Spyropoulos P.1*, Armstrong C.2, Chronopoulos E.3, Kwiatkowski B.4, Babatsikou F.5
1PhD, MS, PT, Associate Professor, Technological Educational Institute of Athens, School of Physical Therapy, Athens, Greece
2PhD, MS, Professor, University of Toledo, Department of Kinesiology
3MD, PhD, PT, Lecturer, University of Athens, Medical School, Department of Orthopaedics
4PhD, MS, Electronic Technologist I, University of Toledo, Department of Kinesiology
5MD, PhD, MS, RN, Assistant Professor, Technological Educational Institute of Athens, Department of Nursing A?, Athens, Greece
*Corresponding Author:
Dr. Panagiotis Spyropoulos
Address: 36-B Pliadon Street
Kifisia, Athens 14561
Greece
Keywords
Osteoarthritis · Walking · Accelerometer · Shock Attenuation · Impact Loading
Introduction
Osteoarthritis is the most prevalent type of rheumatic diseases affecting 21 million Americans [1]. Osteoarthritis is chronic and involves mostly weight bearing joints such as hips, knees, feet and spine. Specifically, the cartilage of joints degenerates and inflammation may develop in all periarticular and intra-articular tissues. Finally, degeneration develops in joint capsules, tendons, ligaments, fasciae and muscles. Frequently, limitation of various movements occurs, which, in turn, causes weakness of muscles, development of contractures and distortion of correct posture [2-5].
Despite the efforts of medical sciences, there is no knowh cure of osteoarthritis. Today, the treatment includes the use of assisstive devices to protect the afflicted joints, weight control, medication, surgery, application of heat or cold over the painful joints and exercises. The goal is to decrease pain and maintain functional activities by preserving or improving strength and muscular endurance [6-12].
Recently, progressive physicians recommend exercise programs for osteoarthric patients [13,14]. Exercise booklets have been prepared by the Arthritis Foundation, providing instruction for active range of motion of different joints. Although these exercises maintain mobility of joints, they improve muscular strength and endurance only minimally [15,16]. In addition, they fail to promote functional activities, tend to become boring and as a result, they are often abandoned. Perhaps, exercise activities such as slow or fast walking could enrich a therapeutic program, promote functional ability and improve cardiovascular denefits in osteoarthritic patients. However, there is scarse research upon which to base recommendations for involvement in programs of therapeutic walking [17,18]. Little is known about the effects of such factors as variation in walking speed and terrain on osteoarthritis. It is conceivable that these factors may influence the levels of musculoskeletal loading, and, thus, further accelerate the progress of the disease. Therefore, the purpose of this study was to investigate the levels of loading in healthy and osteoarthritic women during various conditions of walking.
MATERIAL AND METHOD
Subjects
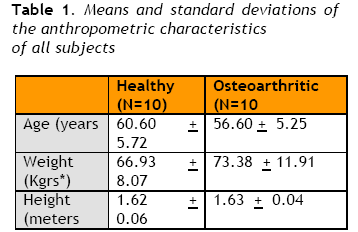
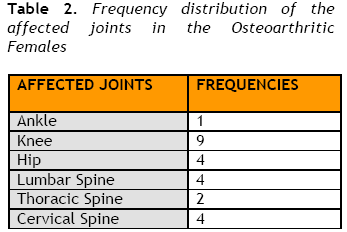
Two groups, each consisting of ten subjects, were chosen for this investigation. One group was comprised of individuals who were healthy, and the other was consisted of those with documented osteoarthritis of the lower extremities and/or spine. All participants were volunteers, middle-aged females of average height and weight (Table 1), referred by local rheumatologists, or recruited from exercise classes at the University of Toledo, South Toledo YMCA, St. Vincet’s Hospital and Flower Hospital. A frequency distribution of the affected joints in the osteoarthritic individuals is reported in Table 2
Each individual was screened through the use of a questionnaire to exclude any diagnosed cardiovascular, neurological or acute othopaedic conditions that might have affected her gait. A typewritten handout was delivered to each subject explaining the procedure, as well as the risks and benefits resulting from the study. An informed consent section was included in the handout that each participant signed prior to testing. The study was approved by the Human Subjects Committee of the University of Toledo and supported by a research grant provided by the Applied Biomechanics Laboratory of the University of Toledo.
Instrumentation
All individuals wore shorts and shirts but no shoes during all experimental conditions. A safety belt was attached to each subject’s waist while walking on a motor-driven treadmill (Cambridge, Model 3050). A low mass accelerometer (Endevco, 7265A Model), encased in balsa wood, was secured via a velcro strap to the left tibial tubercle of each subject. The balsa wood provided protection for the instrument, enabled consistent anatomical placement and minimized movement of the accelerometer. During testing, the accelerometer was connected to a computer system and data were collected and analyzed at a sampling rate of 500 Hz.
Testing Protocol
Each person appeared at the Biomechanics Laboratory of the University of Toledo once for approximately one and a half hour of which 30 minutes were the total practice and testing periods of time. The remaining time was devoted to subject preparation and resting, as well as calibration of testing equipment and alteration of experimental conditions.
Each subject walked on the treadmill at grades 0° (level), +6° (uphill) and -6° (downhill) and at speeds of 1.5 and 2.5 miles per hour while having an accelerometer attached to the left tibial tuberosity and later to the middle of the forehead. These speeds were chosen based on pilot work, and represented slow and fast walking for our groups of middle-aged women. There were 12 experimental conditions randomly assigned (2 speeds x 3 grades x 2 accelerometer placements) for each individual. Prior to each trial, a practice period of 30 seconds to one minute was provided for each person to become familiar with the degree of elevation and speed of treadmill. Following this, the accelerometer data were collected during walking for a period of 100 to 110 seconds during each experimental condition.
Experimental Design and Statistical Analysis
The experimental design was a three factorial mixed design. There were two within subjects factors (repeated measures) and one between subjects factor. The first factor (between subjects) was the type of health status (osteoarthritic and healthy). The second factor (within subjects) referred to the elevation of the readmill ( 0° ,+6° , and -6°). The third factor (within subjects) involved the speed of the treadmill (1.5 and 2.5 miles per hour.
The evaluation of the recorded deceleration signal involved calculation of the peak deceleration (shock) characteristics resulted from ground contact. The statistical analysis included a 2x3x2 ANOVA with the Tukey post-hoc test once significant differences were detected. The dependent variables were the peak deceleration at tibia and forehead, expressed in g units.
RESULTS
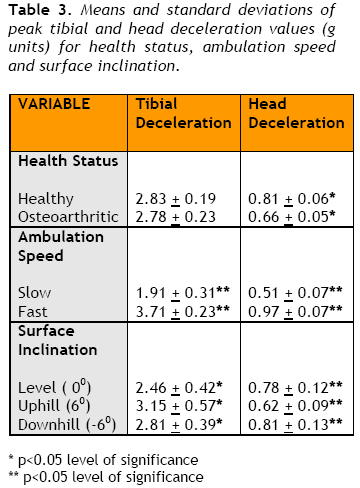
Table 3 shows the mean peak shank deceleration values for healthy and osteoarthritic women, for all subjects between fast and slow speeds and for all participants among level, uphill and downhill walking. Healthy and osteoarthritic women had similar peak shank values. Fast walking produced 95% higher peak shank deceleration whereas during uphill and downhill ambulation the peak shank deceleration values were respectively 22% and 12.5% higher than level walking.
A summary of the three-way ANOVA for peak shank deceleration with level of significance set at p=0.05 is shown in Table 4. The main effects of speed, grade of ambulation and speed by grade interaction were statistically significant (p<0.05 and p<0.01).
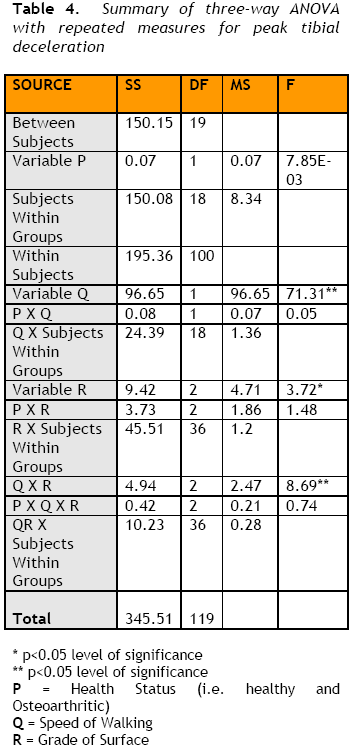
Table 3 also shows the mean peak head deceleration values for healthy and osteoarthritic women, for all subjects between fast and slow speeds and for all participants among level, uphill and downhill walking. Healthy women had 18.2% higher peak head deceleration values than osteoarthritic women. Fast walking produced 47.8% higher peak head deceleration than slow walking whereas during uphill and downhill ambulation the peak head deceleration values were respectively 11.2% lower and 3.4% higher than level walking.
A summary of the three-way ANOVA for peak head deceleration with level of significance set at p=0.05 is shown in Table 5. The main effects of health status, speed, grade of ambulation and speed by grade interaction were statistically significant (p<0.05 and p<0.01).

DISCUSSION
This study investigated the influence of varying walking conditions on shock generation and absorption characteristics of middle-aged women who were healthy or diagnosed as osteoarthrics but their symptoms were not severe to be considered candidates for surgery.
Data, collected via accelerometry, have indicated that both group of subjects collectively presented similar values of peak tibial deceleration during ambulation.
Specifically, the healthy persons had an average peak tibial value of 2.8304 g whereas the osteoarthritic individuals displayed similar mean peak tibial value of 2.7837 g. These results are in accordance to those reported in related literature [19-21] and were expected because the anatomic units of foot and shank will absorb approximately the same amount of ground reaction forces unless a pathology is present in these structures, or unless the velocities of the foot and shank in both groups are unequal at ground contact. Both of the tested groups had about the same mean weight (Table 1), and no considerable pathological deformities in their feet and/or shanks (Table 2). Although the velocities of the foot and shank at ground contact were not calculated, based on the fact that both groups were tested at the same walking speeds, it is speculated that these velocities were probably equal for both groups. Thus, the ground reaction forces produced nearly the same magnitude of shock once transmitted to the tibial tuberosity. Indeed, the three-way ANOVA, in Table 4, statistically confirmed the similarity of tibial peak deceleration of both groups (p>0.05).
Results of mean peak head deceleration revealed that there were statistically lower values (p<0.05) in osteoarthritic women than in healthy individuals. Apparently, kinematic adjustments occurring in the spine and/or pelvis of osteoarthric females [22] as well as muscle function [23-25] may have accounted for the greater absorbed deceleration values although the present study has not examined kinematic or EMG parameters in both groups. Nevertheless, the recorded peak shock head values agree with those reported in scientific related literature [26,21,27].
Regarding walking speed, it was demonstrated that slow walking produced statistically lower (p<0.01) tibial (1.9096 g) and head deceleration (0.5050 g) than fast walking (3.7044 g and 0.9677 g respectively). The outcome of these results was expected since fast walking always generates greater ground reaction forces than slow walking [28]. Similar results in related literature concerning impact loading at shank and head sites are also reported by other investigators [29-32].
The effect of walking surface slopes on deceleration characteristics was also examined in this study. It was reported that peak shank deceleration values were significantly lower (p<0.05) at level grade (2.4617 g) than those recorded during uphill (3.1478 g) and downhill (2.8116 g) walking. In contrast, significantly lower peak head deceleration values (p<0.01) were observed during uphill walking (0.6165 g) than those recorded during level (0.7823 g) and downhill (0.8102 g) walking. By subtracting the results in the three grades of ambulation between the sites of shank and head, it was clearly shown that the highest values of shock generation and attenuation was recorded during uphill walking (2.5313 g) whereas shock absorbed in downhill and level walking was 2.1014 g and 1.6794 g respectively. These findings are in accordance to those reported in scientific related literature regarding slope of walking surface30,33. Therefore, it is safe to recommend level walking to middle-aged osteoarthritic women as a mode of exercising because it produces the least stress and loads the musculoskeletal system minimally.
CONCLUSIONS
Based on the results of the study following conclusions were drawn:
1. Tibial peak deceleration is the same for the healthy and osteoarthritic females.
2. Osteoarthritics exhibit lower values of pek head deceleration than healthy women. Kinematic adjustments may contribute to these findings.
3. Slow walking is less stressful than fast walking in middle-aged females. Thus, slow walking is highly recommended in patients suffering grom osteoarthritis.
4. Level walking produces the least loading on the human locomotor system. Uphill walking generates the highst impact forces in elderly women and thus, it should be avoided.
ACKNOWLEDGEMENTS
This study was supported by a research grant of the Applied Biomechanics Laboratory of the University of Toledo. The authors wish to express their gratitude to all referring physicians.
Conflict of interest
The authors declare that they have no conflict of interest
3674
References
- Eyigor S, Hepguler S, Capaci K. A comparison of muscle training methods in patients with knee osteoarthritis. Clin Rheumatol 2004;23(2):109-15.
- Sharma L, Cahue S, Song J, Hayes K, Pai YC, Dunlop D. Physical functioning over three years in knee osteoarthritis: role of psychosocial, local mechanical, and neuromuscular factors. Arthritis Rheum 2003;48(12):3359-70.
- Gür H, Cakin N. Muscle mass, isokinetic torque, and functional capacity in women with osteoarthritis of the knee. Arch Phys Med Rehabil 2003;84(10):1534-41.
- Jones P, Alexander CJ, Stewart J, Lynskey N. Idiopathic osteoarthritis and contracture: causal implications. Ann Rheum Dis 2005;64(2):226-8.
- Mikesky AE, Mazzuca SA, Brandt KD, Perkins SM, Damush T, Lane KA. Effects of strength training on the incidence and progression of knee osteoarthritis. Arthritis Rheum 2006;55(5):690-9.
- Hendry M, Williams NH, Markland D, Wilkinson C, Maddison P. Why should we exercise when our knees hurt? A qualitative study of primary care patients with osteoarthritis of the knee. Fam Pract 2006;23(5):558-67.
- Shrier I, Feldman DE, Gaudet MC, et al. Conservative non-pharmacological treatment options are not frequently used in the management of hip osteoarthritis. J Sci Med Sport 2006;9(1-2):81-6.
- Van Gool CH, Penninx BW, Kempen GI, et al. Determinants of high and low attendance to diet and exercise interventions among overweight and obese older adults. Results from the arthritis, diet, and activity promotion trial. Contemp Clin Trials 2006;27(3):227-37.
- Deyle GD, Allison SC, Matekel RL, Ryder MG, Stang JM, Gohdes DD, Hutton JP, Henderson NE, Garber MB. Physical therapy treatment effectiveness for osteoarthritis of the knee: a randomized comparison of supervised clinical exercise and manual therapy procedures versus a home exercise program. Phys Ther 2005; 85(12):1301-17.
- Messier SP, Gutekunst DJ, Davis C, DeVita P. Weight loss reduces knee-joint loads in overweight and obese older adults with knee osteoarthritis. Arthritis Rheum 2005;52(7):2026-32.
- Quilty B, Tucker M, Campbell R, Dieppe P. Physiotherapy, including quadriceps exercises and patellar taping, for knee osteoarthritis with predominant patello-femoral joint involvement: randomized controlled trial. J Rheumatol 2003; 30(6):1311-7.
- Diracoglu D, Aydin R, Baskent A, Celik A. Effects of kinesthesia and balance exercises in knee osteoarthritis. J Clin Rheumatol 2005;11(6):303-10.
- Roos EM, Dahlberg L. Positive effects of moderate exercise on glycosaminoglycan content in knee cartilage: a four-month, randomized, controlled trial in patients at risk of osteoarthritis. Arthritis Rheum 2005; 52(11):3507-14.
- Halbert J, Crotty M, Weller D, Ahern M, Silagy C. Primary care-based physical activity programs: effectiveness in sedentary older patients with osteoarthritis symptoms. Arthritis Rheum 2001;45(3):228-34.
- O'Grady M, Fletcher J, Ortiz S. Therapeutic and physical fitness exercise prescription for older adults with joint disease: an evidence-based approach. Rheum Dis Clin North Am 2000;26(3):617-46.
- Chen CP, Chen MJ, Pei YC, Lew HL, Wong PY, Tang SF. Sagittal plane loading response during gait in different age groups and in people with knee osteoarthritis. Am J Phys Med Rehabil 2003;82(4):307-12.
- Kaufman KR, Hughes C, Morrey BF, Morrey M, An KN.Gait characteristics of patients with knee osteoarthritis. J Biomech 2001;34(7):907-15.
- Henriksen M, Simonsen EB, Graven-Nielsen T, Lund H, Danneskiold-Samsøe B, Bliddal H. Impulse-forces during walking are not increased in patients with knee osteoarthritis. Acta Orthop 2006;77(4):650-6.
- Liikavainio T, Isolehto J, Helminen HJ, et al. Loading and gait symmetry during level and stair walking in asymptomatic subjects with knee osteoarthritis: importance of quadriceps femoris in reducing impact force during heel strike? Knee 2007;14(3):231-8.
- Nigg BM. Loads in selected sport activities – An overview. In International Series on Biomechanics: Biomechanics IX-B, Winter DA, Norman RW, Wells, RP, Hayes KC and Palta AE, editors. Champain Ill: Human Kinetics Publishers, Inc., pp. 91-96, 1985.
- Helliwell PS, Smeathers JE, Wright V. Shock absorption by the spinal column in normals and in ankylosing spondylitis. Proc Inst Mech Eng [H]. 1989;203(4):187-90.
- Hortobágyi T, Westerkamp L, Beam S, et al. Altered hamstring-quadriceps muscle balance in patients with knee osteoarthritis. Clin Biomech 2005;20(1):97-104.
- Clancy EA, Cairns KD, Riley PO, Meister M, Kerrigan DC. Effects of treadmill walking speed on lateral gastrocnemius muscle firing. Am J Phys Med Rehabil 2004;83(7):507-14.
- Den Otter AR, Geurts AC, Mulder T, Duysens J. Speed related changes in muscle activity from normal to very slow walking speeds. Gait Posture 2004;19(3):270-8.
- Voloshin A, Wosk J, Brull M. Force wave transmission through the human locomotor system. J Biomech Eng 1981;103(1):48-50.
- Wosk J, Voloshin A. Wave attenuation in skeletons of young healthy persons. J Biomech 1981;14(4):261-7.
- Cavanagh, PR, Lafortune MA. Ground reaction forces in distance running. J Biomech 1980 13:397-406.
- Voloshin A. The influence of walking speed on dynamic loading on the human musculoskeletal system. Med Sci Sports Exerc 2000;32(6):1156-9.
- Schwameder H, Lindenhofer E, Müller E. Effect of walking speed on lower extremity joint loading in graded ramp walking. Sports Biomech 2005;4(2):227-43.
- Cheng CK, Chen HH, Chen CS, Lee SJ. Influences of walking speed change on the lumbosacral joint force distribution. Biomed Mater Engb1998;8(3-4):155-165.
- Holt KG, Wagenaar RC, Kubo M, LaFiandra ME, Obusek JP. Modulation of force transmission to the head while carrying a backpack load at different walking speeds. J Biomech 2005;38(8):1621-8.
- Kuster M, Sakurai S, Wood GA. Kinematic and kinetic comparison of downhill and level walking. Clin Biomech 1995;10(2):79-84.

