Mariangela Panebianco1,2, Patrizia Perrone2, Antonino Pavone3, Domenico Restivo3, Maria Signorelli4, Cannavò Dario5 and Eugenio Aguglia4
1Department of Molecular and Clinical Pharmacology, Institute of Translational Medicine, University of Liverpool, UK
2Department of Neurology, Civile Hospital of Legnano, Asst Ovest Milanese, Italy
3Department of Neurology, Garibaldi Hospital of Catania, Italy
4Department of Psychiatry, University of Catania, Italy
5Department of Psychogeriatrics, ASP 3 of Catania, Italy
*Corresponding Author:
Mariangela Panebianco
Department of Molecular and Clinical Pharmacology
Institute of Translational Medicine, University of Liverpool, UK
Tel: 00393492807975
E-mail: dott_mariangela@hotmail.com; mariangela.panebianco@asst-ovestmi.it
Received Date: October 27, 2016; Accepted Date: November 23, 2016; Published Date: November 28, 2016
Citation: Panebianco M, Perrone P, Pavone A, et al. Left Temporal Neuronal Hyperexitability as a Predictor of Mild Cognitive Impairment: Clinical and Neurophysiological Study. J Neurol Neurosci. 2016, 7:6 doi: 10.21767/2171-6625.1000158
Keywords
Mild cognitive impairment; Hippocampal hyper-exitability; Electroencephalogram; Slow waves
Introduction
The temporal lobe is a structure anatomically connected to the memory, cognitive processes and affectivity and frequently implicated in epilepsy [1]. Temporal lobe epilepsy and mild cognitive impairment are both subject to intensive memory research. Memory problems are a core characteristic of both conditions and we wonder if there are analogies which would enrich the two distinct research communities [2].
Dementia is a definition for decline in various mental abilities such as memory, speech and cognition severe enough to interfere with daily life [3]. Mild cognitive impairment (MCI) usually is the early stage of dementia which is defined as decreasing in mental abilities such cognition, memory, and speech not too severe to interfere daily activities. MCI diagnosis is rather hard and usually assumed as normal consequences of aging [4].
Diagnosis is usually performed through a combination of extensive testing (psychological tests, neurological examination, and magnetic resonance) and eliminations of other possible causes [5].
“Seizures” or neuronal hyper-exitability in the temporal lobe, transiently impair cognition and steadily damage hippocampal circuitry, leading to progressive memory loss, but the mechanisms for hyper-exicitability in AD brain are largely unknown.
In the recent years, several research groups have applied different analyzing methods to find some relations between EEG signal and MCI. In patients with sporadic dementia, scalprecorded EEG patterns typically show abnormalities predominantly composed for slowed background rhythms [6].
Monitoring the mental state contributes both to prevention and monitoring initial symptoms of cognitive impairment will decrease considerably memory complaints and prevent the onset of neurodegenerative diseases. We also state early detection of cognitive impairment will delay dementia and associated illness [7].
Objective
The objective of this study was evaluated the correlation between EEG pattern abnormalities in the left temporal region and a progressive cognitive impairment.
Material and Methods
Study design
This was a clinical and neurophysiology case-control study in healthy adult’s patients with EEG pattern characterized by slow activity in left temporal region.
The investigator did not intervene and rather simply “observed” and assessed the strength of the relationship between a risk factor and disease variables [8]. In fact, casecontrol study usually identifies subjects by outcome status at the outset of the investigation. Once outcome status is identified and subjects are categorized as cases, controls (subjects without the outcome but from the same source population) are selected.
This study lasted three years in total, being divided into two phases: recruitment (for an entire year) and follow-up after 1 year. Admission criteria were checked. The follow-up consisted of neuropsychological assessment with Mini Mental State Examination (MMSE) and MRI scan.
Patient population
Our analysis was based on pooled of patients from Neurophysiology Department in Italy from February 2010 to July 2013. These subjects aged between 40 and 60 years and referred to our out-patient department for episodes of loss of consciousness, headache, dizziness.
Inclusion criteria were: 1) adult patients (aged 40-60 years), 2) pattern EEG with slow waves in left temporal; 3) written informed consent.
Exclusion criteria were: 1) brain trauma; 2) brain cancer; 3) severe psychiatric diseases; 4) degenerative neurological disease; 5) brain malformations; 6) history of childhood epilepsy; 6) abnormal values of laboratory screen considered to be of clinical significance; 7) chronic medications; 8) pathological perinatal events; 9) alcohol and substance abuse.
Withdrawal criteria were: withdrawal of informed consent; deterioration in seizure control sufficient to cause clinical concern; other severe illness.
Each subject underwent a pre-inclusion study evaluation that included history, physical examination, EEG and MRI.
Case group: Subjects with typical alterations on EEG as sharp slow-wave in the left temporal.
Control group: Subjects without specific alterations on EEG.
Electroencephalogram recording
All EEG signals were recorded in the morning times while subjects resting comfortably in a quiet room with closed eyes. The EEG activity was recorded continuously from 19 electrodes positioned according to the 10–20 International system. Data were recorded using 32 channel digital EEG device with 256 Hz sampling rate (Galileo NT, EBneuro, Italy). Electrodes-skin impedance was set below 5 kΩ.
The recording duration was 30 min because longer recordings would reduce the variability of the data and suppress noise and artifacts, but also possibly increase the slowing of EEG oscillations due to reduced vigilance. Hence, during recording procedure, subjects were been checked out continuously to keep them conscious and avoid drowsiness.
Statistical analysis
The average was expressed as means ± SD. The investigated variables were the number of patients with cognitive impairment and that one with MRI abnormalities among those who were with and without left temporal lesion EEG pattern (LTEP). We dichotomized those as “absent” or “present”. So we examined the univariate odds ratios (ORs) that provided an estimate of the strength of association between LTEP and explored variables.
The odd ratio was calculated with a 95% confidence interval (CI) for both, according to [9] while P-value is calculated according to Sheskin [10].
Results
Demographic and clinical data
One hundred forty patients were recruited and one hundred thirty completed the 24-month study.
Of the ten patients who did not complete the study, five patients in experimental group and three patients in control group did not have follow-up and were excluded from outcome analyses. The reasons for withdrawal were intercurrent illness (8 patients) and death (2 patients).
Population included 85 females and 45 males. In case group we had 60 subjects, 15 males and 45 females with sharp slowwave in left temporal region on EEG (Figure 1) Mean age was 58.2 ± 7.1 years. In control group we had 70 subjects, 30 males and 40 females with normal EEG (Figure 2). Mean age was 54.1 ± 8.2 years.
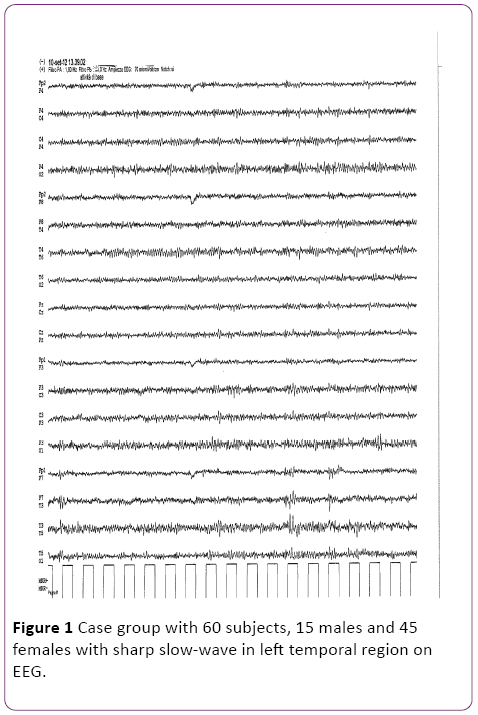
Figure 1: Case group with 60 subjects, 15 males and 45 females with sharp slow-wave in left temporal region on EEG.
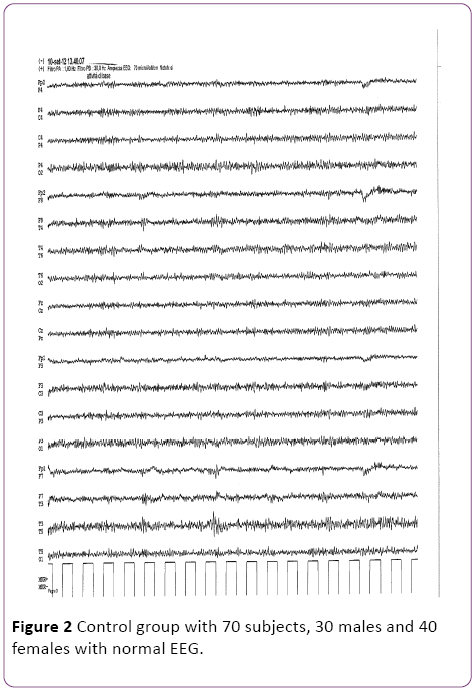
Figure 2: Control group with 70 subjects, 30 males and 40 females with normal EEG.
Demographic characteristics and clinical data for 130 patients are summarized in Table 1.
| |
Sex |
Age (mean) |
Episodes of loss of consciousness |
Headache |
Dizziness |
| Case (n=60) |
15 males
45 females |
58.2± 7.1 |
32 |
19 |
9 |
| Control (n=70) |
30 males
40 females |
54.1± 8.2 |
35 |
25 |
10 |
Table 1: Summary of demographic data.
Outcome analysis
57 patients (Case) and 33 patients (Controls) showed a mild cognitive impairment (MMSE ≥ 23 adjusted for age and education) (Graph 1).
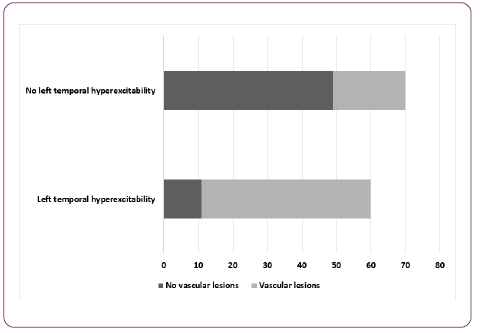
Graph 1: Correlation between left temporal neuronal hyperexitability and vascular lesions.
49 patients (Case) and 21 patients (Controls) with deep lacunar infarcts or subcortical white matter alterations on MRI scan (Graph 2).
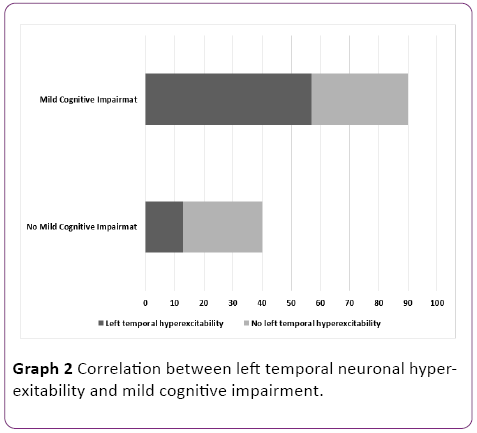
Graph 2: Correlation between left temporal neuronal hyperexitability and mild cognitive impairment.
Overall, 95% had development neurocognitive impairment in case group vs 47% in control group.
Nearly 8% of patients were unavailable for follow-up and this was a study limitation.
Analysis performed according to methods proposed by Koch showed that pattern EEG of slow waves significantly correlated with both variables MCI (P<0.0001) and vascular alterations (P<0.0001). The outcome analysis is summarized in Table 2.
| |
OR |
95% CI |
Z statistic |
p-value |
Patients with MCI
(n= 57/60) |
21.30 |
6.30 to 74.52 |
4.79 |
P<0.0001 |
| Patients with vascular lesions (n=49/60) |
10.39 |
4.53 to 28.84 |
5.53 |
P<0.0001 |
Table 2: Outcome analysis – Odd ratio and 95% confidence interval estimates by EEG patterns, predicting in vascular lesions and MCI.
Discussion
Diagnosis of MCI is hard, and symptoms are often dismissed as normal consequences of aging. In this study, we proposed a reliable and accurate method to discriminate MCI versus normal cases using neurophysiological features.
In fact, in our sample, pattern EEG was predictive for vascular abnormalities and MCI more than 50% after a few years. As described in the literature, well-designed observational study have been shown to provide results similar to randomized controlled trials [11].
Neurons, glial cells, endothelial cells of the blood-brain barrier produce pro-inflammatory elements such as IL-1 beta as answer at injuries: this process precedes the neuronal hyperexcitability condition. The hypothesis suggested that injuries in some regions in the patient’s brain with dementia are caused by inflammatory process. Thus, neuro-excitability and cognitive impairment have the same cause. Furthermore, a lot of studies show that the cerebrovascular disease can stimulate plaques and neurofibrillary tangles, typical elements in brain’s dementia.
Conclusion
The proposed feature selection and classification procedure shows very promising and interesting results.
In summary, typical geographic alterations in left temporal region are “indicators” or “markers” of early cognitive impairment and may be used as a prevention strategy. EEG is non-invasive and inexpensive; therefore it would be very efficient and effective screening tool to detect MCI patients for early diagnosis of MCI.
Further studies should focus to determine new therapeutic approaches directed to selectively suppressing aberrant network excitability in the temporal lobe.
Conflicts of Interest
There are no conflicts of interests.
17972
References
- Foti PV,ReforgiatoRecupero AG, Girella D, Biondi E, Teriaca F, et al. (2003) The importance of Magnetic Resonance Imaging (MRI) in the diagnosis of hippocampal sclerosis. BollettinoSocietà Medico Chirurgica di Catania. Vol. LXXII. Gennaio.
- Höller Y, Trinka E (2014) What do temporal lobe epilepsy and progressive mild cognitive impairment have in common? Front SystNeurosci.
- Calabrese V, Guagliano E, Sapienza M, Panebianco M, Calafato S, et al. (2006) Redox regulation of cellular stress response in aging and neurodegenerative disorders: role of vitagenes. Neurochemical Research.
- Kashefpoor M, Rabban H, Bareatain M (2016) Automatic diagnosis of mild cognitive impairment using electroencephalogram spectral features. J Med SignlsSens6: 25-32.
- Noebels JL (2011) A perfect storm: Converging paths of epilepsy and Alzheimer’s dementia intersect in the hippocampal formation. Epilepsia52: 39–46.
- EtindeleSosso FA, Raouafi S (2016) Brain disorders: Correlation between cognitive impairment and complex combination. Mental Health in Family Medicine12:215-222.
- Griffith HR (2006) Older adults with epilepsy demonstrate cognitive impairments compared with patients with amnestic mild cognitive impairment. Epilepsy Behav 8:161–168.
- Altman DG (1991) Practical statistics for medical research. London: Chapman and Hall.
- Sheskin DJ (2004) Handbook of parametric and nonparametric statistical procedures. (3rdedn). Boca Raton: Chapman & Hall /CRC.
- Dauwels J, Vialatte F, Cichocki A (2010) Diagnosis of Alzheimer's disease from EEG signals: Where are we standing? Curr Alzheimer Res7:487–505.

