Feredun Azari * and Sunil Singhal
Department of Surgery, Hospital of the University of Pennsylvania, United States
- *Corresponding Author:
- Feredun Azari
Department of Surgery
Hospital of the University of Pennsylvania
United States
Received Date: February 14, 2021 Accepted Date: March 1, 2021 Published Date: March 08, 2021
Citation: Azari F, Singhal S (2021) Minimally Invasive Management of Challenging Left Sided Pulmonary Sequestration. Arch Can Res Vol.9 No.1:2.
24-year-old otherwise healthy female on birth control presents to the emergency department with recurrent coughing episodes, sudden onset shortness of breath, and unexplained back pain. After careful discussion with the patient, it appeared that she has had multiple respiratory symptoms initially attributed to her obstructive lung disease over the past two years. Initial laboratory workup revealed normal white blood cell count and chemistry panel.
Keywords
Sequestration; Congenital disease; Thoracotomy; Parenchyma
Introduction
Physical exam was non-contributory. Given the concern for venous thromboembolism she had D-Dimer levels evaluated, which were in the normal range. However, clinical suspicion remained high for pulmonary embolism prompting a cross sectional imaging. Her initial results showed arterio-venous malformation near the left lower lobe. Dedicated high quality lung imaging showed direct connection from the aorta to a small area of lung tissue raising suspicion of pulmonary sequestration (Figure 1).
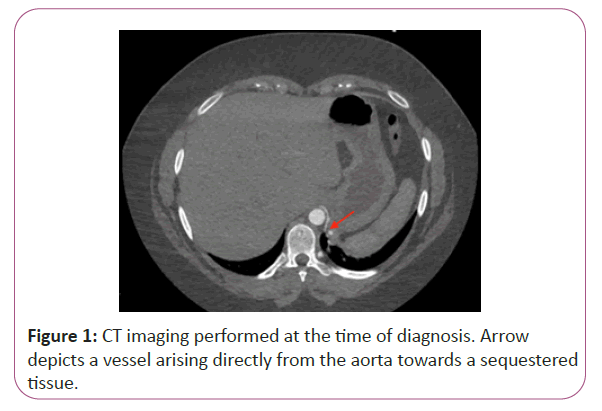
Figure 1: CT imaging performed at the time of diagnosis. Arrow depicts a vessel arising directly from the aorta towards a sequestered tissue.
Since pulmonary sequestration is a relatively uncommon congenital disease and is rarely diagnosed in adults, tissue diagnosis is essential to rule out malignancy. Patient was taken to the operating room for robotic assisted resection of the mass [1]. Usually these operations are done using posterolateral thoracotomy as the sequestered lung tissues have small feeding vessels directly arising from the aorta, which if not controlled correctly can result in significant blood loss (Figure 2).
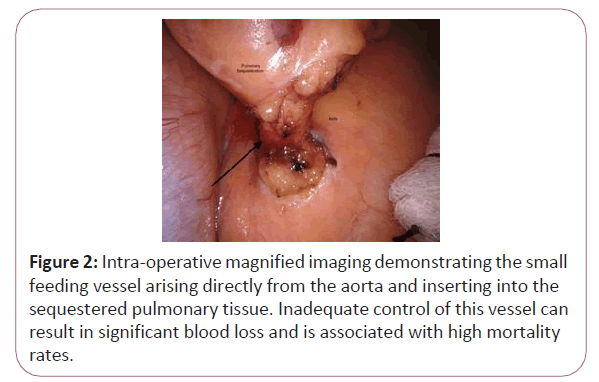
Figure 2: Intra-operative magnified imaging demonstrating the small feeding vessel arising directly from the aorta and inserting into the sequestered pulmonary tissue. Inadequate control of this vessel can result in significant blood loss and is associated with high mortality rates.
However, additional range of motion provided by robotic instruments allowed clear isolation and dissection of the lesion as shown in the Figure 3.
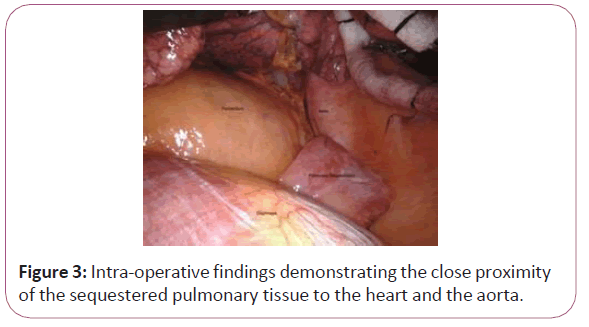
Figure 3: Intra-operative findings demonstrating the close proximity of the sequestered pulmonary tissue to the heart and the aorta.
As seen in the image, the sequestered lung tissue is independent of the lung parenchyma proper and has its own feeding vessels. Patient tolerated the procedure well and was discharged home on post op day 1 and reported no complications on subsequent clinic visit.
Patients with pulmonary sequestration usually present with recurrent respiratory complications that are often attributed to other underlying pathology [2]. These patients are rarely diagnosed in adulthood. Even though the sequestered tissue is small in size, it can harbor malignancy and as in this case affect the quality of life of the patient. Surgical management can be challenging as these cases often require large posterolateral thoracotomy to access the lesion and adequately ligate the feeding vessels. Failure to do so can result in significant blood loss directly emanating from the aorta. Robotic surgery in this setting can reduce complication profile of surgical approach without compromising safety.
36135
References
- Alsumrain M, Ryu JH (2018) Pulmonary sequestration in adults: a retrospective review of resected and unresected cases. BMC Pulm Med. 18(1):97.
- Halkic N, Cuénoud PF, Corthésy ME, Ksontini R, Boumghar M (1998) Pulmonary sequestration: A review of 26 cases. Eur J Cardiothorac Surg. 14(2):127–33.

