Introduction
Interdisciplinary collaboration is critical to excellence in research and translation of innovation, with evidence of its promotion identified across a number of forums in both primary and specialised care[1-5]. Most cancer programmes around the world are introducing interdisciplinary teamwork“(“ID- ”) as a key modality[7-11]. The literature suggests positive outcomes of ID-T, however identifying how it affects outcomes is challenging because of the variables[3,6]. Nevertheless the value of ID-T seems intuitive. The contemporary management of Acute Myeloid Leukaemia“(“AM”) is complex and from basic science research to delivery of clinical care requires a truly interdisciplinary approach among multiple disciplines [8].
The cornerstones for building a successful interdisciplinary management team are humility, tolerance, adaptability, and appreciation that alternative approaches need to be considered [1]. The hope of ID-T in the Translational Medicine of AML is that by encouraging scientific and clinical teams to approach leukaemia through a number of different disciplines while sharing data and findings with each other and acting on information produced by other teams, there is a ‘supercharge’ in innovation, creating projects where the summation of outputs/outcomes is much greater than each of the parts. AML Research through ID-T: Specifi Challenges
In establishing approaches to solve biomedical problems in AML research the focus has very much been on genetics in leukaemia, including function of the genome in the context of therapeutic objectives [13,14]. Translational approaches bridging the gap between basic and clinical sciences have been essential for conducting successful AML research. A key challenge has been that such research can be heavily department-based and at risk of isolation. Interdisciplinary centres are now found in many academic institutions and Industry [15].
Financial issues also constitute a challenge. When considering the increasing financial burden of research, an interdisciplinary approach covering several expert fields could have financial benefits. For example, combining methodological and statistical approaches could save total costs and improve the quality of each process. However such process may also give rise to financial conflicts of interest, especially among industrial and academic researcher [16].
A further challenge arises when selecting members for interdisciplinary research projects. Selection criteria for each research team member should be considered in light of the relevant interdisciplinary research objective [17].
There are a number of reasons why AML research should be conducted at an international level rather than national. This assists in study enrolment given the relative rarity of patient subgroups, and identification of ‘hard to find’ cohorts. Black and Minority Ethnic (“BME”) groups, women, and the elderly are underrepresented in cancer trials compared to white racial groups, men, and younger patients [18]. Races may differ significantly in respect of risk factors such as cytogenetics and age of onset of disease [19]. It has been reported that African American men had significantly lower rates of complete remission (54 versus 64%) and five-year overall survival (16 versus 24%) compared to white men and that they may represent a higher risk group. International AML trials also assist in the reduction of sample bias, and ensure through trial design standardisation of diagnostic/entry criteria, response criteria, and assessment of outcome [20].
Finally, regulatory issues may also constitute hurdles in AML research. New drugs or molecular targets are not necessarily approved simultaneously across different countries. In jurisdictions where approvals are pending, conducting research and clinical trials may become extremely difficult. International networks may support wider dissemination of research and treatment opportunities through mechanisms that include setting precedent, movement of individuals and teams between organisations and institutions, and partnerships where a country with licence leads as the Principle, supporting governance across the programme.
In many respects the challenges raised here are being over come in AML research through ID-T. The following section describes mechanisms for overcoming barriers in AML, many addressed in the literature of the mis 1980’s to 1990s. Although these issues and challenges persist to varying degrees recent developments are highlighted in the final section of this chapter as a means of demonstrating (through many of the principles of Translational Medicine) that these challenges can be transcended, and that AML research has flourished since the late 199’’s through ID-T and networks.
Critical Barriers and Solutions in Interdisciplinary AML Research
Research teams need to be able to overcome several key challenges. The main barriers to interdisciplinarity in AML research can be categorised under following topics:
• Attitudinal resistance,
• Communication across disciplines,
• Academic structure,
• Impediments to obtaining funding,
• Career structures, and
• Leadership capability.
The heterogeneity of research institutions, structures, and value systems, both private and public, has complicated these obstacles even further [21].
Attitudinal barriers
Despite most researchers recognizing interdisciplinary research; studies in the late 1990’s demonstrated that many were reluctant to reconsider their own research focus and some researchers considered interdisciplinary science as inadequate, with concern that quality of the interdisciplinary research may be poor due to the lack depth [21,22]. Some scientists were concerned about “purity” of their research or considered the interdisciplinary approach as a “high risk research” or “loss their professional identity” [21]. Others considered their own discipline as either “too incomplete” or “too immature” to be combined with another one [22,23]. In many respects the latter issues might be seen as the precise reason why an interdisciplinary approach could be beneficial. In other respects such attitudes are entirely natural and often based on fear of change and individual perception of the unknown.
Solutions:
Acknowledging limitations. To cooperate, researchers must acknowledge the value and limitations of both their own and others approach [21,24,25]. Each discipline should not be blinded by in its own superiority, but recognize both strengths and weaknesses, and need for personal development: so-called “Emotional Intellegence”.
Communication barriers
Scientists trained in a discipline learn a particular “language” and adopt the analytical and methodological concepts of that discipline [21]. Such “professional socialisation” has an important role in training experience; however it may constitute barriers to interdisciplinary research. This may cause two types of language problems: (i) not understanding the languages of the other disciplines; and (ii) misinterpreting the same terms used in different disciplines, which can signify something very different in each [21]. When it comes to team building, teamwork necessitates confidence in another’s expertise and leadership that is facilitatory, flexible, and inclusive [21,22].
Interdisciplinary team members may also find it difficult to evaluate each other’s performance [21,26,27].
Solutions:
Learning to speak a common language. Significant efforts must be made to learn the language of another field and to elucidate others the language of one’s own [21,22,25,28]. Building relationships. Relationships among team members affect productivity [21,29]. Thus, team members need to be able to adjust compromise and cooperate [21,22]. A feeling of community can facilitate collaborations in an interdisciplinary team [21,30].
Clear allocation of responsibilities. Clarity regarding roles, expectations, and authority in respect of sharing of data and resources are essential for an interdisciplinary team to succeed [21,31,32]. This among others requires mutually acceptable policies for disseminating research results and facilitating achievement of team member’s personal and professional objectives [21,26].
Different spaces promoting interaction. Architectural design can promote interactions [33]. Also, “virtual” proximity provides another opportunity for achieving intellectual proximity [21]. Creative and persistent leadership. Interdisciplinary research teams need leaders with strong interpersonal skills who understand the challenges of group dynamics and who can establish and maintain an integrated program [21,22].
Academic barriers
Interdisciplinary research requires a commitment from university administration [21]. Scientific education may not be sufficiently broad to produce researchers who can understand essential components of other disciplines while receiving a solid grounding in one or more fields [21].
Solutions:
In order to promote interdisciplinary AML research academic institutions should [21]:
• Allocate appropriate funds for interdisciplinary efforts in AML research,
• Consider appointment, promotion, and tenure policies to ensure that they do not hinder interdisciplinary research and education,
• Facilitate interaction among investigators through support for shared facilities, and
• Encourage development, maintenance, and evolution of interdisciplinary institutes, centers, and programs for appropriate problems in AML research.
Funding barriers
Translational scientists in AML may encounter difficulties in obtaining support for and conducting successful interdisciplinary research because funds for such research come from many agencies with different programmatic emphases [21].
Solutions:
Funding opportunities for interdisciplinary training in AML should be provided for scientists at all stages of their careers [21]. Consortia and multi-institutional programs providing integration of research efforts from various disciplines should be supported. Funding for workshops, symposia, and meetings bringing together diverse fields to focus on a particular scientific question in AML is also valuable [21].
Although the focus of the above examples is primarily on Basic and Clinical Science relationships the paradigm is of equal importance across the whole TM structure inclusive of the Applied Sciences and health service constructs.
Biology, Technology, Epidemiology, Clinical Science, Therapy: AML ID in Action, 2012.
The developments in management of AML described over the last 2 decades would not have been possible without the advances in technology described in previous chapters, bettering our understanding of the biology of stem cells and haematopoetic cell metabolism, advances in imaging, greater ability in interpreting data clinically and classifying patient subgroups, and clinical trials and datasets that function at an international level. As well as taking advantage of new knowledge, research in AML has also added to clinical science. For example in Chapter 2 we described how this has arisen through transplantation medicine supporting development and understanding of stem cell biology.
This section highlights examples of interdisciplinary institutions working in collaboration with external partners, and international networks designed to facilitate collaboration across the disciplines that make up an ideal team researching AML.
Box 1 is 4 News Article headlines from Spring 2012. Each one addresses an area of clinical-science research and is an example of interdisciplinary collaboration, taking advantage of expertise in various aspects of biology and technology pertinent to AML. Examples of collaboration in AML are protean and perhaps best demonstarted in principle by the Medical Research Council clinical trials work of the late 1990s and international collaboration over AML classification criteria (Chapter 1). However, the following have been selected on the basis of being ‘hot off the Press’ in the last few months, or of recently constructed networks that epitomise the facilitation of ID-T
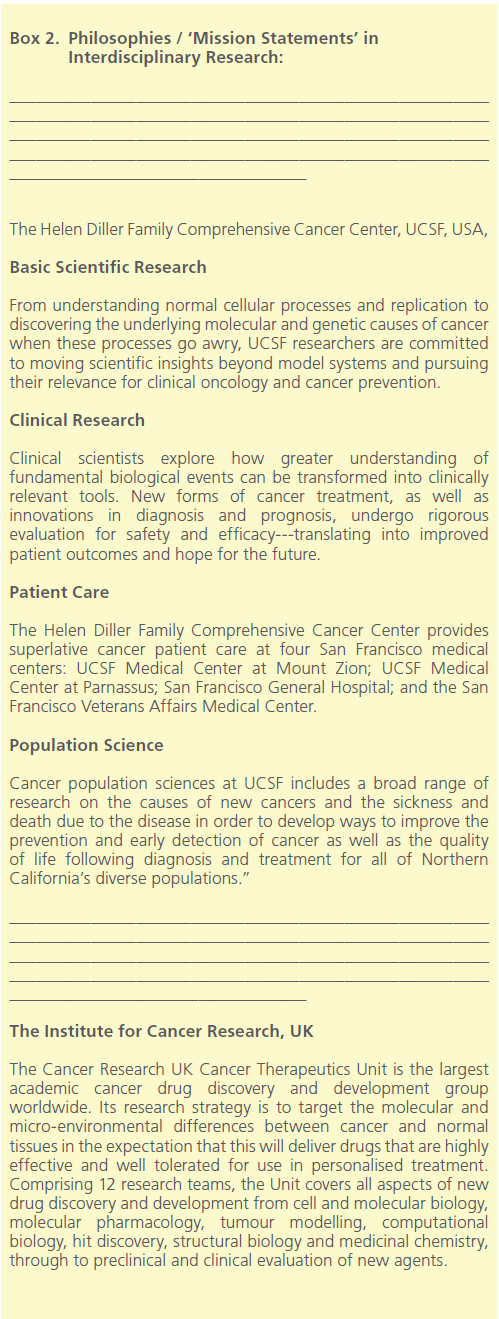
Research led by physician-scientists at the University of California, San Francisco (UCSF) Helen Diller Family Comprehensive Cancer Center has validated certain activating mutations in the FLT3 gene as targets for AML [34]. The Center combines basic science, clinical research, epidemiology / cancer control, and patient care. Their website describes an interdisciplinary model focused on Translational Medicine (Box 2) [35]. This work was completed through collaboration with colleagues at University of California, Berkley; Pacific Biosciences, California; Ambit Biosciences, San Diego; and The Abramson Cancer Center, University of Pennsylvania.
Melbourne researchers have discovered that AML may be susceptible to targeting a protein called Mcl-. The Cancer and Haematology division at The Walter and Eliza Hall Institute, along with the Molecular Genetics department worked in collaboration with scientists from the Australian Centre for Blood Diseases, St. Vincent’s Institute of Medical Research in Melbourne, and Austrian and American researchers [36].
Similarly the team at the Paterson Institute for Cancer Research at The University of Manchester, England, with colleagues at the University of Essen, Germany, have identified a new enzyme target LSD1, an enzyme controlling gene expression [37,38]. Scientists at the Cancer Research UK’s Paterson Drug Discovery Unit synthesised molecules to block LSD1, and teams at Cancer Research UK’s Leukaemia Biology Laboratory, and University of Essen demonstrated this intervention inhibits leukaemia cell growth in samples taken from both patients and in mouse models. A study by scientists at the Institute of Cancer Research (ICR), UK has also demonstrated that tranylcypromine (TCP), used to treat depressive illnesses, renders cancer cells vulnerable to the effects of a vitamin A derivative drug called ATRA used in the treatment of AML [39]. ATRA works by encouraging leukaemic cells to mature and die naturally. However resistance to ATRA arises when genes controlling cell differentiation are switched off the enzyme LSD1. Researchers identified that TCP blocks this ‘off switch’, reactivating cell differentiation and susceptibility to ATRA; a real triumph of collaboration between teams. Box 2 highlights the interdisciplinary nature of the ICR approach from its own website description [40].
By way of example of international networks, The European Leukemia Net (“ELN”) (Figure 1), is an EU funded organisation in the process of integrating input from interdisciplinary partners in diagnostics, treatment research, biometry, basic research and pharmaceutical industry to foster advancements in leukaemia related research and health care through clinical trials, promotion of translational research, introduction of standards for diagnostics and therapy, and development of evidence-based guidelines [41]. It is run via a management centre (“NMC”) with central services for education and information (“ELIC”) and a central information and communication centre (“CICS”), all essential components for maintaining integration as well as being part of the integrated team in them.
Consensus meetings involving experts from many disciplines including Information Technology, Biostatistics, Engineering, Biological Sciences and Applied Sciences and representatives from all major therapeutic research groups in Europe has been the main process by which ELN has organised itself strategically to deliver several key aims including:
Figure 1. The European Leukaemia Net Functional Structure [41].
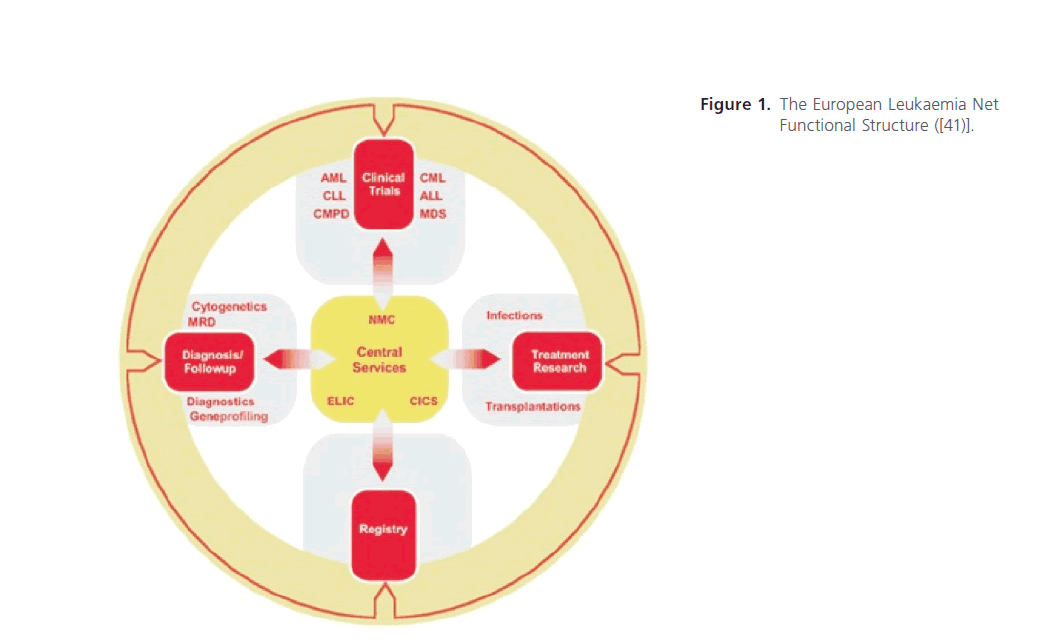
Figure 1: The European Leukaemia Net Functional Structure ([41)].
Figure 2. The National Institute for Health Research Structure [42].
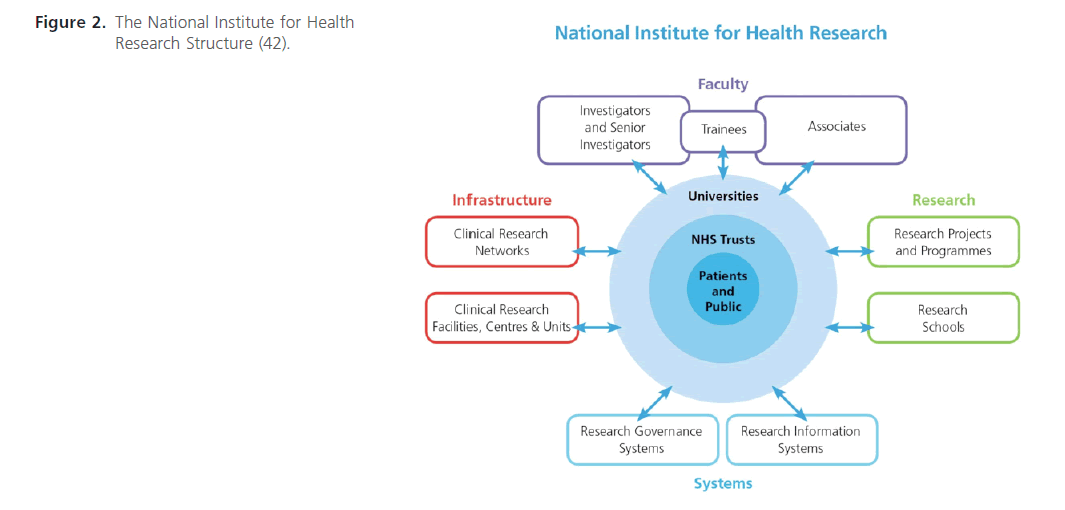
Figure 2: The National Institute for Health Research Structure (42).
• Registries: development of core data sets, essential for comparative interpretation of research results and metaanalyses. To achieve this, consensus meetings involving experts from many disciplines including Information Technology, Biostatistics, and engineering, Biological Sciences and Applied Sciences and representatives from all major therapeutic research groups in Europe have to be organised.
• Technologies platform for diagnostics including cytogenetics and molecular profiling.
• The development of prognostic models.
• Clinical trials design: detailed research planning is supported in defining crucial points such as objectives, eligibility criteria, definition of outcomes, selection of learning and validation samples, quality control, and the statistical analyses.
• Treatment research: the analysis of efficacy and safety in clinical practice.
The benefits of these integrative network approaches are:
• Finding consensus between AML trial groups.
• Adopting common protocol standards including entry criteria and patient selection.
• Common standard treatment arms in trials.
• Cross trial comparison and validation of treatment strategies provided by network structures.
• Refining the monitoring of anti-leukaemic effects on the basis of molecular MRD; and,
• Using networks as instruments to accelerate therapeutic progress against AML.
At a national level, the UK National Institute for Health Reseach (NIHR) structure [42], like the ELN structure demonstrates the interactions between different disciplines for all areas of research (Figure 2). From Figure 2, however, we are also reminded that the ID team requires the membership of health services that are able to work closely with academic organisations, and also requires the support of patients and public. Within the health service, apart from clinicians support comes from integration with government departments such as the National Institute for Clinical Effectiveness (NICE) [43] in the UK or the Food and Drugs Agency (FDA) [44], USA, and also from commissioners / financial structures that fund patient care.
Summary
In summary there are several key challenges and opportunities that arise from ID-T. Research teams in AML rely heavily on a number of disciplines and networked structures across the breadth of their work from Basic science to Community delivery of therapeutics. The challenges are not unique for teams in AML research but include: Allocation of responsibilities and creation of clear roles, expectations and objectives, Assessing performance due to different disciplinary backgrounds, Understanding the concepts, language, and the way of reasoning in different disciplines, and Acknowledging limitations in own and the others’ approaches and bridging these gaps through institutional and network structures.
The opportunities that arise include:
• Increasing and stimulating intellectual curiosity, and creation of new knowledge
• Sharing insights and learning, benefiting from diverse skills and expertise
• Broadening scientific scope and acquiring novel tools to conduct research, and
• Improving flexibility and ability to adapt new approaches and knowledge across boundaries
Integration across disciplines and creation of new knowledge requires both the correct tools and structures for bridging such groups, commitment from all stakeholders, and the right leadership capability and capacity.
Acknowledgement
We wish to thank Prof. Roy Douglas (Programme Director and Member of the Development Team) for his supervisory role in this paper.
5832
References
- Dominique, T., Danièle, R., LindaC, . et al. Evaluation of the impact of interdisciplinarity in cancer care. BMC Health Services Reserch. 2011; 11: 114
- Lemieux-Charles, L., McGuire, L. What do we know about Health Ceam tnesseffectivenes?iew review of tureliteratue. Med Care Res Rev. 2006; 63: 263-00.
- Teamwork in Health re: : Promoting Effective Teamwork in Healthcare in Canada. Polcy Synthesis and Recommendatios. 20at: https://www. chsrf.ca/Home.apx
- Ponte, PR., Gross, AH., Milliman-Richard, YJ., Lacey,K. Interdisciplinary teamwork and collaborati an An essential element of a positive practice environment. Annu Rev Nurs Res. 2010; 28: 159-89.- .
- Teamkin-Greener, H., Gross, D., Kunitz, SJ., Mukamel, D. Measuring interdisciplinary team performance in a long-term care setting. Med Care 2004; 42 (5): 47281.
- Ontario Cancer Plan 2008-2 t: https://cancercare.on.ca/common/pages/ UserFile.aspx?fieId=1308
- The NHS Cancer Plan: Three year progress report - Maintaining the momentum. 2003. Available at: https://www.dh.gov.uk/en/index.tm.
- Rabinowitz, B. Interdisciplinary breast cancer care: declaring and improving the standard. Oncoogy. 2004; 18 (10): 1263-8
- Strategies to improve and strengthen cancer control programmes in Eupe; . Report of a WHO Consultation. 2004. Availablet: https:// whqlibdoc.who.int/hq/2004/WHO_CHP_CPM_PCC_04.1.pdfhttps:// whqlibdoc.who.int/hq/2004/WHO_CHP_CPM_PCC_04.1.df.
- . Wilson, NJ., Kizer, W. Oncology management by t “ “e”” Veterans Health Administration. Cancer 1998; upplsuppl. 10): 2003-9.1-. Zorbas, H., Barraclough, B., Rainbird, K., Luxford, K., Redman, S. Multidisciplinary care for women with early breast cancer in the Australian context: what does it mean? Med J Aust. 2003; 179 (10): 52831.12. – Holland, JF., III, EF., Kufe,DW., et al. Principles of Multidisciplinary ManagemeIn: Bast, Jr, Kufe, DW., PollockRE, . etars. Holland-Frei Cancer Medicine. 5th edition. Hamilton (ON): BC Deker;.
- Collins, FS., Green, ED., Guttmacher, AE., Guyer, S. A vision for the future of genomics research. Naure. 2003; 422 (6934): 835-47.1-. Druker, BJ. Imatinib alone and in combination for chronic myeloid leukemia. Semin Hematol. 2003; 40 (1): 50-8.15- O’’Keefe, CM., Head, J. Application of logic models in a large scientific research program. Eval Program Plann. 2011; 34 (3): 174-84.16-. Parks, MR., Disis, L. Conflicts of interest in translational research. J Transl Med. 2004; 2 (1): 28.
- Silka, L. Partnerships within and beyond universities: opportunities and challenges: commentary n ““conducting interdisciplinary research to promote healthy and safe employment in healthcare: promises and pitfs”. ”. Public Health Rep. 2004; 119 (1): 73-8.18-. Murthy, VH., Krumholz, HM., Gross, P. Participation in cancer clinical trials: race-, sex-, and age-based disparities. AMA. 2004; 291 (22): 2720-6.1-. Sekeres, MA., Peterson, B., Dodge, RK., Mayer, RJ., Moore, JO., LeeEJ, . et al. Differences in prognostic factors and outcomes in African Americans and whites with acute myeloid leukemia. Bood. 20n 1;103 (11): 4036-42.2-. Cheson, BD., Bennett, JM., KopeckyKJ, . et al. Revised recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. J Clin Oncol. 2315 ;21 (24): 4642-9.
- Pellmar, Tand Eisenberg,L. Committee on Building Bridges in the Brain, Behavioral, and Clinical Sciences; Division of Neuroscience and Behavioral Health. Washington: National Academy Press. 00,. pp. 1-html22-. Sigma, Xi. Removing the Boundaries: Perspectives on Cross-Disciplinary Research: Final Report on an Inquiry into Cross- Disciplinary Science. New HenXi, The Scientific Research Socty, . 1998.2-. Bechtel,W. The nature of scientific integratiIn: Bechtel, W. Integrating Scientific Disciplines. Boston: Martinus Nijhoff Publishers. 96, . pp. 3-52.24-. Wilbanks, T. Communications between hard and soft sciencIn: Chubin, DE., Porter, AL., Rossini, A.,, Connolly, T. Interdisciplinary Analysis and Research: Theory and Practice of Problem-Focused Research and Development. Mt. Airy, Md: Lomond Publicatns, . Inc. 86, . pp. 131-140.2-. Groark, CJ., McCall, RB. Building successful university-community human service agency collaboratioIn: Fisher, CB., Murray, JP., Sigel, IE. Applied Developmental Science: Graduate Training for Diverse Disciplines and Educational Set tings. Advances in Applied Developmental Psychology. 19Cpp.Pp. 237-251.
- Druker, BJ. Imatinib alone and in combination for chronic myeloid leukemia. Semin Hematol. 2003; 40 (1): 50-8.
- O’Keefe, CM., Head, RJ. Application of logic models in a large scientific research program. Eval Program Plann. 2011; 34 (3): 174-84.
- Parks, MR., Disis, ML. Conflicts of interest in translational research. J Transl Med. 2004; 2 (1): 28.
- Silka, L. Partnerships within and beyond universities: opportunities and challenges: commentary on “conducting interdisciplinary research to promote healthy and safe employment in healthcare: promises and pitfalls”. Public Health Rep. 2004; 119 (1): 73-8.
- Murthy, VH., Krumholz, HM., Gross, CP. Participation in cancer clinical trials: race-, sex-, and age-based disparities. JAMA 2004; 291 (22): 2720-6.
- Sekeres, MA., Peterson, B., Dodge, RK., Mayer, RJ., Moore, JO., Lee, EJ. et al. Differences in prognostic factors and outcomes in African Americans and whites with acute myeloid leukemia. Blood 2004; 103 (11): 4036-42.
- Cheson, BD., Bennett, JM., Kopecky, KJ. et al. Revised recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. J Clin Oncol. 2003; 21 (24): 4642-9.
- Pellmar, TC., Eisenberg, L. Committee on Building Bridges in the Brain, Behavioral, and Clinical Sciences; Division of Neuroscience and Behavioral Health. Washington: National Academy Press. 2000. pp. 1-14.
- Sigma, Xi. Removing the Boundaries: Perspectives on Cross- Disciplinary Research: Final Report on an Inquiry into Cross-Disciplinary Science. New Haven: The Scientific Research Society. 1998.
- Bechtel, W. The nature of scientific integration. Bechtel, W. Integrating Scientific Disciplines. Boston: Martinus Nijhoff Publishers. 1996. pp. 3-52.
- Wilbanks, T. Communications between hard and soft sciences. Chubin, DE., Porter, AL., Rossini, FA., Connolly, T. Interdisciplinary Analysis and Research: Theory and Practice of Problem-Focused Research and Development. Mt. Airy, Md: Lomond Publications. Inc. 1986. pp. 131-140.
- Groark, CJ., McCall, RB. Building successful university-community human service agency collaborations. Fisher, CB., Murray, JP., Sigel, IE. Applied Developmental Science: Graduate Training for Diverse Disciplines and Educational Set tings. Advances in Applied Developmental Psychology. 1993. pp. 237-251.
- McGuire, DB. Building and maintaining an interdisciplinary research team. Alzheimer Dis Assoc Disord 1996; 13 (suppl. 1): S17-S21.
- Anbar, M. The “bridge scientist” and his role. Chubin, DE., Porter, AL., Rossini, FA., Connolly, T. Interdisciplinary Analysis and Research: Theory and Practice. 1986.
- Kane, RA. The interprofessional team as a small group. Soc Work Health Care 1975; 1: 19-32.
- Barrick, MR., Stewart, GL., Neubert, MJ., Mount, MK. Relating member ability and personality to work-team processes and team effectiveness. Ginsberg, L., Khinduka, S., Hall, JA., Ross-Sheriff, F., Hartman, A.J. Appl Psychol. 1998; 83: 377-391.
- Fagan, LA., Walter, SM. Building an interdisciplinary team: Strategies for leadership, consensus building, meetings, and performance reviews. Rehab Manage 1998-1999; 11 (1): 24-8.
- Bruhn, JG. Beyond discipline: Creating a culture for interdisciplinary research. Integr Physiol Behav Sci. 1995; 30: 331-41.
- Grant, M., Anderson, P., Ashley, M. et al. Developing a team for multicultural, multi-institutional research on fatigue and quality of life. Oncol Nurs Forum. 1998; 25: 1404-12.
- Becker, F., Steele, F. Making space for teamwork. Facilities Design Manage 1995; 14: 56-9.
- Smith, CC., Wang, Q., Chin, CS. et al. Validation of ITD mutations in FLT3 as a therapeutic target in human acute myeloid leukaemia. Nature 2012; 485 (7397): 260-3.
- Glaser, SP., Lee, EF., Trounson, E. et al. Anti-apoptotic Mcl-1 is essential for the development and sustained growth of acute myeloid leukemia. Genes Dev. 2012; 26 (2): 120-5.
- Harris, WJ., Huang, X., Lynch, JT. et al. The histone demethylase KDM1A sustains the oncogenic potential of MLL-AF9 leukemia stem cells. Cancer Cell. 2012; 21 (4): 451-3.
- Sprüssel, A., Schulte, JH., Weber, S. et al. Lysine-specific demethylase 1 restricts hematopoietic progenitor proliferation and is essential for terminal differentiation. Leukemia 2012.
- Schenk, T., Chen, WC., Göllner, S. et al. Inhibition of the LSD1 (KDM1A) demethylase reactivates the all-trans-retinoic acid differentiation pathway in acute myeloid leukemia. Nat Med. 2012; 18 (4): 605-11.

