Rajul Rastogi1*, GL Meena2, Yuktika Gupta1, Asif Majid Wani1, Pawan Joon1, Vijai Pratap1
1Department of Radiodiagnosis, Teerthanker Mahaveer Medical College and Research Center, Moradabad, Uttar Pradesh, India
2Department of Radiodiagnisis, Sardar Patel Medical College & PBM Hospital, Bikaner, Rajasthan, India
*Corresponding Author:
Rajul Rastogi
Department of Radiodiagnosis, Teerthanker Mahaveer Medical College and Research Center
Moradabad, Uttar Pradesh
India
Tel: 919319942162
E-mail: eesharastogi@gmail.com
Received date: February 20, 2016; Accepted date: February 28, 2016, Published date: March 03, 2016
Citation: Rastogi R, Meena GL, Gupta Y, et al. Imaging of Elastofibroma: A Rare Forgotten Tumor of Chest Wall. 2016, 4:1.
Keywords
Elastofibroma, computed tomography
Introduction
Soft tissue tumors of the chest wall including elastofibroma [also known as elastofibroma dorsi] are rare [1]. Elastofibroma is most frequently encountered in middle aged to elderly females in infrascapular location, more commonly on right side but may be bilateral. As imaging and microscopy [FNAC or biopsy] can achieve the diagnosis in majority of cases, hence surgical intervention should be reserved for symptomatic cases [1,2].
Case Report
A 25 years old male presented to us with complaint of soft tissue swelling and pain in right infrascapular region. Local examination revealed palpable soft tissue mass with freely mobile overlying skin and slight pain only on performing scapular movements. No evidence of any other external abnormality or tenderness was noted. Laboratory examination, chest radiograph and ultrasonography (USG) of abdomen were unremarkable. However, high resolution USG of the mass revealed predominantly solidappearing, fairly-defined, smooth-marginated, echogenic mass interspersed with some linear hypoechoic areas. No evidence of any internal calcification or frank necrosis was noted.
Contrast-enhanced, computed tomography (CT) scan of the thorax revealed a nonenhancing, soft-tissue attenuating, solid mass lesion along the posterolateral aspect of right thoracic wall in infrascapular location (Figure 1). The tumor was lying between the chest wall and serratus anterior and latissimus dorsi muscles. The tumor revealed hypodense internal areas of fat attenuation (Figure 2). The lesion measured approximately up to 13.5*8.0*6.5 mm corresponding to approximately up to 350-400 ml in volume. However, no evidence of any obvious internal calcification or necrosis was noted. No evidence of any obvious adjacent osseous involvement or intrathoracic extension was noted.
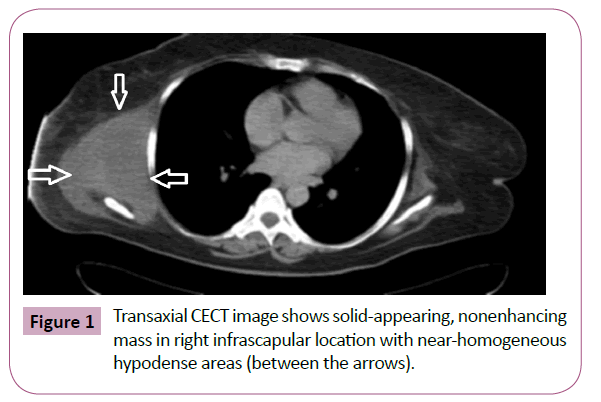
Figure 1: Transaxial CECT image shows solid-appearing, nonenhancing mass in right infrascapular location with near-homogeneous hypodense areas (between the arrows).
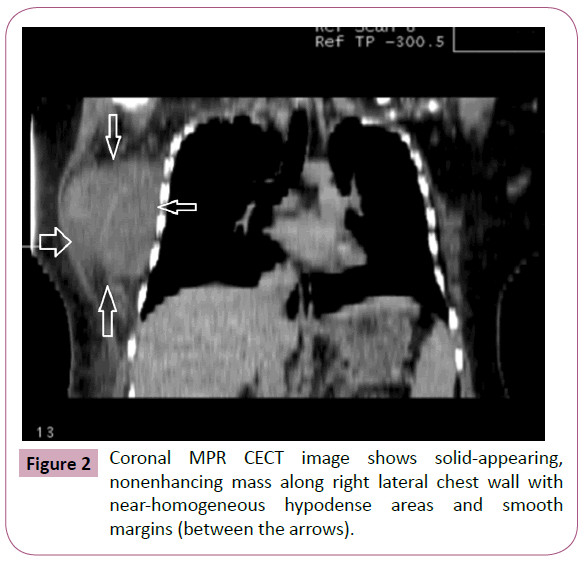
Figure 2: Coronal MPR CECT image shows solid-appearing, nonenhancing mass along right lateral chest wall with near-homogeneous hypodense areas and smooth margins (between the arrows).
Based on the clinicoradiologic findings, the diagnosis of elastofibroma of chest wall was suggested and follow up was suggested. Six months follow up of patient did not reveal any significant change in the clinical symptoms, clinical appearance and size of the tumor. However, as the patient was apprehensive, hence open biopsy was planned to exclude the sarcomatous lesion and to reassure the patient, that surgical excision is not indicated (Figure 3).
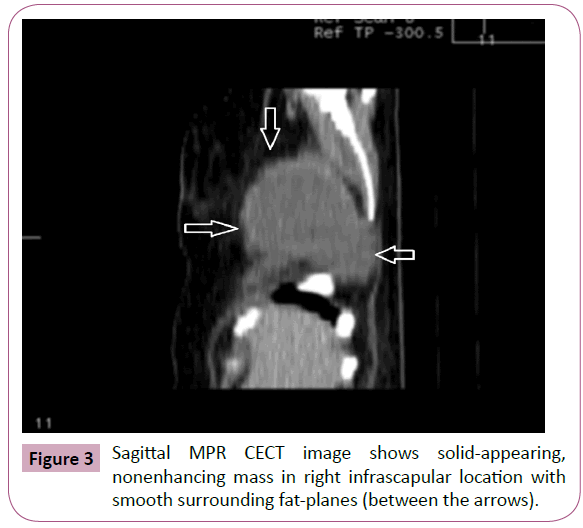
Figure 3: Sagittal MPR CECT image shows solid-appearing, nonenhancing mass in right infrascapular location with smooth surrounding fat-planes (between the arrows).
Histopathology revealed fibrous tissue containing clusters of elastin and collagen fibers interspersed with fatty areas confirming the diagnosis of elastofibroma (Figure 4).
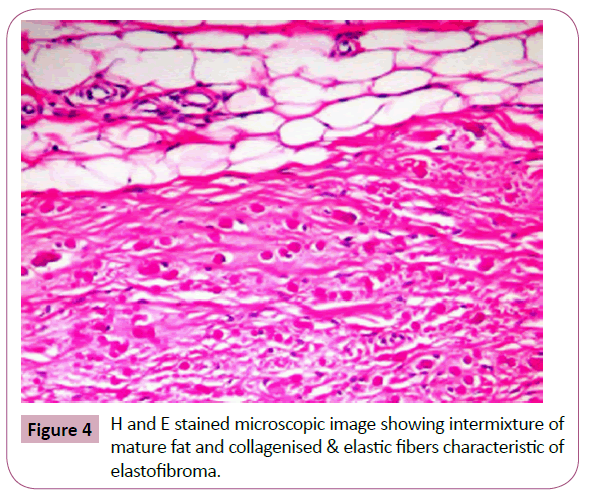
Figure 4: H and E stained microscopic image showing intermixture of mature fat and collagenised & elastic fibers characteristic of elastofibroma.
Discussion
Elastofibroma is a rare, benign tumor of chest wall arising from the connective tissues of dermis, occurring commonly in elderly females. It was first reported by Jarvi and Saxen in 1959. Majority of them are bilateral while in unilateral cases, right side is commoner than left side. The characteristic location is infrascapular or subscapular regions between the serratus anterior, rhomboid & latissimus dorsi muscles and chest wall. Uncommonly, the tumor may occur in the deltoid muscle and region of ischial tuberosity, greater trochanter, olecranon process of ulna, foot and mediastinum [3]. The tumor grows very slowly and is more prevalent in persons involved in manual labor involving hands and arms.
Though the etiology is unknown yet it is considered by some to represent a reactive process or a fibroblastic pseudotumor as it is characterized by accumulation of abnormal elastin fibers [4]. An abnormal gene on chromosome 1 and 2 has been described attributing some of the lesions as genetic [5].
Majority of patients are asymptomatic with few of them being palpable initially. When large, they are associated with clicking/ snapping sensation or pain during scapular movement. Rarely, it may involve the overlying skin which may ulcerate [6].
Imaging features are characteristic with high-resolution ultrasonography showing solid, echogenic, well-defined, fibroelastic tissue interspersed with multiple, hypoechoic, linear areas of fatty tissue without internal necrosis or calcification or vascularity on color Doppler imaging [7]. Computed tomography (CT) scans show fairly-defined, nonenhancing or minimallyenhancing, mass often lentiform or semilunar-shaped, appearing isodense to adjacent muscles in characteristic infrascapular or subscapular location that shows internal linear hypodensities of fatty attenuation [7,8]. No evidence of any obvious sign of internal necrosis or calcification is noted. They are rarely attached to the underlying periosteum.
Magnetic resonance imaging (MRI) shows non-capsulated, solid mass in characteristic location appearing isointense to adjacent muscles on T1W and T2W images showing internal linear hyperintensities corresponding to fat on both T1W and T2W images without obvious restriction on DW images. No evidence of any obvious internal calcification or necrosis is noted. Post-Gadolinium images show mild, near-homogeneous enhancement [7-9].
FDG PET-CT shows uptake on tracer allowing incidental detection of clinically silent small elastofibroma [10]. No evidence of malignant transformation has been described in the literature.
Few cases of elastofibroma have been described in literature with majority of them in elderly females unlike our index case in young male [11].
Histopathological diagnosis is needed in equivocal cases or when the patient is highly-apprehensive of cancer by performing a surgically biopsy. It reveals tumor-like masses of collagen and elastin fibers with scattered areas of fat on microscopy. Complete excision of the tumor is indicated in symptomatic and equivocal cases.
Differential diagnoses that need to be considered in the characteristic location of elastofibroma include lipoma, fibromatosis, sarcoma and metastases. Lipoma is an encapsulated lesion showing homogeneous internal fat without obvious postcontrast enhancement. Fibromatosis appears as solid, soft-tissue tumor with irregular margins without internal striations or fat and showing mild to moderate postcontrast enhancement. Sarcoma is fast-growing, infiltrative tumor showing moderate to intense postcontrast enhancement and internal necrosis with invasion/destruction of adjacent structures. Confident diagnosis of metastases requires a known primary tumor.
To summarize, elastofibroma is a rare, benign, soft tissue tumor of chest wall that can be confidently diagnosed on imaging obviating the need for excision biopsy or major surgery in asymptomatic patients. Small elastofibroma may be incidentally detected on PET-CT where they need differentiation from metastases.
8735
References
- Freixinet J, Rodriguez PM, Hussein M, Sanroman B, Herrero J, et al. (2008) Elastofibroma of chest wall. Interactive CardioVascular and Thoracic Surgery.
- DaigelerA, VogtPM, BuschK (2007) Elastofibromadorsi-differential diagnosis in chest wall tumours. World Journal of Surgical Oncology 5:15.
- DeNictolis M, Goteri G, Campanati G, Prat J (1995) Elastofibrolipoma of the mediastinum. A previously undescribed benign tumor containing abnormal elastic fibers. Am J Surg Pathol 19: 364-367.
- Shimizu S (2004) Multiple elastofibroma. J Am Acad Dermatol 50:126-129.
- Nishio JN (2002) Gain of Xq detected by comparative genomic hybridization in elastofibroma. Int J Mol Med 10: 277-280.
- Schwarz T, Oppolzer G, Duschet P, Brückler B, Gschnait F (1989) Ulcerating elastofibromadorsi. J Am Acad Dermatol 21: 1142-1144.
- Ozpolat B, Yazkan R, Yilmazer D, Kocak N, Yucel E (2008) Elastofibromadorsi-report of a case with diagnostic features. J Ultrasound Med 27: 287-291.
- Valls R, Melloni P, Darnell A, Sanchez-Flo R (1996) Elastofibromadorsi: a chest wall pseudotumor. Computed tomography and magnetic resonance imaging diagnosis. Acta Orthop Belg 62: 103-106.
- Alouini R (2005) Elastofibroma: imaging features. J Radiol 86: 1712-1715.
- Wasyliw CW, Caride VJ (2005) Incidental detection of bilateral elastofibromadorsi with F-18 FDG PET/CT. Clin Nucl Med 30: 700-701.
- HaykirR, Karakose S, Karabacakoglu A (2007) Elastrofibromadorsi: Typical radiological features. Australasian Radiology 51: 95-97.


