Keywords
Intensive Care Unit, admissions, outcome, reasons, length of stay.
Introduction
The ICU is characterized as the hospital in to a hospital. The intensive care hospitalised patients with reversible illnesses that can be improved with detail follow-up and complicated treatments. From practical side there are cases in the ICU where all treatments included the most complex and costly cannot change the situation.
An intensive care unit (ICU) is a continuously busy ward in which critically ill patients are on life support treatment under intensive monitoring. Doctors, nurses and technicians vigilantly work on the patients and handle the life support equipment, pipeline..and..monitors [1,2]. Combination of expensive advanced technologies and increasing frequency of older and more acutely ill patients in ICU has resulted in more expensive care. In the recent years healthcare system has come under increasing scrutiny so there is a need to monitor and assess the quality of ICU care. Mortality is a major but relatively insensitive measure of ICU quality, even with severity adjustments [3].
In 1854, Florence Nightingale left for the Crimean War, where the necessity to separate seriously wounded soldiers from less-seriously wounded was observed. Nightingale reduced mortality from 40% to 2% on the battlefield, creating the concept of intensive care. In 1950, anaesthesiologist Peter Safar established the concept of "Advanced Support of Life," keeping patients sedated and ventilated in an intensive care environment. Safar is considered the first intensivist. In response to a polio epidemic , Bjørn Ibsen established the first intensive care unit in Copenhagen in 1953. The first application of this idea in the United States was pioneered by Dr. William Mosenthal, a surgeon at the Dartmouth-Hitchcock Medical Center [4].
Recent advances and increasing complexity of modern medicine in patients with a high level of physiological compromise and significant co-morbidities led to the development of ICU during the last 50 years [5,6]. However, this advancement in the care of critically ill patients has been associated with a huge increase in health expenditure. As health resources become increasingly constrained, it is imperative that efficient utilization of expensive resources such as intensive care becomes a priority and should be optimized without compromising the quality of care delivered to critically ill patient [7].
Moribund/terminal patients are generally not brought to ICU as they are kept in wards on simple ventilators with basic modes. Nowadays, in Greece the Patient-nurse ratio is fixed at three nurses for five patients, with an aim of keeping it as one for one. For reasons of efficiency and economy, smaller hospitals generally have a combined medical and surgical ICU. The smallest hospitals also combine coronary care with intensive care in a single unit. Larger hospitals, particularly teaching hospitals, often have separate general medical and surgical units as well as separate subspecialty units for specific types of medical problems, e.g., cardiac surgery and respiratory care.
Usual deseases which are faced in the ICU concern the following: the confrontation and recovery of each type of shock, the acute respiratory failure, multiple trauma patients, failure from various organic systems (cardiovascular, acute kidney failure, poisonings, environmental damage, serious infections, decay, chirurgically orthopaedic / neurosurgical and urgent neurological incidents, post surgical complications, heart operation, transplantations etc [8].
With this background, the present study was conducted to do an audit of reported critical events during intensive care stay and to develop a critical event reporting system in the ICU of our hospital.
Aim
The aim of this study was to determine the incidence, patient characteristics, reasons and outcome of admissions in the general adult ICU of the General hospital of Heraklion “Venizeleio - Pananeio” in Crete.
Material and Method
This is a retrospective study conducted in “Venizeleio - Pananeio” in Crete during the period January 1st 2009 to June 30th 2009. The hospital is a 500-bed general hospital that is run primarily by a nursing team. It has no specific ICU policy or protocols. The hospital provides a health service to a total population of 291.225. For each patient, baseline demographic data, together with details on diagnosis, reasons of admission-death, length of stay in the ICU, and final outcome were collected from intensive care unit logbook and patients medical records. On occasion, it also accepted coronary care patients.
Results
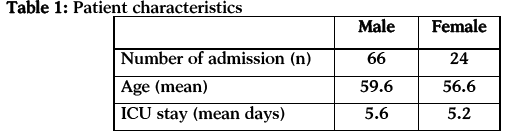
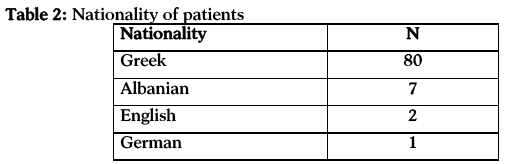
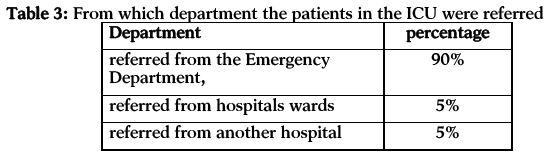
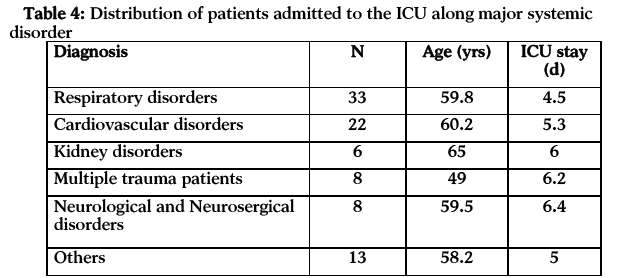
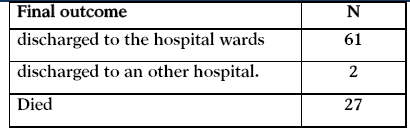
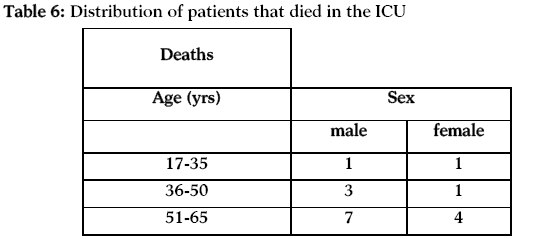
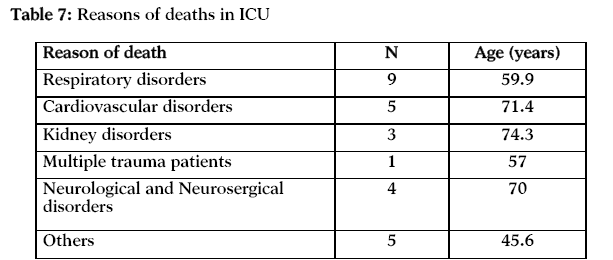
There were 90 admission during the study period. From the patients 66 were male and 24 were female patients. About 90% were referred from the Emergency Department, 5% were referred from hospitals wards and 5% were referred from an other hospital . The distribution of patients by race was 80, 7, 2, 1 for Greek, Albania, English and German. Admission rates were maximum in patients with problems by the Respiratory system (n=33) with mean age 59,8 and ICU stay 4.5. 22 required ICU admission because of a Cardiovascular disorders with mean age 60,2 and ICU stay 5.3. Also, 6 patients had an admission in the ICU because of kidney disease with mean age 65 and ICU stay 6, 8 patients were multiple trauma patients with mean age 49 and ICU stay 6.2 , 8 patients were Neurological and Neurosergical patients with mean age 59.5 and ICU stay 6.4 and 13 had an admission in the ICU for other reasons with mean age 58,2 and ICU stay 5. The patients’ mean age for all the reasons of the admissions was 59.6 for men and 56.6 for women. 61 patients discharged from the ICU to the hospital wards, 27 died and 2 patient discharged to an other hospital. Patients that died in the age of 17-35, 1 was a man and 1 was a woman. Moreover, in the age of 36-50 that died, 3 were men and 1 was a women. In the age of 51-65, 7 were men and 4 were women. Also, in the age of 66-87, 7 were men and 3 were women. From the 90 patients, 27 died. From the patients that died 18 were men and 9 were women. The most patient died because of problems by the respiratory system with mean age 59.9. Also, 5 patient died because of cardiovascular disorder with mean age 71,4. Moreover, 3 patients died because of kidney disorders with mean age 74,3. 1 patient was a multiple trauma patient in age of 57, 4 patients that died were patients with Neurological and Neurosurgical disorders with mean age 70 and 5 patients died because of others reasons with mean age 45,6.
Discussion
In the face of the increasing demand of intensive care services, as well as the high cost of such services systematic steps must be undertaken in order to ensure optimal utilisation of these resources. Admission to an intensive care facility is premised on the view that technologically advanced, competent care made available to the critically ill favourably influences the outcome of such illness [9].
In this study, 90 patients admitted to the ICU. The high ratio of medical admissions to our ICU is due to the fact that a cardiac care is not available in our hospital therefore patients with acute cardiac disorders are admitted to the ICU. If this group of patients is admitted to cardiac care unit of another general hospital, the percentage of medical admission to our ICU will be comparable to medical admissions of other hospitals. About 90% were referred from the Emergency Department, 5% were referred from hospitals wards and 5% were referred from another hospital.
From them 66 were men and 24 were women. Studies of ICU patients demonstrate a remark-ably consistent male to female ratio of about 3:2. In the general, the ratio represents the prevalence of serious disorders from the respiratory system among males and females under the age of 70. Above that age, female representation in ICUs increases [10-12].
33 medical admissions were due to respiratory disorders. 22 patient were hospitalized in the ICU because of cardiovascular disorders. Further analysis for the distribution of patients among medical disorders is shown in Table 4. As Chassin emphasized, medical ICUs treat a wide spectrum of illnesses, any specific disease represents a very small promotion of the total number of diseases that are present [13]. Similar findings have been described for mixed ICUs [14]. Even respiratory ICUs treat a variety of primary diseases [15]. Studies of ICU patients that had taken part in American shows that the main reasons for admission in ICU are acute reversible disease for whom the probability of survival without ICU intervention is low, but the survival probability with such interventions is high. Common clinical examples include the patient with acute reversible respiratory failure due to drug overdose, or with cardiac conduction disturbances resulting in cardiovascular collapse but amenable to pace-maker therapy. Moreover includes as second reason for admission in a mixed ICU the postoperative trauma patients. Also a third reason is the acute myocardial infarction [16].
In the present study the average length of stay in the ICU was 5.6 per men and 5.2 per women compared to 4-6 days per patient in the UK and the USA [17,18]. The reason for this variation is simply due to improper selection of patients for intensive care in our unit and the involvement of the junior doctors in admitting patient to the ICU. These patients have affected our average length of stay because they hospitalized in the ICU less than a day. Therefore, patients should be referred and followed by the most senior member of staff responsible for their care. The mean length of stay in a ICU for all Medicare ICU patients in 1980 in USA was 4.2 days [19]. The average length stay in USA hospitals has been notably stable over the past 15 years. In a study of 1.001 consecutive patients in a ICU, Pessi [20] found that 27 percent stayed less than 2 days, while 15 percent stayed longer than 10 days. In one ICU, Chassin 21 found that 10 percent stayed longer than 10 days. ICU stays of more than a month are not uncommon.
From the current study was resulted that 27 patients died which is a big percent. The most of them (n=18) were men and the main reason of their death was respiratory disorders (n=9) with a mean age 59.9. Further analysis for the distribution of patients that died is shown in Table 6,7 . Most studies have looked at mortality in the ICU or in the hospital as a measure of the efficacy of ICU care. These studies shows definite reduction in mortality for conditions as respiratory failure treated with ventilators, status asthmatics and emphysema, non-hemorrhagic strokes, severe burns, postoperative trauma patients. Other studies shows no reduction in strokes, drug overdose, head injuries with coma, Pulmonary edema, Pneumococcal bacteremia and Postperative acute renal failure [22].
Conclusions
In summary, the findings of the present study shows that respiratory problems are the major reason for an ICU admission.The high ratio of medical admissions to our ICU is due to the fact that a cardiac care is not available in our hospital therefore patients with acute cardiac disorders are admitted to the ICU. Patients that are men and in the age 51-87 are at greatest risk of an ICU admission. The average length of stay in the ICU is 5.6 per men and 5.2 per women. Moreover, the first half-year period of 2009 was realised high mortality rate and the main reason was problems by the respiratory system.
As health resources become increasingly constrained, it is imperative that efficient utilization of expensive resources such as intensive care becomes a priority and should be optimized without compromising the quality of care delivered to critically ill patient. Two main goals of the ICU are to help the dying have a dignified death and to save the salvageable.
ANNEX

5308
References
- Cooper JB, Newbower RS, Long CD, McPeek B. Preventable Anesthesia mishaps: A study of human factors. Anesthesiology 1978; 49(6):399-406.
- Cooper JB, Newbower RS, Kitz RJ. Analysis of major errors and equipments failure in anesthesia management: Considerations for prevention and detection. Anesthesiology 1984; 60(2):34-42.
- Angus DC. Grappling with intensive care unit quality-Does the readmission rate tell us anything? Crit Care Med 1998; 26(2):1779-80.
- "Remembering Dr. William Mosenthal: A simple idea from a special surgeon". DartmouthMedicine.https://dartmed.dartmouth.edu/spring04/html/vs_mosenthal.shtml. Retrieved on 2007-04-10.
- Society Critical Care Medicine Guideline Committee. Guidelines for intensive care unit admission, discharge, and triage. Crit Care Med 1999; 27(2):633-638.
- Coggin R, Parkin CH, DeCossart L. Use of a general surgical high dependency unit in a strict general hospital: The first 10 years, J R CollSurgEdinb 1998; 43(3): 381-384.
- Weissman C. Analyzing intensive care unit length of stays data: Problems and Possible solutions. Crit Care Med 1997; 25(2):1594-1600.
- Coggin R, Parkin CH, DeCossart L. Use of a general surgical high dependency unit in a strict general hospital: The first 10 years, J R CollSurgEdinb 1998; 43(4): 381-384.
- Thibault GE, Mulley AG, Barnett GO, Goldstein RL, Reder VA, Sherman EL, Skinner ER. Medical intensive care: Indications, interventions and outcomes. N Engl J Med 1980; 302(1):938-942.
- Thibault GE. “The Medical Intensive Care Unit: A Five-Year Perspective.” Ch.2 in Major Issues in Critical Care Medicin, J, Parrilo and S.M. Ayes (eds) (Baltimore, MD: Williams & Wilkins, 1984.
- Bell JA, Bradley RD, Jenkins BS, Spencer GT. “Six Years of Multidisciplinary Intensive Care” Brit. Med. 1974;1(2):483.
- Crockett GS, Barr A. “An Intensive Care Unit: Two Years Experience in a Provincial Hospital ” Brit. Med. J, 1965; 2(2):1173.
- Chassin MR. “Costs and outcomes of medical intensive care,” Medical Care 1982; 20(2):165.
- Cromwel J, Kanak JR. “The Effects of Prospective Reimbursement Programs on Hospital Adoption and Service Sharing,” Health Care Finam. Rev. 1982; 4(2):67.
- Bartlett RH, Gazzaniga AB, Wilson A F, Medley T, Wetmore N. “Mortality Prediction in adult Respiratory Insufficiency”, 1975; 67(6):680.
- Reichel W. “The Continuity Imperative,” editorial, J, A.M.A. 1981; 246(18):2065.
- Weissman C. Analyzing intensive care unit length of stays data: Problems and possible solutions. Crit Care Med,1997; 25(9): 1594-1600.
- Sprung CL, Geber D, Eidelman LA, Baras M, Pizov R, Nimrod A, et al. Evaluation of triage for intensive care admission. Crit Care Med 1999; 27(2):1073-1079.
- Raffin TA. Intensive care unit survival of patients with systemic illness. Am Rev Resp Dis 1989;23(1):28-35.
- Pessi TT. “ Experiences Gained in Intrnsive Care of Surgical Patients: A Prospective Clinical Study of 1.003. Consecutively Treated Patients in a surgical intensive care unit.” Ann. Chir. Gynecol. Fenn, 1973; 62(2):185.
- Chassin M RM. “Costs and Outcomes of Medical Intensive Care.” Medical Care 1982; 20(2):165.
- Nunn JF, Milledge J S, Singaraya J. “Survival of patients ventilated in a intensive care unit,” Brit. Med. 1979; 41(1): 1525.

