Keywords
CP; QOL; Psychosocial distress; Parent proxy
Introduction
A group of motor impairment syndromes that develops in the earlier stages of development second after to the anomalies of the brain, comes under the umbrella of cerebral palsy [1]. CP patients may have movement and posture disorders, and some of them may have intellectual disability, abnormality of sensations or perceptions, impaired vision and/or hearing, seizures, language and speech issues [2]. The low birth weight was the most common risk factor identified [3]. Maternal, fetal inflammatory response caused by intrauterine maternal infection was found to be associated with white matter injury and Cerebral Palsy [4].
Premature babies tend to have high levels of bilirubin, deprivation of oxygen, infections, trauma, ultimately leading to Cerebral Palsy [5]. Asphyxia at the time of birth causes hypoxia. This hypoxia leads to damage in brain cells causing abnormality and disorders [6]. In particular maternal genitourinary infections were correlated with high risk of CP with a low birth weight and preterm babies [7].
Rubella, chicken pox, toxoplasmosis, cytomegalovirus, syphilis, viral encephalitis and bacterial meningitis are infections especially included [8]. Twins have more tendencies to develop CP then singletons born babies. Low birth weight or be born prematurely are the main causes [9]. Incompatibility between A-B-O and Rh type can occur if there is a conflict between mother’s and her newborn child blood type. This incompatibility could exacerbate the risk of damage in brain and CP [10].
The clinical disorders result due to brain damage and can differ depending upon the level, nature and extent of injury. It has been found that 75 percent of the infants who died shortly after birth were premature and were periventricular leukomalacia cases. Severe impairments i.e. cognitive, neurodevelopmental and motor delays and epilepsy can be caused by encephalopathy due to hypoxia and ischemia. Intraventricular Haemorrhage leads to damage to the brain causing impairments [11].
Spastic (65 percent), athetoid (10 percent), ataxic (5 percent), mixed and hypotonic are different forms of motor abnormality based CP. Monoplegia, diplegia, hemiplegia, triplegia, quadriplegia and double hemiplegia are different forms based on a part of body being involved, according to anatomical findings [12]. Patients of cerebral palsy can’t be cured completely, but effective treatment can maintain and improvise the child's wellbeing and living standards. Physical therapy, if started earlier can produce more results and is a cornerstone for CP child treatment. It may enhance balance, motor skills, muscle strength and can avoid contracture. Different approaches are now being employed for better results in physical therapy [13]. The new ones focus more on lifestyle changes and increasing resources for generalized mobility [14].
As CP children have to face not only physical problems but also a variety of social and emotional issues. In order to assess the disability that develops the quality of life (QOL) has been captured by many researchers.
Various authors outline different definitions of quality of life. From a health QOL defines as ‘an evaluation of wellbeing between different areas of life [15]. A study of children with CP with their parents identified the important areas of life such as acceptance, participation, social well-being, emotional well-being, physical health, functioning feelings, access to services pain and distress, disability impact, and family health [16].
Aside from the illness other factors influence QOL’s proxy results. This could include the physical and mental health, temperament, motivation, coping, and self-esteem for the parent. Although there is insufficient research to assess the effect of these factors [17]. Researcher in this study was interested in evaluating the relation of parental psychosocial distress to quality of life reported by parents.
Materials and Methods
Study design: It was a Cross Sectional Study Design.
Settings: The settings used for data collection was Children Hospital and Pakistan Society for the Rehabilitation of Disabled (PSRD) Lahore.
Duration of study: After the approval of synopsis, three months was the time of completion of study.
Sampling technique: To obtain the sample Purposive Sampling was used.
Sample size: Sample size was of 131 patients. By using following formula Sample size was calculated
Sample Size = Z1-α ?2 P (1-P)/d2
and the level of significance was taken 8% [18].
Sample selection
Inclusion criteria: All the children having CP between the ages of 4- 12 years.
The parents of CP child included.
Exclusion criteria
Age <4 and >12 years of CP child comes under exclusion criteria. Children with neurological disorders other than CP Parents of those childs who do not have CP.
Data collection procedure
Quality of Life Questionnaire for Children (CP QOL-Child) for 4-12 years was used after taking consent from patients and their parents. It was a Primary Caregiver Questionnaire. Primary caregiver was described as the person who knew the most about the infant. In this research we took the parents as the primary care giver. The Kessler–10 (K-10) questionnaire was used for assessing psychosocial distress.
Data Collection Tools (Proforma/Questionnaire)
To collect the relevant information from the subjects, a welldesigned and detailed Questionnaire/Pro-forma was used.
Data analysis
Using the SPSS 17.0 statistical software data was analyzed. As was the estimation of cross sectional study frequencies of various domains of quality of life and frequency of psychosocial distress of parents was calculated. It also calculated Mean and Standard deviation. Bar charts were created for each QOL domain. In the form of mean ± standard deviation (S.D.), their cumulative score was then given.
Results
To analyze the data Statistical Analysis tools such as Mean, Standard Deviation, descriptive statistics, bar chart and pie chart were used.
The domain of family and friends: Table 1 shows that in the domain of family and friends 92 (70.2%) children were unhappy, 20 (15.3%) were neutral and 19 (14.5%) were happy. In the area of participation (Table 2) 100 (76.3%) were unhappy, 12 (9.2%) were neutral and 19 (14.5%) were happy out of 131.
| Variables |
Frequency |
Percent |
Valid Percent |
Cumulative Percent |
| Unhappy |
92 |
70.2 |
70.2 |
70.2 |
| Neutral |
20 |
15.3 |
15.3 |
85.5 |
| Happy |
19 |
14.5 |
14.5 |
100.0 |
| Total |
131 |
100.0 |
100.0 |
-- |
Table 1: Domain of family and friends.
| Variables |
Frequency |
Percent |
Valid Percent |
Cumulative Percent |
| Unhappy |
100 |
76.3 |
76.3 |
76.3 |
| Neutral |
12 |
9.2 |
9.2 |
85.5 |
| Happy |
19 |
14.5 |
14.5 |
100.0 |
| Total |
131 |
100.0 |
100.0 |
-- |
Table 2: Domain of participation.
In the area of communication: Table 3 shows that in the domain of communication 114 (87%) children were unhappy, 11 (8.4%) were neutral and 6 (4.6%) were happy.
| Variables |
Frequency |
Percent |
Valid Percent |
Cumulative Percent |
| Unhappy |
114 |
87.0 |
87.0 |
87.0 |
| Neutral |
11 |
8.4 |
8.4 |
95.4 |
| Happy |
6 |
4.6 |
4.6 |
100.0 |
| Total |
131 |
100.0 |
100.0 |
-- |
Table 3: Domain of communication.
In health domain, 101 (77.1%) were unhappy, 20 (15.3%) were neutral and 10 (7.6%) were happy. In the domain of special equipment, 127 (96.9%) were unhappy and 4 (3.1%) were neutral. In the area of pain and botherness, 24 (18.3%) were very bothered, 76 (58.0%) were not bothered and 31 (23.7%) were neutral. In the domain of access to services, 62 (47.3%) were unhappy 45 (34.4%) were neutral and 24 (18.3%) were happy.
Out of total 131 participants, 20 (15.3%) were in mild distress, 42 (32.1%) were in moderate distress, and 69 (52.7%) were in severe distress (Figure 1).
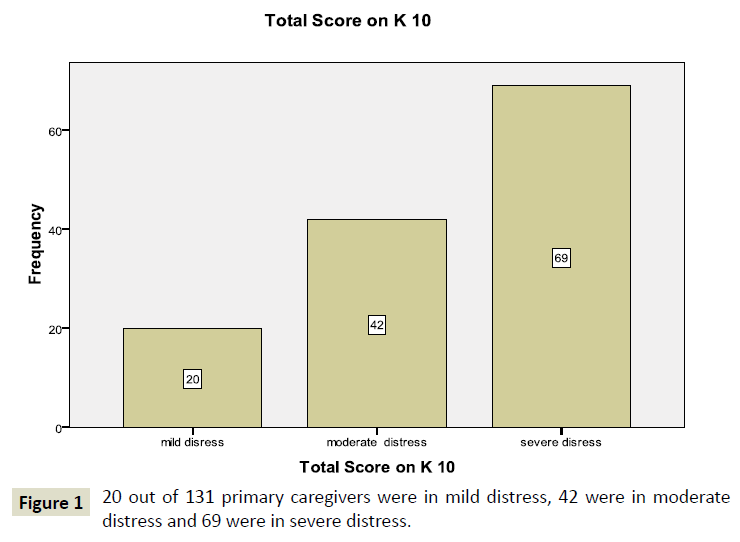
Figure 1: 20 out of 131 primary caregivers were in mild distress, 42 were in moderate distress and 69 were in severe distress.
Discussion
The aim of the research was to find the effect of parental psychosocial distress on quality of life reported by parent proxy in different domains. In this study, 20 (15.3%) of the total 131 parents were in mild distress, 42 (32.1%) were in moderate distress, and 69 (52.7%) were in severe distress. Because of this stress level the proxy recorded outcomes from the quality of life domains showed that most children were unhappy. The results of my research were very similar to a recent earlier study that identified the negative impact of parental distress on the QOL recorded from all proxy domains. This research also recommends that psychological state of parents should also be considered when using the parent proxy. This study was different from previous studies in a way that no researcher has seen the effect of psychosocial distress on all areas of QOL. Previous researches only describe the anxiety and depression effects but in this research both social and psychological aspect is considered. And the questionnaire used in this study was CP-QOL (4-12 years), whereas previously CHQ or HRQOL questionnaire was used on these kinds of studies.
Conclusion
This research concluded that quality of life domains i.e. Family and friends, Communication, Participation, Special Equipment, Health, Pain and Botherness, Access to services are highly influenced by parental psychosocial distress. This research also found that psychosocial parental distress was negatively correlated with QOL identified by the parent proxy.
It is recommended that, a longitudinal prospective study should be conducted on this issue as parents’ depression and psychosocial distress changes over time. And in this study information is only collected from primary caregivers whereas data should be collected from both parents i.e. both from primary and nonprimary care giver instead of only from primary caregivers for further researches.
39081
References
- Sankar C, Mundkur N (2005) Cerebral palsy-definition, classification, etiology and early diagnosis. The Indian Journal of Pediatrics 72: 865-868.
- Warschausky S, White D, Tubbergen M (2010) Cerebral palsy across the lifespan. Principles and Practice of Lifespan Developmental Neuropsychology 205-219.
- Suvanand S, Kapoor S, Reddaiah V, Singh U, Sundaram K (1997) Risk factors for cerebral palsy. The Indian Journal of Pediatrics 64: 677-685.
- Jacobsson B, Hagberg G (2004) Antenatal risk factors for cerebral palsy. Best Practice & Research Clinical Obstetrics & Gynaecology 18: 425-436.
- Murphy D, Johnson A, Sellers S, MacKenzie I (1995) Case-control study of antenatal and intrapartum risk factors for cerebral palsy in very preterm singleton babies. The Lancet 346: 1449-1454.
- Phelan JP, Martin GI, Korst LM (2005) Birth asphyxia and cerebral palsy. Clinics in perinatology. 32: 61-76.
- Mann JR, Mcdermott S, Bao H, Bersabe A (2009) Maternal genitourinary infection and risk of cerebral palsy. Developmental Medicine & Child Neurology 51: 282-288.
- Gibson CS, MacLennan AH, Goldwater PN, Dekker GA (2003) Antenatal causes of cerebral palsy: associations between inherited thrombophilias, viral and bacterial infection, and inherited susceptibility to infection. Obstetrical & Gynecological Survey 58: 209-220.
- Bonellie S, Currie D, Chalmers J (2005) Comparison of risk factors for cerebral palsy in twins and singletons. Dev Med Child Neurol 47: 587-591.
- Mayer PS, Wingate MB (1978) Obstetric factors in cerebral palsy. Obstetrics & Gynecology 51: 399-406.
- Reddihough DS, Collins KJ (2003) The epidemiology and causes of cerebral palsy. Australian Journal of Physiotherapy 49: 7-12.
- Rosenbaum P, Paneth N, Leviton A, Goldstein M, Bax M, et al. (2007) A report: the definition and classification of cerebral palsy April 2006. Dev Med Child Neurol Suppl 109: 8-14.
- Damiano DL (2006) Activity, activity, activity: rethinking our physical therapy approach to cerebral palsy. Physical therapy 86: 1534-1540.
- Ketelaar M, Vermeer A, Hart Ht, van Petegem-van Beek E, Helders PJ (2001) Effects of a functional therapy program on motor abilities of children with cerebral palsy. Physical Therapy. 81: 1534-1545.
- Bjornson K, McLaughlin J (2001) The measurement of health‐related quality of life (HRQL) in children with cerebral palsy. Eur J Neurol 8: 183-193.
- Waters E, Maher E, Salmon L, Reddihough D, Boyd R (2005) Development of a condition‐specific measure of quality of life for children with cerebral palsy: Empirical thematic data reported by parents and children. Child: Care, Health and Development 31: 127-135.
- Vance YH, Jenney ME, Eiser C, Morse RC (2001) Issues in measuring quality of life in childhood cancer: measures, proxies, and parental mental health. J Child Psychol Psychiatry 42: 661-667.
- Maisaarah Abd Halim
Cik Feresa Mohd Foozy
isredza rahmi A Hamid
Aida Mustapha,
A Review of Live Survey Application: SurveyMonkey and SurveyGizmo

