Keywords
Long acting and permanent methods; Involvement of men; Southern Ethiopia
Background
Family planning is instrumental to reduce poverty, promote economic growth, increase female productivity and improve child and maternal health. Decreasing women’s time on child rearing and increasing their enrolment in productivity and education enhances their social status and decision making power [1]. In Africa, men generally desire larger families than their wives. Gender norm, societal cultural expectations on behaviors of females and males often bound women’s ability to negotiate in contraceptive use and active participation in efforts to improve their livelihoods [2].
Though Long Acting and Permanent Methods (LAPMs) are safe and convenient, their utilization is low. Studies in Sub Saharan Africa (SSA) between 2003 and 2005 showed that in each of the nine countries including Ethiopia, fewer than 7 percent of the women were using LAPMs [3]. In Ethiopia utilization of female sterilization, intrauterine device (IUCD) and implant were only 0.5 %, 0.3 % and 2.9 %, respectively [4]. A study by performance monitoring and accountability (PMA) 2020 project revealed that the prevalence of female sterilization, IUCD and implant increased to 15.9 %, 1.9 %, and 0.4 %, respectively in 2014 though study women were recruited from mobile network accessible areas [5]. Family planning program planners focused their attention largely on women. Even though women bear the physical, psychological and emotional strain of pregnancy and childbirth, fertility and contraception did not solely refer to the female population. Thus, the social, cultural and economic roles of men who are dominant not only in decision making within the family but also at community level have been overlooked. Most family planning programs gave less attention to the understanding of men’s role in the effective and steadfast utilization of contraceptives [6,7].
According to Ethiopian traditions, wives in most ethnic groups, consider their husbands as overall heads of the household which could be related to religious teachings and cultural norms that favored Ethiopian men, as decision makers both at family and community levels [8]. Thus, the male dominated family structure could have significant contribution in matters of reproduction and has great influence on a couple’s family planning decisions and use. However, Ethiopia has made several important international commitments to improve the sexual and reproductive health rights of its entire population through the Millennium Development Goals. Scaling the use of LAPMs may play a critical role in meeting these international goals [3]. The purpose of this study is therefore to assess the role of males’ involvement in the use of LAPMs. In particular, the study attempts to measure the use of LAPMs by men and their spouses and its associated factors in South Western Ethiopia.
Methods
A community based cross sectional study with a mix of quantitative and qualitative methods was conducted from January to March 2014 in Mizan-Aman town in Southern Nations Nationalities and People Region (SNNPR) of Ethiopia. The total population of the town according to the 2007 census was 34,080, of which 18,138 were males. According to the town health office, there were five Kebeles with a total of 9,145 households. There were one general hospital, one health center and 5 health posts all run by the government. On the other hand, there were 9 private clinics (of which 5 are medium clinics) and 8 drug venders.
A sample of 554 currently married men aged 20–64 years were recruited from usual residents of the town who stayed for at least six months in the study area. The sample size was determined using single population proportion formula. It is computed by considering 67.6 % of men supporting LAMPS from a previous study (36); margin of error of 5 %, and 95 % confidence level. Then, a 10 % non-response rate and design effect 1.5 were considered to obtain the total sample size of 554. Out of the total 5 small administrative units (Kebeles) in Mizan-Aman town, 3 Kebeles were selected by lottery method. The total sample size was then allocated using probability proportional to size (PPS) of households in the selected Kebeles. Study participants were selected from households from each selected Kebele using systematic random sampling. The sampling interval was obtained by dividing the total household in each selected Kebele by the allocated sample. The first household was then chosen at the center of each Kebele by a lottery method as a starting point, and then data collectors were going in the right direction from the first chosen household until the required sample size for the Kebele was obtained. In case the eligible man in the selected household is absent the next household was considered. If more than one eligible man was identified in the selected household one of them was selected randomly for the interview.
For the qualitative method, 8 key informants were included in the interview. The sample size was determined based on saturation of ideas. Two health extension workers, one program officer, 3 currently married men, and 2 women were involved in the in depth interview.
The questionnaire was adapted from related studies including the Ethiopian Demographic and Health Survey (EDHS). The quantitative and qualitative data collection instruments were first prepared in English and then translated to Amharic. To check consistency of the translation; back translation to English was done by another person. The quantitative questionnaire was pre-tested on 5 % of the sample in a similar population with the same context. Based on the findings of the pretest, questions were modified. The structured closed ended questionnaire drafted using the local language was used for data collection. Five males who had completed grade 12 were recruited as data collectors. Two nurses who had diploma supervised the data collection. Training was given on principles of data collection and study instrument for two days. Data were collected by face-toface interview. Completed questionnaires were checked daily for completeness, legibility and consistency.
Data entry and cleaning were done using Epi Info version 3.5.1. Cleaned data were exported to SPSS Version 21 for analysis. Descriptive statistics were computed and presented using Tables. The main outcome variable, LAPMs use, is binary in nature and it is labeled as “1” when currently married men or their spouse reported its use at the time of the study or “0”, otherwise.
Bi-variate analysis was used to determine the association between different factors and use of LAPMs while multivariable logistic regression was employed for those variables which were significant at the bivariate level to identify factors associated with the use of LAPMs after controlling confounding factors. The association between the dependent and independent variables was determined using odds ratio (OR) with 95 % confidence interval (CI) in binary logistic regression model.
The in depth interview was conducted at a convenient place and time for interviewees. The collected data were transcribed and translated at the same day on which the interview was held. Transcripts were checked against notes taken to ensure quality. Open code software version 3.6 was used for coding and categorization. Thematic content analysis was then applied. Finally, findings were triangulated with the quantitative result during write up.
Ethical clearance was sought from the Research Ethics Committee of the School of Public Health, College of Health Sciences in Addis Ababa University. Written permission letter was also obtained from Bench- Maji Zone Health Office. Oral informed consent was obtained from each study participant. Privacy of respondents and confidentiality of information were kept throughout the study.
Results
A total of 521 currently married men were interviewed for the quantitative study with the response rate of 94.1%. The remaining 33 were nonresponsive, so all the analysis was done on 521 individuals. The mean age of the participants was 37 (± 9 SD) years. Majority of the participants were Bench (37 %) by ethnicity and Orthodox (44.5 %) by religion. One hundred thirty nine (30.2 %) of respondents and 121 (30.4 %) of their wives attained secondary school (Figure 1). while 60 (11.5 %) of the participants and 123 (23.6 %) of their partners could not write and read at the time of the study. One hundred ninety two (36.9 %) of respondents’ household earned a monthly income of 2500 Ethiopian birr (ETB) or more, while 163 (31.3 %) of the respondents’ household got a monthly income which was less than 1200 ETB, with mean and SD, 2150.5 ± 1410.9. nearly half, 248 (47.8 %) of the study participants were married at the age of 20-24 with the mean age at first marriage of 22.86 + 3.7 (SD). The majority 449 (86.2 %) of study men had at least one child at the time of the study. The average desired number of children was 4.4 per man. Among the study twenty seven percent of the respondents preferred to have the next child within 2 years, while, 41 %, and 32 % of the respondents wished to have their next child between 2 and 3 years and after 3 years, respectively. More than half 311 (59.7 %) of the study participants wished to have (another) children, from those, the majority 189 (60.8 %) wished to have 1-2 children, while 122 (39.2 %) of the respondents wished to have more than five children. Sixty two percent of the study participants (324) had discussions with their wives on the number of children that they want to have, while the rest did not to do so. Likewise, 57.2 % of study participants made the decision to have more children or to stop jointly, whereas, 36.5 % left the issue to God /Allah (Table 1).

Figure 1: Educational status of the study subjects and their wives, in Mizan-Aman Town/District, SNNPR, Ethiopia, 2014(n=521).
Table 1: Frequency distribution of Socio -demographic and Reproductive characteristics of the study subjects in Mizan-Aman Town/District, SNNPR, Ethiopia, 2014 (n=521).
| Variable |
Frequency |
Percent (%) |
Ageof respondents: 20-30
31-40
41-50
51-64 |
178
169
122
52 |
34.2
32.4
23.4
10 |
Ethnicity: Bench
Amahara
Kefa
Oromo
Tegri
Others** |
194
110
94
52
41
30 |
37.2
21.1
18.0
10.0
7.9
5.8 |
House hold monthly income: ≤1199
1200-2499
2500
With Mean & SD |
163
166
192
2150.5 ± 1410.9 |
31.3
31.9
36.9 |
Age at the first marriage: ≤ 19
20-24
25-29
≥30 |
91
249
156
25 |
17.5
47.8
29.9
4.8 |
Age at the first child (N=449): ≤19
20-24
≥25 |
16
203
230 |
3.6
45.2
51.2 |
No of currently living children (n=449: <2
3-4
≥5 |
201
160
88 |
44.8
35.6
19.6 |
The respondents Desired no of children: 1-2
3-4
≥5 |
93
252
176 |
17.9
48.4
33.8 |
Discussion with wife on the No of children to have:
No Yes |
197
324 |
37.8
62.2 |
** Wolita, Gurage
Comprehensive knowledge on modern contraceptive methods
Most 508 (97.5 %) of them reported that they heard about modern family planning, while only 394 (78 %) of them had awareness about LAPMs. The most commonly known modern family planning method reported by study participants was Pills 508 (97.5 %), followed by injectables 506 (97 %). But Female condom 212 (40.7 %), Female Sterilization 156 (30 %), and male sterilization 149 (29 %) were mentioned less frequently (Table 1). Likewise among LAPMs, implants 388 (98.5 %) and IUCD 349 (88.6 %) were mentioned mostly, while male sterilization 147 (37.3 %) was the least known reported methods. Among those who had ever heard about LAPMs, the majority 344 (93.1 %) heard LAPMs through the mass media in the past 12 months. With regards to the source of information about LAPMs, 87 % got from health institution, while only 30 (7.6 %) got the information form NGOs (Table 2). On the other hand using a composite knowledge score, nearly a third 172 (33 %) of them had high knowledge about LAPMs, whereas 211 (40.5 %) and 138 (26 %) of them had low and moderate level of knowledge about LAPMs respectively.
Table 2: Frequency distribution of the study subjects’ Knowledge towards modern contraceptives in Mizan-Aman town, South Western Ethiopia, 2014.
| Variable |
Frequency |
Percent (%) |
| Types of modern contraceptives Known (n=521) |
|
|
| Pills |
508 |
97.5 |
| Injectables |
506 |
97 |
| Implant |
381 |
73.1 |
| IUCD |
362 |
69.5 |
| Male sterilization |
149 |
29 |
| Female sterilization |
156 |
30 |
| Male condom |
381 |
73.1 |
| Female condom |
212 |
40.7 |
Ever heard about LAPMs (n=508)
No
Yes |
114
394 |
22.4
77.6 |
| Source of information for LAPMs (n=394) |
|
|
Health institutions
Family members
Friends
Media
NGO |
344
71
126
292
30 |
87.5
18
32
73.9
7.6 |
| Type of LAPMs known (n=394) |
|
|
| IUCD |
349 |
88.9 |
| Implant |
388 |
98.5 |
| Female sterilization |
148 |
37.6 |
| Male sterilization |
147 |
37.3 |
Exposure to LAPMs message (n=394)
No
Yes |
27
367 |
6.9
93.1 |
More than half 281 (54 %) of men approved the use of LAPMs. Among those who did not support the use of LAPMs, 118 (49.2 %) mentioned religious prohibition, whereas, 66 (27.5 %), 55 (22.9 %), 25 (10.4 %), and 22 (9.2 %) reiterated the need for more child, fear of side effect, rejecting it, health problems and culture respectively as reasons not to support the use of LAPMs (Figure 2). The attitude of the community towards LAPMs is kind of mixed as elucidated by a 35 years old female in depth interviewee: "Stopping of child bearing by using FP is considered as sin. Few individuals said that it is the same as killing a person. But this is not good, in my opinion if we do not feed, dress, and educate them properly, it is better to have few children."
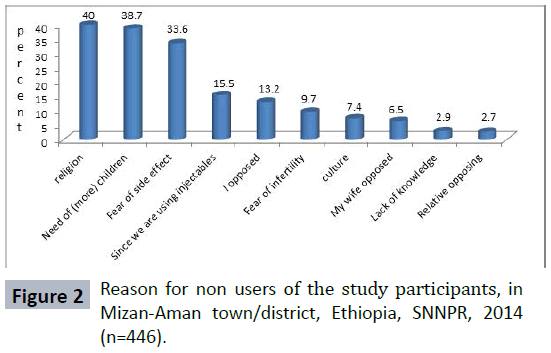
Figure 2: Reason for non users of the study participants, in Mizan-Aman town/district, Ethiopia, SNNPR, 2014 (n=446).
The respondents were also asked about their agreement, whether male sterilization could cause sexual impairment /impotence. And more than half 307 (59.2 %) were not sure, whereas 15 (2.1 %), 120 (23 %), 69 (13.3 %), and 10 (1.9 %) strongly disagreed, disagreed, agreed, and strongly agreed respectively. Regarding to their attitude, 179 (34.4 %) had unfavorable attitude, while 130 (25 %) had favorable attitude and the rest 212 (40.7 %) were indifferent.
Current use of long acting and permanent contraceptive methods
LAPMs have been used by 75 (14.4 %) of spouses of study participants in their life time while only 60 (11.5 %) of them used it during the study period. However, none of the study men used permanent methods themselves. Currently, the most commonly used methods include implant by 51 (85 %), IUCD 9(15 %) of the respondents, but there is no one who had permanent methods (female or male sterilization) in the study area (Table 3).
Table 3: Frequency distribution of Current utilization of LAPMs among married men aged 20-64 years or their spouse in Mizan-Aman town/ district, SNNPR, Ethiopia, 2014 (n=521).
| Variable |
Frequency |
Percent (%) |
Ever user: No
Yes |
446
75 |
85.6
14.4 |
| Currently are you using or stopped? (n=75) |
|
|
| Stopped |
15 |
20 |
| Using |
60 |
80 |
| Types of LAPMs that are Currently used ( n=60) |
|
|
| Implant |
51 |
85 |
| IUCD |
9 |
15 |
| Whose choice isthe current LAPM ( n=60) |
|
|
| My wife |
10 |
16.7 |
| Myself |
7 |
11.7 |
| Both of us |
43 |
71.7 |
| Who made the decisionon LAPMS that your wives used currently? (n=60) |
|
|
| My wife |
5 |
8.3 |
| Myself |
5 |
8.3 |
| Both of us |
50 |
83.3 |
Discussions about LAPMs in the last 12 months with their wives.No
I do not remember
Yes |
322
28
171 |
61.8
5.4
32.8 |
| Whose idea was accepted during discussion n=171 |
|
|
| Mine |
75 |
37.7 |
| my wife/partner |
80 |
40.2 |
| Both of us |
44 |
22.1 |
| Responsibility of male in LAPMs utilization |
|
|
| Supportwifeto use |
282 |
54 |
| Usethe methodsby themselves |
90 |
17.3 |
| Allocate budget for it |
124 |
23.8 |
| Support in choreso as female use LAPMs |
185 |
35.5 |
| Discussion with wife about utilization |
358 |
68.7 |
| Know the advantages and tell the partner/wife |
367 |
70.4 |
| Have no role |
47 |
9.2 |
Regarding to the decision on current use of LAPMs, 50 (83.3 %) of respondents made the decision jointly, while only 8.3 % of the respondents made the decision by themselves. When they were asked on the roles of males in the use of LAPMs, the majority 367 (70.4 %) of the respondents indicated that the role of the male should be to understand the advantages of LAPMs and inform their wives and discuss with them on the possibilities of using LAPMs. Whereas, 90 (17.3 %) of study participants indicated that they had to use the methods by themselves (Table 2).
The majority 446 (85.6 %) of spouses of study participants were non-users of LAPMs. Various reasons were given during the interview for not using LAPMs. Of those, religion, desire to have more children, fear of side effects, and respondents’ opposition were the most important reasons that were reiterated by 179 (40 %), 172 (38.6 %), 149 (33.4 %), and 59 (13.2 %) of the study participants, respectively. This is further augmented by the in depth interview when a 31 years old male participant described the situation as: "In our community the usual understanding is, when the child is born it is not born only with the mouse but also with foot and hand, so s/he can do and live by his own and when we got old s/he may help us. If you have only one child s/he may pass away so it is better to have more children."
Another factor that hinders the use of LAPMs is culture. Most participants indicated that culture has a significant role in the use of reproductive health services including family planning methods. For instance, a forty seven years old male in depth interviewee mentioned that: "In our community, one male can marry up to seven wives. This is an accepted norm for the rich in the area. One is said to be a rich man, when he had more than two wives and many children. Those thoughts hinder the society from utilization of FP. So education is important to change the society's attitude". Another forty 37 years old male in depth interviewee elucidated that "IUCD may migrate to the brain, and make women crazy, then finally it will kill them, IUCD or implant prevents from doing routine /daily work, and even the method had psychological, mental, and physical impact on the child who will be born after utilization ."
Factors associated with the current utilization of LAPMs
The result of binary logistic regression analysis on the association of socio-demographic and reproductive health characteristics of study participants with the current utilization of LAPMs showed that men in the age groups of 20- 30 and 31-40 years were 2.2 and 1.7 times respectively more likely to use LAPMs than those who were aged 41 years or older (COR=2.2, 95 % CI, 1.1- 4.5 & COR=1.7, 95 % CI, 2.8-3.5) (Table 4).
Table 4: Factors associated with the current utilization of LAPMs among married men or their spouses in Mizan-Aman Town/District, SNNPR, Ethiopia, 2014 (n=521).
| Variable |
Utilization of LAPM |
COR(95%CI) |
AOR(95%CI) |
| No |
Yes |
| Age group of the respondent |
|
|
|
|
| 20-30 |
151 |
27 |
2.21 (1.10-4.45)* |
0.63(0.26-1.54) |
| 31-40 |
149 |
20 |
1.66 (2.80-3.46)* |
0.96(0.39-2.38) |
| >41 |
161 |
13 |
1 |
1 |
| Wives educational status |
|
|
|
|
| No education |
117 |
6 |
1 |
1 |
| Primary school |
118 |
20 |
3.31(1.28-8.52)* |
0.86 (0.263-2.77) |
| Secondary school |
105 |
16 |
2.97 (1.11 -7.87)* |
0.73(0.21-2.52) |
| Higher education |
121 |
18 |
2.90(1.11-7.56)* |
|
| The respondents desired no of children |
|
|
|
|
| 1-2 |
77 |
16 |
3.12(1.38-7.03)* |
4.13(0.86-19.87) |
| 3-4 |
219 |
33 |
2.26(1.11 -4.61)* |
1.11(0.42-2.98) |
| ≥5 |
165 |
11 |
1.00 |
1.00 |
| Wivesoccupation |
|
|
|
|
| House wife |
239 |
19 |
1.00 |
1.00 |
| Government employee |
102 |
17 |
2.10 (1.05-4.20)* |
1.60(0.56-4.55) |
| Private employee |
42 |
10 |
3.00 (1.30-6.90)* |
2.32(0.80-6.91) |
| Student & Others |
78 |
14 |
2.26(1.08-4.71)* |
1.82(0.73-4.56) |
| Discussion with wife/ wiveson the no of children to have |
|
|
|
|
| No |
191 |
6 |
1.00 |
1.00 |
| Yes |
270 |
54 |
6.37 (2.69-15.10)* |
3.05(1.01-9.18)* |
| Ever heard about LAPMs |
|
|
|
|
| No |
99 |
5 |
1.00 |
1.00 |
| Yes |
338 |
55 |
4.10(1.45-11.59)* |
0.32 (0.02-4.28) |
| Exposed to message through the mass media about LAPMs in the last 12 month |
|
|
|
|
| No |
149 |
5 |
1.00 |
1.00 |
| Yes |
312 |
55 |
5.23(2.06-13.40)* |
2.57(0.26-25.43) |
| Supportingthe use of LAPMs |
|
|
|
|
| No |
235 |
5 |
1.00 |
1.00 |
| Yes |
226 |
55 |
11.44(4.50-29.09)* |
4.46(1.59-12.49)* |
| Knowledge about LAPMs |
|
|
|
|
| low knowledge |
201 |
10 |
1.00 |
1.00 |
| moderate knowledge |
121 |
17 |
9.41(3.08-28.78)* |
1.96 (0.62-6.20) |
| High knowledge |
139 |
33 |
5.42(1.79-16.41)* |
2.18 (0.72-6.66) |
| Attitude towards LAPMs |
|
|
|
|
| Unfavorable attitude |
170 |
9 |
1.00 |
1.00 |
| Indifferent way |
190 |
22 |
2.82 (1.25-6.37) |
1.25 (0.46-3.37) |
| Favorable attitude |
101 |
29 |
4.77 (2.28-10.00)* |
1.53(0.58-4.01) |
| Communication with wife/wives about LAPMs in the last 12 month |
|
|
|
|
| No |
336 |
14 |
1.00 |
1.00 |
| Yes |
125 |
46 |
8.83(4.69-16.63)* |
3.96(1.90-8.23)* |
| Going to health facility with wife/wivesto discuss about FP with health provider |
|
|
|
|
| No |
345 |
18 |
1.00 |
1.00 |
| Yes |
116 |
42 |
6.94 (3.84-12.53)* |
2.71(1.32-5.55)* |
| Who made decisioneither to stop/to have more children |
|
|
|
|
| Either husband/wife only |
29 |
4 |
3.14(0.90-11.09) |
4.13(0.86-19.87) |
| Both (husband and wife) |
250 |
48 |
4.37(2.02-9.46)* |
1.12 (0.42-2.98 ) |
| God /Allah |
182 |
8 |
1.00 |
1.00 |
| Birth orders (interval) |
|
|
|
|
| <2years |
128 |
13 |
1.00 |
1.00 |
| 2-3 years |
195 |
18 |
0.91(0.43-1.92)* |
0.60 (0.23-1.55) |
| Above three years |
138 |
29 |
2.01(1.03-4.15)* |
0.81(0.32-2.06) |
A strong association has also been observed between education of wives and current utilization of LAPMs in this study at the bivariate level. Men whose wives attained primary, secondary, and higher level of education were 3.3 ,3,and 2.9 times more likely to use LAPMs respectively, when compared to wives who could not read and write (COR = 3.3, 95 % CI: 1.3 - 8.5, COR = 3, 95 % CI: 1.1 - 7.9 and COR = 2.9, 95 % CI: 1.1 - 7.6). Besides, there was also statistically significant association between wives occupation and current utilization of LAPMs. Men whose wives were governmental employees, private employees, and students were 2.1, 3,and 2.3 times in that order more likely to use LAPMs when compared to those who were house wife (COR = 2.1, 95 % CI: 1.1 - 4.2, COR= 3, 95 % CI: 1.3 - 6.9 and COR = 2.3, 95 % CI: 1.1 - 4.7) (Table 4).
Men who had ever heard about LAPMs were 4.1 times more likely to use LAPMs than those who had not ever heard (COR = 4.1, 95 % CI: 1.5 - 11.6). Similarly those men who heard media messages on LAPMs in the last 12 month were 5.3 times more likely to use LAPMs, when it is compared with those who were not exposed to such messages about LAPMs in the last 12 month (COR = 5.3, 95 % CI: 2.1 - 13.4) (Table 4).
The study also showed that men who supported the use of LAPMs were 11.4 times more likely to use LAPMs than those who did not support the use of LAPMs. (COR = 11.4, 95 % CI: 4.5 - 29) Positive attitude towards LAPMs and knowledge about LAPMs by men were significantly associated with current utilization of LAPMs. For instance, men who had favorable attitudes towards LAPMs were 4.8 times more likely to use LAPMs than those who had unfavorable attitude (COR = 4.8, 95 % CI. 2.3 - 10). Likewise, men who had high and moderate knowledge of LAPMs were 3.1 and 5.4 times more likely to use LAPMs respectively than those who had low knowledge of LAPMs (COR = 9.4, 95 % CI: 3.1 - 28.8 & COR = 5.4 , 95 % CI: 1.8 - 16.4) (Table 4).
Men who reported a desired number of children of less than two and 3 - 4 in their life time were 3 and 2.3 times more likely to use LAPMs correspondingly when compared to those who desired five or more children(COR = 3.1, 95 % CI: 1.4 – 7 & COR = 2.3, 95 % CI: 1.1 - 4.6). And those men who wished to have the next children in the coming three or more years were 2.1 times more likely to use LAPMs than those who wished to have it within two years (COR = 2.1, 95 % CI: 1 - 4.2). As well, those who had discussed with their wives on the number of children they want to have, were 6.4 times more likely to use than those who did not discuss (COR = 6.4 95 % CI: 2.7 - 15.1) (Table 4).
A strong association was also found between discussion about LAPMs in the past 12 month and current utilization of LAPMs. Those who had discussion with their wives about LAPMs in the past 12 months were 8.8 times more likely to use LAPMs than those who did not have such discussion (COR= 8.8 (95 % CI: 4.7 - 16.6). Moreover, those who reported joint decision making to have another child or to stop child bearing were 4.4 times more likely to use LAPMs than those who said God/Allah knows (COR = 4.4, 95 % CI: 2 - 9.5).Besides to this, men who accompany their wives to health facilities to discuss about LAPMs with health providers were 7 times more likely to use LAPMs when compared to those who did not accompany their wives to health facilities (COR = 6.9 ,95 % CI: 3.8 - 12.5) (Table 4).
After controlling most demographic, social, economic and reproductive health characteristics of married men through the use of multivariate Binary Logistic Regression analysis, this study showed that discussion with wives on the number of children they want to have and about LAPMs in the last 12 months, accompanying wives to health facilities to discuss about FP with health provider, and supporting the use LAPMS were found to be strong and significant predictors of LAPMs utilization (Table 4). Specifically, married men who had discussion with their wives about LAPMs in the past 12 months were 4 times more likely to use LAPMs than those who had no discussion with their wives (AOR = 4 , 95 % CI: 1.9 - 8.2). Those who had discussed with their wives on the number of children they want to have were 3 times more likely to use LAPMs than those who did not discuss after controlling some confounding factors (AOR = 3.1, 95 % CI.1 - 9.2). Besides, married men who accompanied their wives to health facility to discuss about FP with health provider were 2.7 times more likely to use LAPMs compared to those who did not do it (AOR = 2.7, 95 % CI: 1.3 - 5.6). Likewise, married men who supported the use LAPMS were 4.5 times more likely to use LAPMs than those who did not support (AOR = 4.5 (95 % CI: 1.6 - 12.5) (Table 4).
Discussion
The results of this study revealed that the proportion of men who had low, moderate, and high knowledge were 40.5 %, 26.5 %, and 33 % respectively. In Ethiopian demographic and health survey of 2011 the level of awareness for female sterilization, male sterilization, IUCD, and implant was 46.8 %, 17.6 %, 27.5 %, and 63.5 % respectively. This indicates that there is an enhancement in the level of awareness about LAPMs which may be explained by spread of more information, education and communication to the community by media and village based Health Extension Workers (HEWs) whose main tasks are promotion of good health and prevention. Likewise, 25 %, and 34.4 % of men had favorable and unfavorable attitudes respectively. Though the increase is remarkable, it is a little bit derailing from the anticipation in our national reproductive health strategy (2006 - 2015) that aspired to reach a contraceptive prevalence rate of 60 percent by the year 2010 and couples’ approval of FP to 75 percent by 2015. The increase in contraception could be attributed to the fact that the government has given due attention to change communities' awareness and perception through mass media advertisement. Moreover, HEWs’ household level reproductive health service provision could have played paramount contribution.
This study also revealed that only 11.5 % of men’s wives were using LAPMs in the study area. This result is in line with that of a study done in Mekele Town and Wolita zone , which were 12.3 % and 12.2 % respectively [9,10]. However, it was higher than the study done in Goba Town, Bale Zone which was 8.7 % (36) and the EDHS 2011 finding of 4.2 % [4]. The qualitative result also underpins this result as one participants elucidated as, "in the previous time there were cultural and religious thoughts that hinders the use of LAPMs. And the individual was being proud by their high number of children. And even some considers their children as an asset. But now the community has altered their thoughts, because of community education". This may be explained by the increment of advertisement through mass media, and community mobilization by government and nongovernmental organization. The population pressure due to the high economic recession could also be one factor that may oblige individual to use LAPMs. And the role of HEW might not been forgotten.
The utilization rate of each method was 85 %, and 15 % for implant and IUCD respectively in this study. This is also in line with the study done in Mekele Town and Goba Town (25, 36). However, there were no one who used vasectomy (male sterilization) and tubal ligation (female sterilization) among the study population. The qualitative result also complemented this findings, one informant described the context as follows, "We heard about male and female sterilization, but there was no one who used it in our community, because we heard that such methods bring about total infertility and unwanted effects on health . So, these methods are not good." This may be explained by perceived side effects, low awareness, and misconceptions towards such methods by both the study participants and their spouses. The non reversibility of the method might also be another thing, which makes them to be frustrated and to have downbeat approach.
It also showed that there was statistically significant association between supporting of LAPMs use and its utilization in the study area. That is, men who supported the use of LAPMs were more likely to use LAPMS than their counterparts. This finding is in line with the previous studies conducted in other areas of the country [7,11-14] and outside of the country [13,15-17]. The qualitative results of this study also amplified this finding. One of the participants described the scenario as follows, "since men are heads of the family, they can influence and persuade their wives. Hence, the attitude of male towards use of LAPMS has to be changed, because they can without doubt change the attitude of their wives or even they can use the method by themselves." This might be the fact that lack of support from the husband not only hinders contraceptive use, but could also lead to premature termination of the use of LAPMs. And the respondents who accepted the use of family planning methods are more likely to ensure that their favorable attitude is decoded into high use of LAPMs.
Those who had discussed with their wives about LAPMs in the last 12 months were more likely to use LAPMs than those who did not have such a discussion. This finding is in line with another study done in Jima Town [14], and Wollega zone [18] and outside of the country [16,19-21]. However, this is tricky to justify because crosssectional studies cannot clearly show the direction of causation between communication and contraception use. In many cases, it is unclear whether communication, predicts contraception use, or the use of contraception enhances communication between couples. Similarly, men who had discussed with wives on the number of children they wanted to have were also more likely to use LAPMs than those who did not have the discussion. This finding is in agreement with studies done in other areas of the country [7,18] and outside the country [19,21]. This may be explained by the fact that partners who discussed with wives on the number of children that they wanted to have may have an opportunity to discuss about LAPMs. Partners may know how to express their desires and feelings without any fears, and easily make out his/her spouse’s attitudes and beliefs regarding to LAPMs. The partner may think that the other is not disparate to use, hence, he/she may not hesitate to discuss about LAPMs for fear of angering or annoying their spouse.
Men who had gone to a health facility with their wives to discus about FP with health providers were also more likely to use LAPMs when compared to those who had not gone. This finding is in line with the study conducted in Nigeria, which documented that when the husband accompany his wife to the health facility, his resistance to contraception was more likely to be broken and the couple was more likely to adopt the method [15]. This is may be due to the fact that those who had misconception and confusion towards LAPMs, and fear of perceived side effects of LAPMs could be cleared during the discussion with health care providers. In addition, those who are going to health facility to discus about FP with health providers are those who may have an intention to use and had good attitude towards FP use. Their behavior is translated easily into practice.
The qualitative results of this study showed that most of the decisions were made by men. This is in line with the study done in other parts of the country and elsewhere [2,7,18,22]. This indicates that men are more likely to influence household decision than their wives. This makes clear that males’ involvement in the utilization of LAPMs have a paramount role in decision making, supporting and encouraging of their wives to use LAPMs. Involving men in encouraging, communication and joint decision-making on issues like family size and LAPMs use can help them to exercise their responsibility and take in hand their concerns towards LAPMs use within their family and outside their family. Men who are aware of the benefits of LAPMs use can be motivated to play a key role in their families and their communities. This is supported by the study done in Cairo which stated that men had the authority for contraception decisionmaking. In reaction to men’s opposition to contraceptive use, women were observed to use covertly. And finally resulted with divorce as potential consequences of covert use when it was exposed to their husbands [22]. This augments the fact that involving men can lead to better outcomes including those specific to LAPMs knowledge, intra-spousal communication, and LAPMs use and its sustainability .
The study used a mixed design which helps to triangulate the quantitative findings with qualitative findings. However, cause and effect relationship was difficult to establish for the factors dealt in the study since it is cross-sectional study. Since this study included only men, the practice of their spouses might be different from what is measured by this study. Perceived social-desirability of responses rather than actual knowledge or practices could be response biases. So further research should be done including both females and males.
Conclusions
Awareness and support towards the use of LAPMs were 78 % and 54 % respectively. Utilization of LAPMs in the study area was small. That is only (11.5 %) of the respondents reported the use of LAPMs. Discussion with the partners on the number of children they want to have, and communication with the wives about LAPMs in the last 12 months were the most important factors that were influencing utilization of LAPMs in the study area.
Respondents' approval of LAPMs' utilization and accompanying spouses to a health facility to discuss about FP methods with health providers were also the other most important factors that enhances utilization of LAPMs in the town. Even if men did not use vasectomy, in cases of decision making, supporting and encouraging of their wives to use LAPMs, they played a valuable role. IUCD may migrate to the brain, and make them crazy, then finally it will kill, IUCD or implant prevents from doing routine / daily work, and LAPMs had psychological, mental, and physical impact on the child who would be born after utilization were commonly observed misconception in the study area.
Health professionals, including HEWs should continuously make easy the discussions between couples on the use of LAPMs and the number of children. The media should promote on the use of LAPMs to increase the attitude and involvement of males in the use of such methods. Consistent awareness creations should be provided by health service providers and the media to mitigate some of the myths and misconceptions related to LAPMs.
Competing Interests
There is no any competing interest.
Authors’ Contributions
KM carried out the conception and designing the study, performed statistical analysis and wrote the manuscript.
WM approved the design of the study, analysis, reviewing and editing the final draft of the manuscript.
Authors’ Information
KM (MPH in Epidemiology), lecturer at Mizan -Tepi University,
WM (PhD): Assistant Professor, School of Public Health, Addis Ababa University.
Acknowledgements
We thank School of Public Health in Addis Ababa University for financing the project. We would like to acknowledge Bench Maji Zonal Health Office for their cooperation in conducting this study. We are very grateful to the study participants for their willingness to participate in this study and to the field data collectors for their hard work and sincere contribution.
8705
References
- Elizabeth R, Nancy Y (2002) Making Mother Hood Safer: overcoming obstacles on the pathway to care. Population Reference Bureau, Washington DC, United States.
- Omar J, Roble S, Aditi K (2010) Constructive Men’s Engagement in Reproductive Health and HIV in Ethiopia, Facilitating Policy Dialogue. Health Policy Initiative, Task Order 1, United States.
- RC Macro. Unmet Need for Long-Acting and Permanent Methods in Sub-Saharan Africa. Measure DHS stat compiler.
- Addis Ababa (2012) Central Statistical Authority. Ethiopia Demographic and Health Survey 2011, Ethiopia.
- Addis Ababa (2014) University’s School of Public Health at the College of Health Sciences (AAU/SPH/CHS), In collaboration with regional universities, the Federal Ministry of Health, the Central Statistics Agency. KEY FAMILY PLANNING INDICATORS, PMA2014/ETHIOPIA.
- Hogan DP, Berhanu B, Hailemariam A (1999) Household organization, women's autonomy, and contraceptive behavior in southern Ethiopia.Stud Fam Plann 30: 302-314.
- Tsedeke T, Deressa W, Ali A, Davey G (2006) The role of men in contraceptive use and fertility preference in Hosanna Town, southern Ethiopia. J Health Dev 20: 152-159.
- Addis Ababa (2001) Central Statistical Authority. Ethiopia Demographic and Health Survey 2000, Ethiopia.
- Alemayehu M, Belachew T, Tilahun T (2012) Factors associated with utilization of long acting and permanent contraceptive methods among married women of reproductive age in Mekelle town, Tigray region, north Ethiopia.BMC Pregnancy Childbirth 12: 6.
- Meskele M (2013) Women's Attitude, Barriers and Intension to use Lonacting and Permanent Methods among short term users in Wolita Zone, Southern Ethiopia. MPH thesis, AAU.
- Berhane A, Biadgilign S, Amberbir A, Morankar S, Berhane A, et al. (2011) Men's knowledge and spousal communication about modern family planning methods in Ethiopia.Afr J Reprod Health 15: 24-32.
- Yemane B,Mekonnen E, Zerihun, Asefa G (1999) Perception of Fertility regulation in remote community, South Ethiopia. Ethiop J Health Dev13: 217-221.
- Bunce A, Guest G, Searing H, Frajzyngier V, Riwa P, et al. (2007) Factors affecting vasectomy acceptability in Tanzania.IntFam Plan Perspect 33: 13-21.
- Haile A, Enqueselassie F (2006)Influence of Women’s Autonomy and Husband’s Involvementon Couple’s Contraception UsE. Ethiop J Health Dev 20:145-151.
- Babalola S, John N (2012) Factors Underlying the Use of Long-Acting and Permanent Family Planning Methods in Nigeria: A Qualitative Study. The Respond Project Study Series: Contributions to Global Knowledge-Report ,No 5 New York: EngenderHealth/The RESPOND Project, United States.
- Farrokh M, Amir H, Homa A (2006) Socio-Cultural Factors Affecting Men’s Use of Family Planning Methods in Iran. Journal of Social Hciences & Humanities of Shiraz University 24: 9-16.
- Tawiah EO (1997) Factors affecting Contraceptive use in Ghana. Regional Institute for Population Studies, University of Ghana, Legon, Ghana. J Biosoc Sci 29:141-149.
- Yohannes T (2004) The role of men in family planning in a rural community of Western Ethiopia. Thesis. 23-42.
- Lasee A, Becker S (1997) Husband-wife communication about family planning and contraceptive use in Kenya. IntFam Plan Perspect 23:15-21.
- Kim Y, Marangwanda C, Kols A (1996) Involving Men in Family Planning. The Zimbabwe Male Motivation and Family Planning Method Expansion Project, 1993-1994 Baltimore, Johns Hopkins School of Public Health, Center for Communication Programs, United States.
- Lundgren R, Cachan J, Jennings V (2012) Engaging men in family planning services delivery: experiences introducing the Standard Days Method® in four countries.World Health Popul 14: 44-51.
- Jessica L (2008) Reaching the goals of Cairo: Male-involvement in Family planning Center for Global Health Initiative, United States.

