Keywords
Migrants, Knowledge, Risk perceptions, HIV/AIDS, Gulf countries
Introduction
Migration is one of the significant factors for the rapid spread of the HIV/AIDS epidemic throughout the world. Generally, migration not only causes health threats to migrants but also increases risks for communities within receiving countries [1-3]. The total number of international migrants within the year 2010 is estimated as 214 million. The estimated migrant population in the Gulf Cooperation Council (GCC) countries is 15.1 million [4]. United Nations Joint Programme on AIDS (UNAIDS) has estimated that there are 33.3 million people living with HIV/AIDS worldwide at the end of 2009, and of these 4.9 million are living in Asia [5].
Temporary migrant workers who visit sex workers are exposed to sexually transmitted infection (STI) risks at each visit and then serve as a “bridge” for transmitting HIV/AIDS to their spouse or other sexual partners in the destination country and back home [6-8]. Inadequate knowledge of HIV transmission and prevention, misconceptions about HIV/AIDS and low perception of HIV vulnerability are still major challenges in developing countries [9-13].
Foreign employment has been a common livelihood for many adults in Nepal. Qatar, Saudi Arabia and United Arab Emirates (UAE) of the Gulf countries are the most popular destinations among Nepalese migrants for foreign employment [14-16]. Most Nepalese migrants are originally from rural areas, have lower education or vocational training and typically work in low-paid and unskilled jobs [17,18]. Nepal is experiencing a concentrated epidemic of HIV/AIDS with a higher prevalence among certain high-risk groups, such as injecting drug users (IDUs), sex workers and labour migrants [7,19].
An annual health report by the Government of Nepal estimates more than a quarter (29.5%) of adult HIV cases attributed to labour migrants [20]. Poverty, ignorance, cultural variation, internal migration and international migration for foreign employment are the major challenges for HIV/AIDS prevention in Nepal [18,19]. Sexual exposure and practice in the destination countries are known to be the risk factors for HIV/AIDS among adult Nepalese migrant workers [21,22].
The pre-departure training module introduced by government of Nepal for migrant workers travelling for foreign employment does not include comprehensive information about preventive measures of HIV/AIDS [23]. Migration and HIV/AIDS are key public health issues and are often related to each other, but still there has been little action to address them together. The original study was designed to assess the health risks and access of health care services for Nepalese migrants in three Gulf countries. The aim of this article is to report the knowledge and perceived risks of HIV/AIDS among this sample of Nepalese migrants.
Methodology
Study design and sample selection
A cross-sectional survey based on a questionnaire interview was used to obtain the information for this study. Potential participants were approached and interviewed at two different types of site within Kathmandu, Nepal: departure area of Tribhuvan international airport and the hotels and lodges near the airport and the bus park area. By recruiting the respondents from both of these sites we assumed to interview the migrants who had just returned from Gulf countries and migrants who were about to go to those countries after a stay in Nepal. The participants for this study were obtained using a convenience sampling method as there was known to be no complete sampling frame. It was assumed that approximately 50% of the Nepalese migrants might have access to health care services and to achieve a 95% confidence interval of width 45%-55% on this percentage, a sample of at least 400 participants was required [14].
Inclusion and Exclusion criteria
Only Nepalese adults who had work experience of at least six months in one of the three Gulf countries (Qatar, Saudi Arabia and United Arab Emirates), who were in Nepal at the time of recruitment and who had returned to Nepal within last 12 months (on their annual leave or for any other reason) were included in this study.
Ethical consideration
The study protocol and study tools were reviewed and approved by the Ethics committee of Nepal Health Research Council (NHRC). Before starting the data collection, approval and permission were gained from the Immigration Department, Tribhuvan International Airport in Kathmandu, and from the owners of the hotels near the airport and bus park area in Kathmandu. Verbal consent was obtained from all the potential participants before the start of the interview. Participants were informed about the purpose and the benefits of carrying out the study and were also advised that participation was voluntarily, and the questionnaire was anonymous.
Study questionnaire and data analysis
The questionnaires were adapted from Nepal Demographic and Health Survey (NDHS) and the Behavioral Surveillance Surveys (BSS) developed by Family Health International (FHI). During the initial phase of the study, a pilot study was carried out which was followed by an amendment of the questionnaire according to the requirements of the study. The final questionnaire was in both the English and Nepali languages. Four trained interviewers were involved during the data collection along with the corresponding author. The interviewers were Nepalese university graduates and were experienced in conducting research on sensitive issues. Statistical analysis was performed using SPSS version 19. Descriptive statistics were used to explore the demographic and HIV/AIDS related variables. Categorical variables were presented as counts and percentages. Chi-square tests were applied to investigate associations between the categorical variables. The p-value for statistical significance was set at 0.05.
Results
Background characteristics
Overall, 408 respondents met the inclusion criteria and were included in the study. More than half (n=218; 53.4%) were aged between 26-35 years and the majority (n=377; 92.4%) were males. A total of 162 (39.7%) respondents districts of birth were in the eastern development region of Nepal. More than three quarters of the respondents, (n=311; 76.2%), had only completed their primary level of education. The majority of the respondents (n=329; 80.6%) were married (Table 1). Only 3 of the respondents were living with their spouse during their stay abroad. Only one-fifth of the total respondents (n=78; 19.1%) were provided pre-departure training in Nepal before travelling to those destination countries.
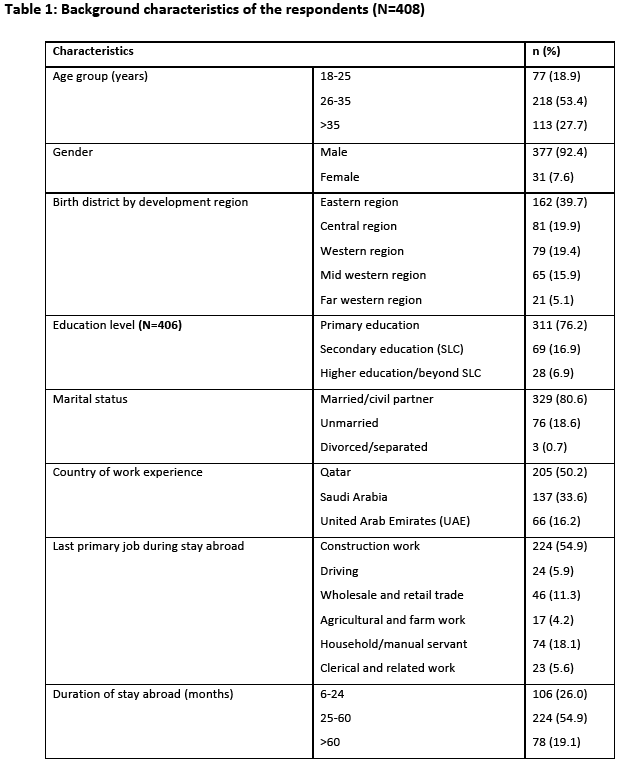
Half of the respondents (n=205; 50.2%) were currently working or had previous work experience of at least six months in Qatar. With regards to occupation, 224 (54.9%) were involved in various types of construction work. Household and manual activities, wholesale and retail trades and driving were also very common jobs among Nepalese migrant workers. More than half of respondents (n=224; 54.9%) had stayed for between 2 and 5 years in the working countries (Table 1).
Knowledge of HIV/AIDS
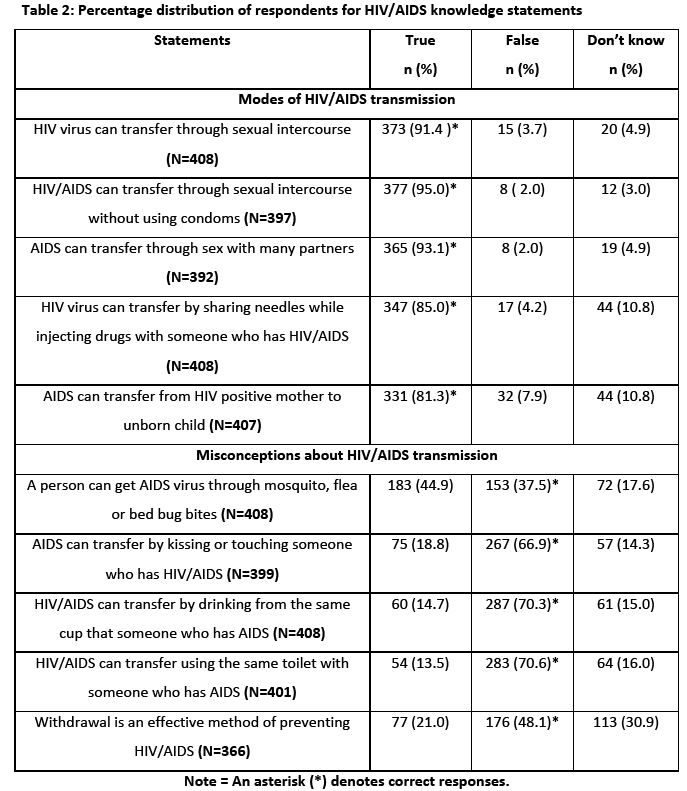
All of the respondents of this study had heard of HIV/AIDS. Half of the respondents, (n=202; 49.5%), reported that HIV/AIDS exists in the country where they were working or had a previous work experience. Regarding knowledge of the mode of transmission, the majority of the respondents were aware that HIV virus is transmitted through sexual intercourse (n=373; 91.4%), sexual intercourse without using condoms (n=377; 95.0%), and sex with many people (n=365; 93.1%). The study also found general agreement among respondents that sharing needles while injecting drug with someone who has HIV/AIDS (n=347; 85.0%), and from and HIV infected women to her unborn child (n=331; 81.3%), are ways by which HIV/AIDS can be spread (Table 2). On the other hand, the most prevalent misconception about HIV/AIDS was that a person can get HIV/AIDS from a mosquito, flea or bed bug bite if the insect has drawn blood from an HIV/AIDS infected person (n=183; 44.9%). Between 10-20% of the respondents answered that HIV can be transmitted by kissing or touching or sharing the same cup or toilets with HIV infected persons. 21% of the respondents believed that withdrawal during sex is an effective method of preventing HIV/AIDS (Table 2).
Risk perceptions of HIV/AIDS
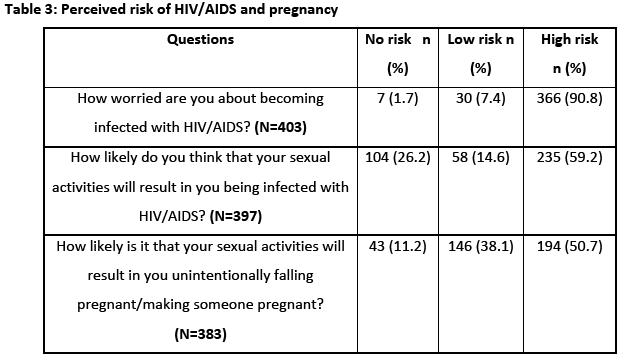
Most of the respondents (n=366; 90.8%) stated that they were worried of getting HIV/AIDS. More than a quarter (n=104; 26.2%) of the respondents perceived that they were not at risk of being infected with HIV/AIDS due to their sexual activities. Few of the respondents (n=43; 11.2%), reported that they perceived no risk of unintentionally falling/making someone pregnant due to their sexual activities (Table 3). It is not possible to assess the accuracy of these perceptions without knowing about their sexual behaviour.
Sexual Behaviour
Almost all of the respondents (99.2%), among the 393 participants who replied, had ever heard about condoms. Only 70 (17.2%) of the respondents had sexual intercourse with a partner other than their spouse during the last 12 months of their stay abroad.
Factors associated with knowledge and risk perception towards HIV/AIDS
The respondents who had obtained higher education were significantly more likely to report that HIV/AIDS can be transmitted by sharing injecting drugs needles (P=0.002) and transmission through HIV positive mother to child (P=0.015). Alternatively, the respondents who had obtained only primary education were significantly more likely to report the incorrect misconceptions of HIV/AIDS transmission than that of respondents of higher education.
Respondents who had work experience in Qatar were significantly more likely to report that HIV/AIDS could be transmitted by sharing a toilet with someone already infected with HIV (P=0.005) than respondents in the other two countries. No other significant differences were found in the percentages answering the HIV/AIDS knowledge related statements correctly between the three host countries. Married respondents were significantly more likely to report that HIV could be transmitted through having sexual intercourse without using condoms (P=0.04) and having unprotected sex with many people (P=0.01) than unmarried respondents.
Respondents of younger age (18-25) were significantly more likely to correctly answer questions on transmission via the toilet (P=0.038) and insect bites (P=0.014). Older respondents were significantly more likely to give the correct answer to the questions about transmission of HIV/AIDS from HIV positive mother to child (P=0.004) and from sharing injecting drugs needles (P=0.03) than younger respondents.
The respondents from western region of Nepal were significantly less likely to give the correct answer to the question about transmission of HIV/AIDS through HIV infected mother to child than respondents from other regions of Nepal (P=0.001). There were no significant associations between likelihood of risk perceptions and other demographic variables such as age group, working country, or birth region of the respondents. Married respondents were significantly more likely to believe that their own sexual activity made them at higher risk of unintentionally making someone pregnant (or of falling pregnant themselves) (P=0.04).
Discussion
Socio-demographic characteristics
Most of the respondents in this study were adult male. We were able to interview only 31 females. It was difficult to find more female respondents in this study because Government of Nepal has restricted female migrants from going to work in the Gulf countries in the informal sectors. There has been an increase in undocumented Nepalese female migrants travelling to the Gulf countries via different cities in India [16]. The small number of females interviewed in this study may not be representative of all the Nepalese female migrants working in the Gulf countries. The illegal migration status of some female travellers may have influenced the willingness of these women to state their true destination country and to participate in this study.
Previous research suggests that Nepalese migrants in the Gulf countries are normally low skilled labourers and only a few skilled workers [17]. Similarly, in this study most of the respondents had only primary level educational qualifications and the most common jobs were in construction related work, domestic work and marketing related jobs. It might be expected, this study also found a significant association between the education status and the last primary occupation during the stay abroad (p<0.001) with those people having lower education being more likely to have worked in unskilled jobs in construction or farm work.
Only one-fifth of the total respondents were provided pre-departure training in Nepal before going to work in different countries. The length of pre-departure training reported suggested that the idea of pre-departure training was not consistently understood by the respondents. Research findings by NIDS also suggest that majority of the Nepalese migrants do not attend pre-departure orientation and the training session also do not cover HIV/AIDS information [23]. In this study, we did not specially ask whether information on HIV/AIDS was covered during this training to those who received pre-departure training.
Knowledge and risk perceptions of HIV/AIDS
Migrants are more likely to visit sex workers which make them at higher risk of contracting HIV/AIDS and transmitting HIV/AIDS to their partners [22,24]. Most of the respondents of this study were not living together with their spouse during their stay abroad. So, they might be considered to be at risk of HIV/AIDS while they are away unless they have appropriate knowledge and perceptions about transmission of HIV/AIDS. From this study we were able to quantify the knowledge and risk perceptions about HIV/AIDS among the Nepalese migrants working in the Gulf countries.
A study found 92.6% of young people in urban Nepal had ever heard of HIV/AIDS [25]. Similarly, all of the respondents in this study had heard the term “HIV/AIDS” and in addition half of them believed that HIV/AIDS existed in the country where they were working or had worked previously. A separate study reported that the majority of immigrants (86%) in Thailand had heard of HIV/AIDS while they were in Thailand, compared to 66% before moving to Thailand [26]. However, we were not able to assess whether the respondents of this study had heard of HIV/AIDS when they were in Nepal or they first gained this knowledge while in the destination country.
Awareness about the different modes of HIV/AIDS transmission was found to be fairly high with between 80-95 percent giving the correct answers. Similarly, knowledge about the modes of HIV/AIDS transmission was found to be good among Nepalese migrants who had worked in India21 and moderately good among Nepalese adolescents.27 The study among immigrants in Thailand also found high level of awareness of different modes of HIV/AIDS transmission.26 So, the past research evidences also supports the findings of this study.
In the present study almost half of the respondents (44.9%) had a misconception about HIV transmission through insect bites. Similarly, in a previous study, the majority of Nepalese migrant workers in India believed that HIV could be transmitted by kissing, mosquito bites and social contact with HIV/AIDS patients [21]. Another separate study found 93.3% of the Nepalese adolescents were aware that HIV is not transmitted by mosquito [27] which is significantly higher as compared to the findings of our study. Transmission of HIV/AIDS through a mosquito bite if the mosquito has drawn blood from a HIV/AIDS infected person (49%) was also the most prevalent incorrect belief among immigrants in Thailand [26]. In the same study 20% of respondents believed that a person gets HIV/AIDS by sharing a meal with someone who is already infected. The percentages for both of the misconception statements of the study in Thailand are higher than the findings of this study.
30.3% of respondents of 15-49 age from Nepal Demographic and Health Survey (NDHS 2011) believed that HIV cannot be transmitted by mosquito bites, 56.8 % of them believed that HIV cannot be transmitted by sharing food with a person who has AIDS and 72.3% of them thought that HIV cannot be transmitted while touching a person who has AIDS [28]. For all these three statements, the percentages of misconceptions from NDHS findings are higher than this study.
In our study more than a quarter of respondents perceived that they were not at risk of getting HIV/AIDS due to their sexual activities. Other studies among adolescents in Nepal aged 15-24 years old suggested that far higher percentages (60-90%) of the respondents thought that they were not at risk of getting HIV/AIDS [22,27,29]. The older age of the respondents of this study with more than half (53.4%) adults of 26-35 years of age may partly explain this difference. Additionally, this study did not find any significant association between risk perceptions and age groups of the respondents. So, from previous studies we can assume that adolescents in Nepal do not perceive themselves to be at risk of HIV/AIDS.
Conclusion
This study found lack of adequate and appropriate awareness and risk perceptions about HIV/AIDS among some of the Nepalese migrants. Accurate and adequate information regarding modes of HIV/AIDS transmission are essential to the prospective Nepalese migrants to prevent the spread of HIV to the host and home countries. Collaborative efforts of both home and destination governments are crucial to reduce these migrants’ risks of exposure to HIV/AIDS. Potential migrants should be encouraged to attend the pre-departure training and information regarding health and HIV/AIDS should also be included in the training sessions. Employers in the destination countries should also be responsible for disseminating information about precautions and preventive measures for HIV/AIDS to all of their migrant workers.
Acknowledgements
We are grateful to all the respondents who participated in this study. We would like to express thanks to all of the interviewers for their hard work during administration of the questionnaire. We are also grateful to the immigration officers and hotel owners who showed good cooperation and support during data collection in Nepal. We would also like to thank the University of Aberdeen for providing a small grant fund to support the field trip to Nepal for data collection.
2653
References
- Wolffers I, Verghis S, Marin M. Health and human rights: Migration, human right and health. The Lancet 2003; 362: 2019-2020.
- Gushulak B.D, MacPherson D.W. Population mobility and health: An overview of the relationships between movement and population health. Journal of Travel Medicine 2004; 11(3): 171–178.
- Zimmerman C, Kiss L, Hossain M. Migration and health: A framework for 21st century policy-making. PLoS Medicine 2011; 8(5): e1001034.
- IOM. World migration report 2010. The future of migration: Building capacities for change. International Organisation for Migration, 2010.
- UNAIDS. Global report. UNAIDS Report on the global AIDS epidemic 2010: United Nations Joint Programme on AIDS, 2010.
- El-Bassel N, Gilbert L, Terlikbayeva A, West B, Bearman P, Wu E, et al. Implications of mobility patterns and HIV risks for HIV prevention among migrant market vendors in Kazakhstan. American Journal of Public Health 2011; 101(6): 1075-1081.
- Nepal B. Population mobility and spread of HIV across the Indo-Nepal border. Journal of Health Population and Nutrition 2007; 25(3): 267-277.
- Smith-Estelle A, Gruskin S. Vulnerability to HIV/STIs among rural women from migrant communities in Nepal: A health and human rights framework. Reproductive Health Matters 2003; 11(22): 142–151.
- Ford K, Chamrathrithirong A. Sexual partners and condom use of migrant workers in Thailand. AIDS and Behavior 2007; 11(6): 905–914.
- IOM, UNAIDS. Migration and AIDS. International Migration 1998; 36(4): 446-468.
- Saggurti N, Schensul S.L, Verma R.K. Migration, mobility and sexual risk behavior in Mumbai, India: Mobile men with non-residential wife show increased risk. AIDS and Behavior 2009; 13(5): 921–927.
- Thorne C, Ferencic N, Malyuta R, Mimica J, Niemiec T. Central Asia: hotspot in the worldwide HIV epidemic. Lancet Infectious Disease 2010; 10(7): 479–488.
- Simonet D. The AIDS epidemic and migrants in South Asia and South- East Asia. International Migration 2004; 42(5): 35-67.
- Joshi S, Simkhada P, Prescott G.J. Health problems of Nepalese migrants working in three Gulf countries. BMC International Health and Human Rights 2011;11(3). https://dx.doi.org/10.1186/1472-698X-11-3
- Sharma J, Gurung G. Impact of global economic slowdown on remittance inflows and poverty reduction in Nepal. Institute for Integrated Development Studies (IIDS), 2009.
- NIDS. Nepal Migration Year Book 2009. Nepal. Nepal Institute of Development Studies, 2010.
- Graner E, Gurung G. Arab kolahure: Looking at Nepali labour migrants to Arabian countries. CNAS Journal 2003; 30(2): 295-325.
- Thieme S, Bhattrai R, Gurung G, Kollmair M, Manandhar S, Muller-Boker U. Addressing the needs of Nepalese migrant workers in Nepal and Delhi, India. Mountain Research and Development 2005; 25(2):109-114.
- Sharma S. HIV and AIDS: The global perspectives and the challenges for Nepal. Kathmandu University Medical Journal 2004; 2(4): 283-285.
- DOHS. Annual Report (2009/2010). Ministry of Health and Population, Government of Nepal, Kathmandu, Nepal. Department of Health Services, 2010.
- Poudel K.C, Jimba M, Okumura J, Joshi A.B , Wakai S. Migrants’ risky sexual behaviours in India and at home in far western Nepal. Tropical Medicine and International Health 2004; 9(8): 897–903.
- Tamang A, Nepal B, PuriM ,Shrestha D. Sexual behaviour and risk perceptions among young men in border towns of Nepal. Asia-Pacific Population Journal 2001; 16 (2): 195-210.
- Gurung P, Roy R, Ghotane R, Limbu B. State of Migrants Health 2005. Nepal Country Report, Nepal Institute of Development Studies (NIDS), 2006. [Online] Available from: https://www.caramasia.org/enews/2007/april/inside/soh_country_reports/nids_booklet.pdf
- Singh S, Mills E, Honeyman S, Suvedi B.K, Pant N.P. HIV in Nepal: Is the violent conflict fuelling the epidemic? PLoS Medicine 2005; 2(8): e216.
- Neupane S, Nichols D, Thapa S. Knowledge and beliefs about HIV/AIDS among young people in urban Nepal. Asia-Pacific Population Journal 2003; 18(4): 39-52.
- Fuller T.D, Chamratrithirong A. Knowledge of HIV risk factors among immigrants in Thailand. Journal of Immigrant & Minority Health 2009; 11(2): 83–91.
- Mahat G, Scoloveno M.A. HIV/AIDS knowledge, attitude and beliefs among Nepalese adolescents. Journal of Advanced Nursing 2006; 53(5): 583-590.
- MoHP. Nepal Demographic and Health Survey 2011. Government of Nepal. Ministry of Health and Population, 2012.
- Puri M, Cleland J. Sexual behaviour and perceived risk of HIV/AIDS among young migrant factory workers in Nepal. Journal of Adolescent Health 2006; 38(3): 237–246.

