Keywords
Knowledge; Attitude; Practice; Unsafe abortion; Female students; Preparatory school; Southeast ethiopia
Background
Abortion is the termination of a pregnancy by the expulsion of a fetus or embryo from the uterus. An abortion can occur spontaneously due to complications during pregnancy or can be induced. Abortions are categorized as safe or unsafe using World Health Organization definitions (WHO). WHO defines unsafe abortion as a procedure meant to terminate an unintended pregnancy that is performed by individuals without the necessary skills, or in an environment that does not conform to the minimum medical standards, or both. In the context of human pregnancies, an abortion induced to preserve the health of the pregnant female is termed as therapeutic abortion, while an abortion induced for any other reason is termed as elective abortion. By convention, induced abortion is usually defined as pregnancy termination prior to 20 weeks or less than 500-gm birth weight(for developed countries) and 28 weeks gestation or less than 1000-gm birth weight (for developing countries, like Ethiopia) [1,2].
Deliberate terminations of pregnancy have been traced back to ancient times. There are evidences to suggest that historically ,pregnancy where terminated through a number of methods including administration of aborting agent, herbs, the use of sharpened implement, application of abdominal pressure and other techniques [3].
In Ethiopia, abortion has been contributing to the high maternal mortality rate (MMR). The risk groups, (mothers and children) have priority in health service implementation. Worldwide, the plan to achieve the Millennium Development Goal 5 is focusing on maternal and child health as a primary goal in health program. To achieve the MDG 5 of reducing maternal deaths by three-fourths by 2015, particularly in sub-Saharan Africa, like Ethiopia, the issue of abortion has to be systematically addressed [4].
The demand for abortion in this poor and predominantly rural country is rooted in low contraceptive use and high levels of unintended pregnancy. Indeed, only 14% of Ethiopian women of reproductive age use contraception and more than 40% of pregnancies are unintended. Expansion of contraceptive services is crucial if unintended pregnancy and abortion-related mortality and morbidity are to be reduced. The main causes of death from unsafe abortion are hemorrhage, infection, sepsis, genital trauma, and necrotic bowel. Poor wound healing, infertility, consequences of internal organ injury (urinary and stool incontinence from vesico-vaginal or recto-vaginal fistulas), and bowel resections are not ignored. It is also one of the most easily preventable and treatable [5,6].
Adolescence course is a time of transition from childhood to adulthood where new behaviors are learned more easily, in Ethiopia history adolescent and young people ages 10-24 are the largest group ever to be entering adulthood most of them are facing reproductive health problem one of which is unsafe abortion. Limited knowledge of sexual psychology, early marriage, limited use of contraceptive, limited access to reproductive health information and education over their sex life, all contribute to high rate of pregnancy for which abortion done in unsafe condition [7]. Unsafe abortion may be induced by the women herself, by non medical persons or by health workers in unhygienic conditions, such abortions may be induced by insertion of a solid object (usually root, ting or catheter) into the uterus in improperly performed dilation and curettage procedure, ingestion of harmful substances or external force. The mortality and morbidity risks of induced abortion depend on the facilities and skill of the abortion provider methods used and certain characteristics of the women herself such as general presence of reproductive tract infections, STI, age parity and stage of the pregnancy. The risks involved also depend on the availability and the utilization of treatment facilities once complication has occurred [8].
Worldwide approximately 20 million unsafe abortions performed each year, resulting nearly 80,000 maternal deaths and hundreds of disabilities. In Africa the risks of dying after unsafe abortion is one in hundred fifty. Several studies indicated that unsafe abortion accounts for up to 25-35% of maternal deaths in Ethiopia being a critical public health problem with possible complication like hemorrhage, sepsis, incomplete abortion and damage to internal organs [9].
Legality of abortion and cooperation with NGOs are some of the country’s health activities to reduce maternal mortality. Marie Stops International (MSI) is one of the most dynamic NGO works to reduce the number of unsafe abortions globally by rapidly expanding access to comprehensive sexual and reproductive health services, including safe abortion and post abortion care [10]. Hence, the importance of doing this research is to be used as a base line by policy makers, public health planners and administrators and significant others to explore the way to reduce risks of unsafe abortion and prevention.
Methodology
Study design, area and period
An institutional based cross sectional study was conducted from April 1-12, 2013 at Goba town.
Sample size determination
The sample size were determine using single population proportion formula by assuming proportions of female student in Batu Terara preparatory school Goba town who are aware of unsafe abortion to be 50%, 5% marginal error and 95% confidence interval. By considering 10% contingency for non-respondent the finale sample size were 196.
Sampling technique and procedure
The study was conducted using systematic sampling method. The student attendance sheet was used as sampling frame.
Data collection
Data were collected by using closed ended questionnaires and prepared in English language, which were held with a method of self administered data collection tool.
Data quality control
To ensure the quality of data the pre test were given on Robe preparatory school female students for 30 students one week prior to the time of data collection. There were immediately data checking data for their completeness and clarity.
Data processing and analysis
After the data collection, each questionnaire was checked for its completeness. Data cleaning and editing as well as coding were done. The data was analyzed using SPSS version 16. To ascertain the level of female preparatory students’ knowledge about unsafe abortion, 8 knowledge assessment questions were provided for those respondents who have heard about unsafe abortion. To obtain the summarized extent of knowledge of female students of Batu Terara preparatory students each knowledge assessment question response were recorded into the value ‘1’ for correct answers and the value ‘0’ for the incorrect answers in the first place. Then respondents’ correct responses to the questions were aggregated. And based on the cumulated correct responses score, the study subjects were classified as not knowledgeable and knowledgeable about unsafe abortion. On the same hand, the level of attitude and practice were ascertained on the same manner.
Ethical consideration
Ethical clearance was obtained from Madda Walabu University College of medicine and health sciences. Informed verbal consent was obtained from each participates.
Results
Socio- demographic characteristics
From a total of 196 female students who were given self-administered questionnaire 182(92.85%) were responding voluntarily. The study shows out of 182 female students 167(91.8%) were between15-19, 12(6.6%) were between 20-24 and the rest 3(1.6%) were above 25years, for this distribution age the mean were 18.38 with variance and standard deviation of 2.2 and 1.48 respectively and also the minimum age were 16 and the maximum were 26 and their religious status 134(73.6%) were Orthodox, 24(13.2%) were Muslim, 22(12.1%) were protestant. The study also showed their ethnicity 117(64.25%) were Oromo, 44(24.2%) were Amhara 10(5.5%) were Tigre and 11(6.05%) were other ethnic groups and their marital status 156(85.7%) were single, 15(8.4%) were married, 8(4.3%) were divorced, and the remaining three (1.6%) were widowed (Table 1).
| Characteristics |
Frequency |
Percent |
| Age in year |
|
|
| 15-19 |
167 |
91.8% |
| 20-24 |
12 |
6.6% |
| >=25 |
3 |
1.6% |
| Religion |
|
|
| Orthodox |
134 |
73.6 |
| Muslim |
24 |
13.2 |
| Protestant |
22 |
12.1 |
| Others |
2 |
1.1 |
| Ethnicity |
|
|
| Oromo |
117 |
64.25 |
| Amhara |
44 |
24.2 |
| Tigre |
10 |
5.5 |
| Others |
11 |
6.05 |
| Marital status |
|
|
| Single |
156 |
85.7 |
| Married |
15 |
8.4 |
| Divorced |
8 |
4.3 |
| Widowed |
3 |
1.6 |
Table 1 Socio- demographic characteristics of female students in Batu Terara preparatory school Goba town April, 2013.
From these respondents 33(18.1%) have been pregnant and the rest 149(81.9%) never had been. Among those who had been pregnant 24(13.18%) were conceived once, 7(3.8%) were two times and the rest 2(1.09%) were pregnant more than two times.
Knowledge
Out of 182 respondents 108(59.34%) were knowledgeable and the rest 74(40.66%) were not knowledgeable.
Majority of the respondents 113(62.1%) know how to prevent pregnancy, but the rest 69(37.9%) were not. Among those who did not know how to prevent pregnancy 23(12.6%) were heard about pills, 32(17.58%) about condom, 22(12.08%) about loop. Among the respondents 83(45.6%) knows how to induce abortion, while 99(54.4%) were not. Of those who know the method how to induce 17(9.34%) know about insertion of solid object, 29(15.93%) know ingestion of harmful substance. It is briefly presented in Table 2.
| Methods they know to induce abortion |
Frequency |
Percent |
| Insertion of solid objects |
17 |
9.34 |
| Ingestion of harmful substance |
29 |
15.93 |
| By health professionals |
79 |
43.4 |
| Others |
3 |
1.64 |
| Total |
128 |
67.21 |
Table 2 Methods how to induce abortion of female students in Batu Terara preparatory school, Goba town, south east of Ethiopia, April, 2013.
While assessing the safe method to induce abortion, 77(42.3%) said by health professional, 6(3.29%) ingestions of harmful substance and 5(2.74%) said Insertion of solid object (Figure 1).

Figure 1 Knowledge of safe method to induce abortion of female students in Batu Terara preparatory school, Goba town southeast Ethiopia, April, 2013.
The study was ascertained level of knowledge complication of unsafe abortion, 83(45.6%) were knew and of those 51(28.02%) know bleeding, 36(19.78%) infection, 28(15.38%) internal organ damage, 24(13.2%) know infertility and 43(23.62%) know death, but the rest 99(54.4%) were not knew the complication of unsafe abortion. Concerning legalization status of abortion in Ethiopia 60(33.1%) said it is legalized, 64(35.2%) of them mentioned is not legalized and the rest 58(31.7%) did not know about legalization status of abortion.
Attitude
Out of 182 female students who were ascertained their level of attitude 85(47.8%) of the respondents had positive attitude and the remaining 97(52.2%) had negative attitude. Most of the respondents had attitude towards an intended pregnancy 106(58.25%) need to induce abortion while the rest 72(41.75%) need to continue pregnancy. The respondents preferable place to induce abortion were 70(38.46%) wants at health institution 10(5.49%) at home and the remaining 102(56.05%) prefer traditional healer. Concerning the right of abortion to prevent 70(38.5%) said themselves 63(34.6%) government, 24.7%) family (Figure 2).
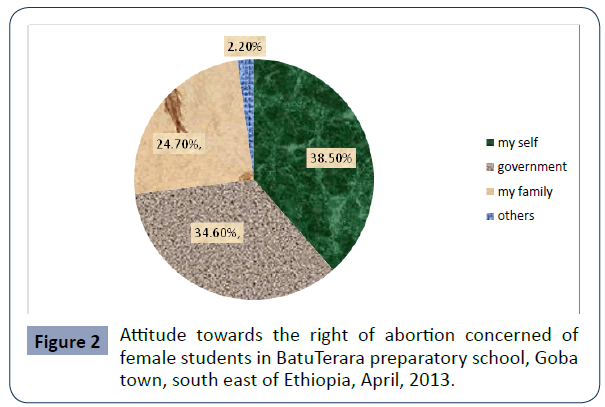
Figure 2 Attitude towards the right of abortion concerned of female students in BatuTerara preparatory school, Goba town, south east of Ethiopia, April, 2013.
About 64(35.16%) of the respondents’ were agreed about legalization of abortion in our country, 89(48.9%) disagreed and the rest 29(15.94%) were indifferent. At the same time 66(36.3%) of the respondents’ were answered all abortion performed in health institution are safe, while the rest 116(63.7%) were replied not.
Practice
From 182 respondents 67(37.64%) were used family planning method, among those 18(9.89%) were used pills, 36(19.78%) condom were used and the remaining 111(62.36%) had never used (Figure 3).
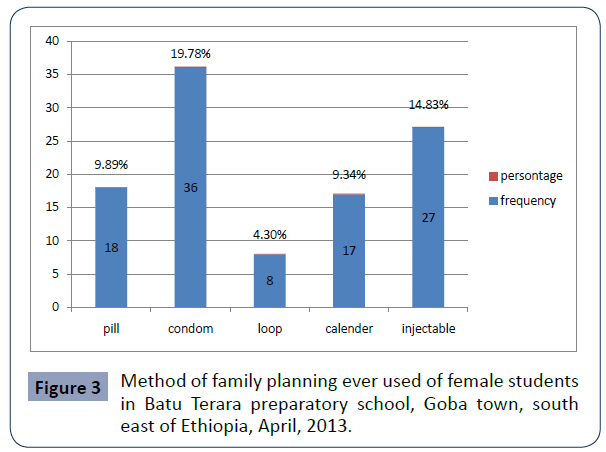
Figure 3 Method of family planning ever used of female students in Batu Terara preparatory school, Goba town, south east of Ethiopia, April, 2013.
Concerning the experience of abortion 22(12.08%) were experienced, of them 19(10.43%) were by inducing and 3(1.64%) were spontaneously, while the rest 160(87.92%) were not experienced. Among those who experience abortion 12(6.59%) of them were experienced once, 4(2.19%) of them were twice, and the rest 3(1.64%) were more than two times. The study also assessed the reason to induce abortion 14(7.69%) were due to fear family criticism, 13(7.14%) were due to economic problem (Table 3).
| Reason to induce abortion |
Frequency |
Percents |
| Fear of family criticism |
14 |
7.69 |
| Economic problem |
13 |
7.14% |
| Not personally interested to have baby |
5 |
2.74% |
| Rape/incest |
3 |
1.64% |
Table 3 Reasons of female students to induce abortion in Batu Terara preparatory school, Goba town, south east of Ethiopia, April, 2013.
While checking who perform abortion 8(4.39%) were induced by health professionals, 10(5.5%) were by traditional healer and the rest 5(2.74%) were induced by themselves. In associated to these their reason 9(4.94%) were for the sake of cost, 12(6.6%) were due to sake of secret and the rest 8(4.39%) were due to sake of safety. Among those who perform abortion 8 (4.39%) of them were by health professionals, 10(5.5%) were by insertions of solid object (Figure 4).
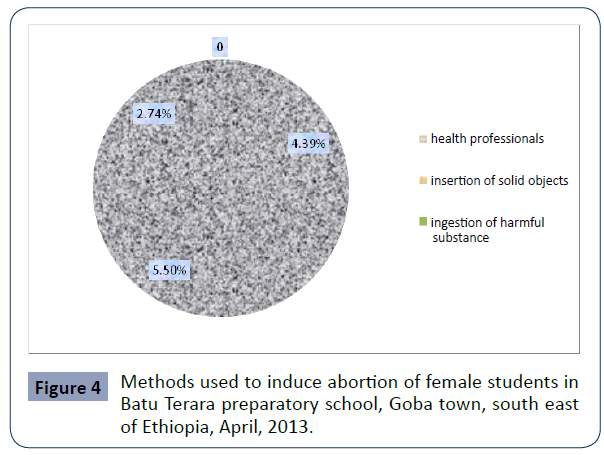
Figure 4 Methods used to induce abortion of female students in Batu Terara preparatory school, Goba town, south east of Ethiopia, April, 2013.
Out 22 female student who experience abortion 19(10.43%) of them were faced bleeding, 11(6.04%) infection (Figure 5).
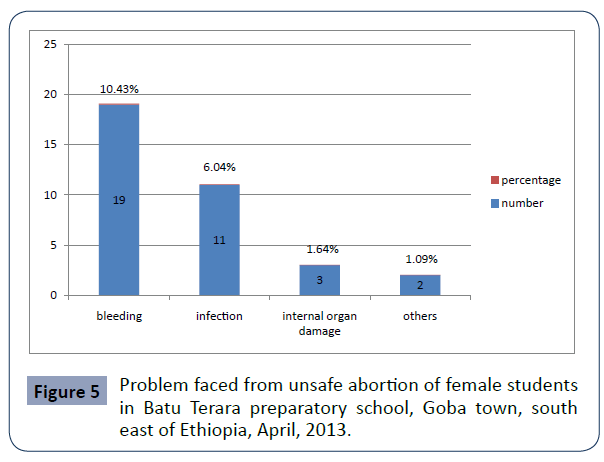
Figure 5 Problem faced from unsafe abortion of female students in Batu Terara preparatory school, Goba town, south east of Ethiopia, April, 2013.
Discussions
The aim of this study was to assess KAP on unsafe abortion among female students in BatuTerara preparatory school. Lack of awareness about prevention of unintended pregnancy and negative attitude towards unsafe abortion contribute the main reason for increment of unsafe abortion. A study of this type is therefore, found to be very important. The result of this study shows that 15(7.13%) were practiced by traditional healer and themselves from those experienced abortion, which increases the likely hood of unsafe abortion. Unsafe abortion showed an exaggerated in developing countries [11]. This could be due to high level of family criticism and economic problem to have safe abortion. In this study 22(12.08%) were practiced abortion of those 16(8.79%) were less than 20 years of age which is less than from the data showed in 2003 for the developing country for the same age which was 14% [3]. This could be due to the availability of private health care providers in these commercial centers draws women from surrounding areas. This study reveals among the total of 19(10.4%) who induce abortion 8(5.5%) were performed in health institutions [12-18]. In 2008, 27% of induced abortions were safe procedures performed in health facilities [19]. This could be due to improve level of knowledge and attitude towards health institutions to practice induced abortion. The result of this study showed among the total of 22 students who practiced abortion, 19(10.43%) and 11(6.04%) were faced bleeding and infection respectively. Whereas, study conducted on abortion at Jimma hospital 2008 shows that among the total of 80 patients with diagnosis of induced abortion 50(62.5%) were admitted for bleeding and infection [16]. Even if it is still low as compared to the study shown in Jimma, it could be due to difference in the study design. The result of this study shows about 13(7.14%) were due to economic problem and 14(7.69%) were due to fear of family criticism which showed the highest proportion. the same study revealed that 18(22.5%) of the case gave economic problem as the main reason for abortion [20].
Conclusion
The study showed that 108(59.34%) were knowledgeable and the rest 74(40.6%) were not. From total of respondents 85(47.8%) had good attitude and the rest 97(52.2%) had not good attitude. Majority of the respondents who practiced induced abortion 16(8.79%) were under 20 years of age and the reason to induce abortion 27(14.83%) were due fear of family criticism and economic problem as well 15(8.24%) were performed induced abortion by traditional healers and themselves. The major toll of complication faced during abortion were bleeding 19(10.4%) which accounts the highest rank, while infection were the second leading which were 11(6.04%) and the rest includes internal organ damage 3(1.64%).
Competing Interests
The authors declare that they have no any competing interests.
Authors' Contributions
All authors have contribution to the manuscript; all authors read and approved the final manuscript.
Authors’ Information
AYM is an assistant professor at Madda Walabu University and ALW is an assistant professor at Madda Walabu University and TE is lecturer at Madda Walabu University.
Acknowledgments
We are grateful to Madda Walabu University for supporting this study. We are also very grateful to data collectors and study participants to undertake this study.
36817
References
- Cunningham FG, Lenevo KJ, Bloom SL, Hauth JC, Gilstrap III, et al. (2007) Williams Obstetrics (22ndedn). McGraw-Hill Companies medical publishing division, Section III.
- Negussie S (2006) Obstetrics and gynecology for health science student. Lecture Note.
- Alan Guttmacher Institute (1999) Sharing responsibility woman, society and abortion worldwide.New York USA.
- Wirth M, Sacks E, Delamonica E, Storeygard A, Minujin A, et al. (2008) delivering” on the MDGS: equity and maternal health in Ghana, Ethiopia and Kenya. East Afr J Public Health 5: 133-141.
- Haddad LB, Nour NM (2009) Unsafe Abortion: Unnecessary Maternal Mortality. Rev Obstet Gynecol 2: 122–126.
- Singh S, Fetters T (2010) Access to Abortion Step By Step, Ethiopia Pushes Back Unsafe Abortion, a report jointly authored by Ipas and the Guttmacher Institute.
- FDRE Ministry of Health (2007) National Adolescent and Youth Reproductive health strategy 2007-2012.
- Meskel YW, Chekol A (1999) Induced Abortion and Problems of Sexual Health, South West Ethiopia Ethiopian Journal of Health Science 9: 77-78.
- Stanley K, Haw H, Singh S, Haas T (1999) The Incidence of Abortion, Supplement. International Family Planning Perspectives 25:30–38.
- Marie Stopes International (2010) Safe abortion and post abortion care.
- World Health Organization (1994) Abortion: a tabulation of available data on the frequency and mortality of unsafe abortion. WHO/FHE/MSM/93. Geneva.
- World Health Organization (2003) Unsafe Abortion: Global and regional estimates of the incidence of unsafe abortion and associated mortality in 2003. Geneva.
- Guttmacher institute (2010) Facts on Unintended Pregnancy and Abortion in Ethiopia.
- Buruh G (2011) Assessment of Determinants of Induced Abortion Among Child Bearing age Women Attending Maternal and Child Health clinic in Mekele town. Tigray, Ethiopia.
- Singh S, Fetters T, Gebreselassie H (2010)The estimated incidence of induced abortion in Ethiopia. International Perspectives on Sexual and Reproductive Health 36: 16-25.
- Braeken, Doortije, Upieka de S Liva, Seidy E (2020)Use Working group meeting report. International planned parenthood.
- Benson J, Nicholson LA, Gaffucin L, Kinotp SN (1996) complications of unsafe abortion in sub-saharan Africa: a review. Health Policy and Planning 11: 117-131.
- Population Reference Bureau (2008) 2008 World Population Data Sheet. Washington, DC: PRB.
- The Guttmacher Institute (2009) Facts on the Sexual and Reproductive Health of Adolescent Women in the Developing World. New York: The Guttmacher Institute.
- Shan I, Ahima E (2004) Age Patterns of unsafe abortion in developing countries,regions. Reprod Health Matters 12: 9-17.

