALS). Medical and SurgicalDiseasesCare. (2nd edn), Nobel Publications.
- Deeken JF, Taylor KL, Mangan P, Yabroff KR, Ingham JM (2003) Care for the caregivers: a review of self-report instruments developed to measure the burden, needs, and quality of life of informal caregivers. J Pain Symptom Manage 26: 922-953.
- Armon C (2001) Environmental risk factors for amyotrophic lateral sclerosis. Neuroepidemiology 20: 2-6.
- Carpenito-Moyet (2009) Handbook of Nursing Diagnosis. (13th edn), Lippincott Williams & Wilkins.
- Mitchell JD, Borasio GD (2007) Amyotrophic lateral sclerosis. Lancet 369: 2031-2041.
- Black JM, Matarassarin-Jacobs E (2010) Neurologic Disorders: Amytrophic Lateral Sclerosis. Luckmann and Sorenson’s Medical Surgical Nursing: A Psychophysiolojik Approach. (4th edn), W.B. Saunders. US.
- Haverkamp L, Appel V, Appel SH (1995) Natural history of amyotrophic lateral sclerosis in a database population. Validation of a scoring system and a model for survival prediction. Brain 118: 707-709
- Logroscino G, Traynor BJ, Hardiman O, Chio' A, Couratier P, et al. (2008) Descriptive epidemiology of amyotrophic lateral sclerosis: new evidence and unsolved issues. J Neurol Neurosurg Psychiatry 79: 6-11.
- Navaie-Waliser M, Feldman PH, Gould DA, Levine C, Kuerbis AN, et al. (2002) When the caregiver needs care: the plight of vulnerable caregivers. Am J Public Health 92: 409-413.
- Oliver D (2002) Palliative care for motor neurone disease. Pract Neurol 2: 68-79
- Oliver D, Borasio GD (2004) Palliative care for patients with MND/ALS. Eur J Palliat Care 11: 185-187
- Birol L (2004) Nursing Process: A Systematic Approachin Nursing Care. (6th edn), Etki Publishing.
- Kuzu N, Zencir M, Beser N, Sahiner T, Parkerson George RJ (2004) Reliability and valididity of the duke health profile. Journal ofHacettepeUniversity School of Nursing 2: 35-44.
- Parkerson GR Jr, Broadhead WE, Tse CK (1990) The Duke Health Profile. A 17-item measure of health and dysfunction. Med Care 28: 1056-1072.
- Novak M, Guest C (1989) Application of a multidimensional caregiver burden inventory. Gerontologist 29: 798-803.
- Luniewski M, Reigle J, White B (1999) Card sort: an assessment tool for the educational needs of patients with heart failure. Am J Crit Care 8: 297-302.
- Katz N, Krapin H, Lak A, Furman T (2003) Participation in occupational performance: reability and validity of the activity card sort. Participation and Health 23: 10-17.
- Deibel K, Anderson R, Anderson R (2005) Using edit distance to analyze card sorts. Expert Systems. 22: 129-138
- Küçükgüçlü Ö (2004) The reliability and validity of the caregiver burden inventory in Turkey. Ege University Institute of Health Sciencess Doctoral Thesis.
- Gauthier A, Vignola A, Calvo A, Cavallo E, Moglia C, et al. (2007) A longitudinal study on quality of life and depression in ALS patient-caregiver couples. Neurology 68: 923-926.
- Chiò A, Gauthier A, Calvo A, Ghiglione P, Mutani R (2005) Caregiver burden and patients' perception of being a burden in ALS. Neurology 64: 1780-1782.
- Dramali A, Demir F, Yavuz M (1998) The strain state of caregivers relatives of patients with chronic problems in the home care. I.NationalHome Health CareCongressAbstract Book. Istanbul.
- Altun I (1998) Strain state in the role of caregiver relatives of patients I.NationalHome Health CareCongressAbstract Book. Istanbul.

