Keywords
Gyrus; Prosodical; Multiple sclerosis; Hyperventilation; Globus pallidum
Introduction
Foreign Accent Syndrome (FAS) is rare speech disorder that affects about 80 persons in all the world. It was first described in 1907 by Pierre Marie, it´s a rare speech disorder characterized by segmental (abnormality in time of pronunciation of vocal and consonant) and prosodical deficits (abnormality in rhythm and intonation of words and phrases) without abnormal grammatical abnormalities, the patient´s speech resembles a non-native accent. The most of cases present like an acquired abnormality of the speech due to a damage of the central nervous system [1].
Symptoms can persist months or years or maybe it could be disappeared spontaneous or progressively [1].
Causes
Neurogenic: Due to lesions in central nervous system, specifically in motor areas of dominant hemisphere in relation with speech: precentral and frontal medium gyrus, lower portion of parietal gyrus, the insula (previous part) and subcortical adjacent structures. (Etiology: stroke, brain trauma, multiple sclerosis, tumor). This form less frequently can be linked to development of the speech.
Psychogenic cause: It is not due to damage of the brain, it is relation with psychiatric or psychological disturbance like: depression, schizophrenia, autism, anxiety, bipolar disorder, personality disorder, or conversion reaction or converse disturbance [2,3].
Mix cause
Involvement areas
Dominant hemisphere for speech, regions like subcortical left fronto-temporal parietal and subcortical areas: precentral gyrus, premotor area, supplementary motor area, postcentral gyrus, left parietal area, cerebellum, and basal ganglia (caudate, putamen and globus pallidum) [1,2].
This accent is caused by an abnormality of capacity of program the sequence of movement and the position of muscles in relation with speak. It causes abnormalities in the accentuation, intonation and sound of consonants, changes in the articulation of vocals and finally abnormalities of syllabic structure [3]
Structural abnormalities of basal ganglia (caudate and putamen nuclei) have been n in some children with language disturbances [4,5].
We present a case with FAS secondary to multiple sclerosis event. In Cuba we know scarce cases with FA secondary to cerebro-vascular event; they are having not been published. This is the first case secondary to Multiple Sclerosis that we know in Cuba.
Materials and Methods
We described a case with FAS in relation with Multiple Sclerosis. Clinic Neurophysiological and Image evaluation were done to her. It included:
Visual evoked potential (PEV)
Oz-Fz montage was used, pattern stimulator was applied to each eye, using conventional parameters. We analyzed bilateral P100 wave latency.
Auditory brainstem evoked potential (ABEP)
A1-Cz montage was used, click stimulator was applied to each ear, using stimulation intensity of 90 dB, and conventional parameters of stimulation and record. We analyzed bilateral I, III and IV wave’s latencies, I-V, I-III and III-V intervals.
Somatosensory evoked potential (SSEP)
Cz-Fz and L1-Iliac spine montage was used, tibial nerve behind medial malleolus was stimulated with electric pulses, using conventional parameters of register and stimulation. We analyzed bilateral P40 and L1 wave’s latencies and Central Conduction Time.
Electroencephalogram (EEG)
19 channels of 10/20 international montage were used. Close eyes, open eyes, hyperventilation, recuperation and fotoestimulation stages were registered. Visual analysis of EEG signal was done for an expert. Quantitative measures of automatized analysis of EEG signal were evaluated: Narrow band measures, broad band measures (absolute power, relative power and mean frequency of alpha, beta, theta and delta bands).
Image acquisition
MRI was carried out using a 3 T Allegra system scanner (Siemmens) equipped with a standard quadrature head coil. High-resolution three-dimensional whole-brain. T1 and T2- weighted, FLAIR and diffusion weight MRI scans were acquired.
Case Description
Cuban female of 65-year-old, right hands, with diagnosis of multiple sclerosis. She has not experience in any foreign language. Native foreign: Spanish. She suddenly starts speaking in Spanish but with English accent.
Tests
Visual evoked potential (PEV): P100 wave latency was prolonged bilaterally, left P100 wave morphology was abnormal (Figure 1). It traduces abnormality of nerve conduction on visual system due to demyelinating.
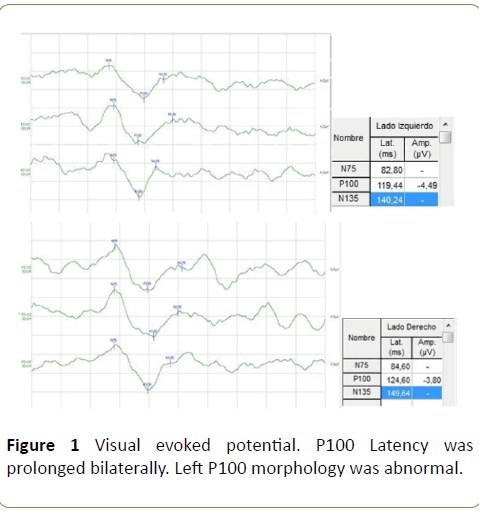
Figure 1: Visual evoked potential. P100 Latency was prolonged bilaterally. Left P100 morphology was abnormal.
Auditory brainstem evoked potential (ABEP): Was normal (Figure 2).
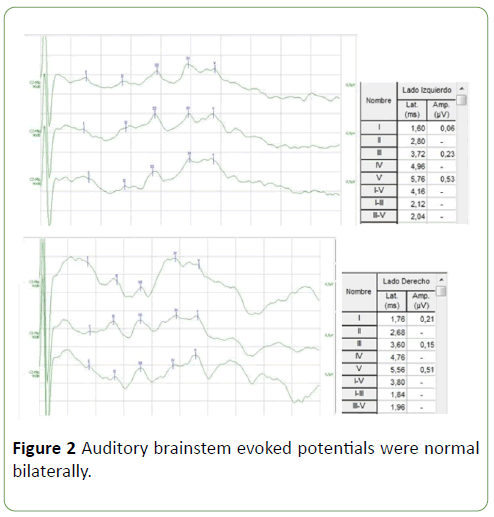
Figure 2: Auditory brainstem evoked potentials were normal bilaterally.
Somatosensory evoked potential (SSEP): P40 wave latency was prolonged on the left side (Figure 3). It traduces abnormality of nerve conduction on somatosensory way at parietal area, probably due to demyelinating.
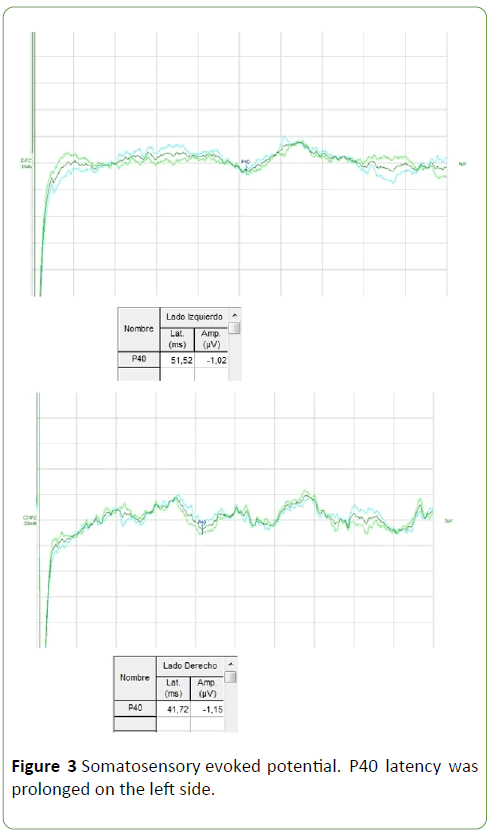
Figure 3: Somatosensory evoked potential. P40 latency was prolonged on the left side.
Visual electroencephalogram (EEG): It showed paroxysmal activity on bilateral Fronto-Centro-Temporal regions (Figure 4). It shows abnormalities of the function of those areas.
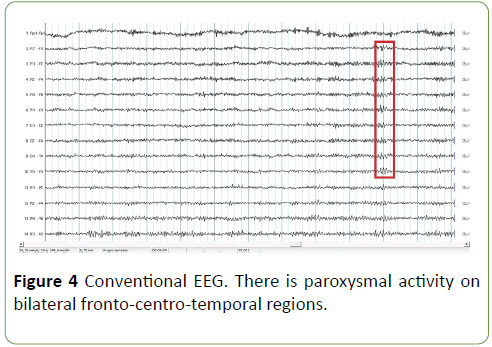
Figure 4: Conventional EEG. There is paroxysmal activity on bilateral fronto-centro-temporal regions.
Quantitative EEG (QEEG):
Narrow band measures: It showed a peak of energy on theta band in all of derivation, predominantly in lower frontal and temporal regions (Figure 5). It shows abnormalities of the function of those areas.
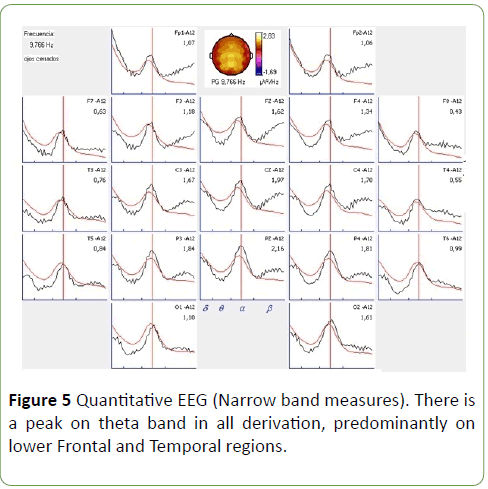
Figure 5: Quantitative EEG (Narrow band measures). There is a peak on theta band in all derivation, predominantly on lower Frontal and Temporal regions.
Broad band measures: It showed an increase of absolute power, relative power and mean frequency of theta band on lower Frontal and Temporal regions (Figure 6). It shows abnormalities of the function of those areas.
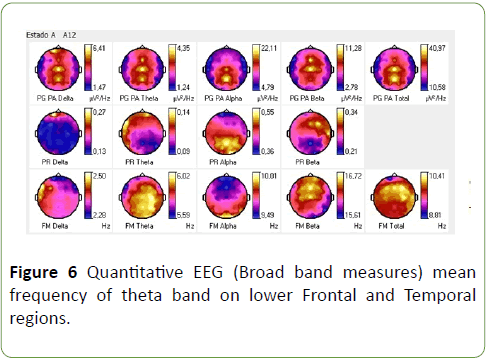
Figure 6: Quantitative EEG (Broad band measures) mean frequency of theta band on lower Frontal and Temporal regions.
3T MRI: Hyperintense yuxtaxial image in cortical regions, hypointense images in brain stem. Demyelinating plaques on left Frontal, Parietal and Temporal subcortical areas and in periventricular regions (Figure 7). It shows anatomic abnormalities of those areas.
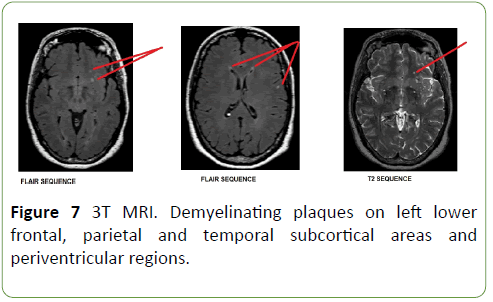
Figure 7: 3T MRI. Demyelinating plaques on left lower frontal, parietal and temporal subcortical areas and periventricular regions.
Outcome: Patient was hospitalized; she was tried with intravenous pulses of methylprednisolone for five days. Past 3 months, she recovered her normal Spanish accent but in MRI are keep demyelinating images on lower left frontal, parietal and temporal areas (Figure 8).
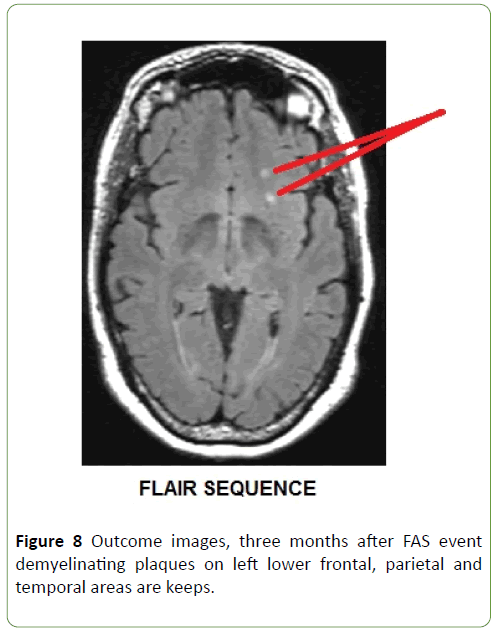
Figure 8: Outcome images, three months after FAS event demyelinating plaques on left lower frontal, parietal and temporal areas are keeps.
Results and Discussion
Electrophysiological and Image studies of our patients showed structural and functional abnormalities of lower frontal, temporal and parietal regions bilaterally with predominance of left side, due to an event of multiple sclerosis.
Apparently in FAS there is a disturbance of front basal circuit of motor control, they are complex circuits with loop form, and they are origin in frontal cortex, they are in relation with subcortical structures, fundamentally basal ganglia and they return to the cortex by thalamic way (cortico-striato-pallidalthalamic loop). This kind of circuits are control circuits, they modulate and regulate order of motor cortex [4,6]. FAS has been reported in relation with varied conditions such as: after surgery of brain tumor or arteriovenous [7].
Central process of speech is a very complex process; it needs the integrity of posterior part of dominant hemisphere of temporal, parietal and occipital lobes. Most important functions that takes place in those structures are: Transformation of receive language in its significant content, conversion of inner significant content in a language for exteriorization, access to vocabulary and grammatical order of the words [7-9].
Central processor of language converts the significant sequences of words in a nervous code that would order to motor programmer of speech, which will activate selectively the necessary muscles to speech in adequate order, duration and sequence [7].
Emotional component of speech is another important and complex process; it could be disturbance in FAS. Mitchell et al. in 2016 did an experiment in health subjects and concluded that the superior temporal gyrus and basal ganglia may be involved in expressing emotional prosody irrespective of the specific emotion. Inferior frontal gyrus activity may be more variable, and might relate to the participants sampled since its activity correlated with participants’ ability to express the target prosodic emotions [3].
In another hand, Whitaker had postulated some diagnosis criteria for FAS. The accent is considered by the patient, by acquaintances and by the investigator, to sound foreign. It is unlike the patient’s native dialect before cerebral insult. It is clearly related to central nervous system damage.
Here is no evidence in the patient’s background of being a speaker of a foreign language [10,11]. Those criteria would be fulfilled in a case of FAS patients, it is considered a rare condition due to it affected a low of persons in all the world [10,11].
FAS of neurological origin are most common of psychogenic causes. Gurd et al. in 2012 reported a case of FAS, which was qualified as psychogenic, even though CSF analyses revealed oligoclonal bands, a bio-marker of Multiple Sclerosis (MS) and EEG revealed transient spikes. Over the left temporal lobe. T2 hyper-intensities were found on MRI, it was demonstrated that this patient really develops FAS as a consequence of their neurological disorder or due to accompanying psychological distress [12].
Some authors have described that that 20% to 25% of MS patients have disturbance of verbal fluid in speech, other abnormalities have been described like rare disorders [13,14] Villa Verde, et al. in 2003 reported a case with MS that debuted like a FAS, MRI demonstrated several demyelinating plaques all neurophysiological tests were normal [15].
The collective evidences across a variety of clinical population shows the role of a set of areas in accent processing; these include Broca’s area (frontal operculum and posterior third of the inferior frontal gyrus), the premotor cortex, the striatum, the insula, the pallidum, the thalamus, as well as white-matter pathways of the internal capsule all typically on the left side in right handed patients [16].
Some authors are agreed in the involved of brain structures in speech, others have purposed new functions. Some experiments in healthy second language learners in relation with fMRI have showed a significant activation in left middle occipital gyrus, left Lingual gyrus, left inferior frontal gyrus, left precentral gyrus, left inferior frontal gyrus and left, and right middle occipital gyri, right parahippocampal gyrus, right cerebellar tonsil and the insula. Mostly of those areas have been showed impaired in FAS patients [16].
Moreno Torres in 2013 reported a case of a woman with chronic FAS, her MRI showed bilateral lesions, particularly in the left deep frontal operculum, and dorsal anterior insula. Also, Diffusion Tensor Imaging (DTI) and tractography suggested disrupted left deep frontal operculum-anterior insula connectivity. Positron Emission Tomography (PET) showed decreased activation in Brodmann’s areas 4, 6, 9, 10, 13, 25, 47, in the basal ganglia, and anterior cerebellar vermis. The authors have argued that the ensemble of the neurofunctional and neuroanatomical evidence from this single-case report suggests that FAS entails altered planning and execution of speech production, with both cognitive control and emotional communication dimensions, this report shows the key role played by the insula-frontal operculum circuit in the processing of accent [17].
Katz et al. in 2012 reported the activation maps related to a picture-naming task in an English-speaking woman with FAS of unknown etiology. The activations included the left superior temporal and medial frontal structures, bilateral subcortical structures and thalamus, the left insula and the left cerebellum. Similar results were showed by their PET study. Authors conclude that FAS is a result of an impairment of the feed-forward control commands, in particular of the articulator velocity and position maps [18,19].
Another PET study by Poulin et al. examined FAS in a case of bipolar syndrome and reported hypometabolism in the frontal, parietal and temporal lobes bilaterally, as well as a focal damage in the left insular and anterior temporal cortex [20], thus pointing to the role of the anterior temporal gyrus and the left insula in accent processing [20,21]
Keulen in 2016 reported a FAS case. It was a 17 years old man without any apparent causes. SPECT was done to him, it demonstrated a significant bilateral hypoperfusion distributed in the medial prefrontal regions and in both lateral temporal regions. Decreased perfusion in the left inferior medial frontal region, right inferior lateral frontal region and right cerebellar hemisphere nearly reached significance, this SPECT findings lead to the hypothesis this pattern of hypoperfusions reflects significant involvement of the cerebro- cerebellar functional connectivity network [22].
Carbary in 2000 reported a 51 years old male with FAS following head and throat trauma from a physical assault that injured left frontal cortex. Undoubtedly frontal lobe is in relationship with prosodic component of speech [23].
Berthier et al. in 2015 reported FAS in three Argentinean monolingual speakers with different causes (brain hemorrhage, aneurysm and abscess). In those patients structural lesion of the brain overlapped in left pericentral regions (inferior frontal gyrus, Rolandic operculum, middle frontal gyrus, precentral gyrus, post-central gyrus and dorsal insula). The greatest area of overlap was the left precentral gyrus [24].
Berthier et al. in 2016 reported two FAS patients, theirs MRI revealed a venous angioma close to the head of the left caudate that crossed the medial frontal lobe white matter to drain into the superior sagittal sinus, a mild dilatation of the left lateral ventricle in one of subject, in the other MRI showed expanded perivascular spaces mainly involving both insular cortices. Parenchymal changes adjacent to the venous angioma have been described and correspond to demyelination, gliosis, leukomalacia and neuronal degeneration or result from compensatory adaptive changes secondary to hemodynamic disturbances. These findings suggest that the anatomical distribution of the venous angioma in subject 1 may have altered intrinsic connectivity within the frontal lobe [25].
Conclusion
In conclusion in the actually it is not clear all brain structures that are involved in speech and it´s emotional component. Due to redundancy of the results it is possible to affirm that brain structures such as: insula, precentral and postcentral gyrus, frontal and temporal lobes play and important role in some components of speech.
Undoubtedly FAS continue to be a rare disorder, the most frequent cause is vascular disease, nevertheless we present a FAS patient secondary to Multiple Sclerosis, in whom neurophysiological and image studies have confirmed disturbance of the function of frontal, temporal and parietal areas and some of their connections.
21691
References
- Buentello GRM, Martínez RAR, Cisneros FJM, AlonsoVMA (2011) Síndrome de acento extranjero. Arch Neurocir 16: 167-169.
- Vares GE (2015) Un nuevo caso de síndrome del acento extranjero ligado al desarrollo. Revista de Logopedia, Foniatría y Audiología 35: 77-83.
- Mitchell RLC, Jazdzyk A, Stets M, Kotz SA (2016) Recruitment of language, emotion and speech-timing associated brain regions for expressing emotional prosody: Investigation of functional neuroanatomy with fMRI. Front Hum Neurosci 10: 518.
- González AJ, Parcet IMA, Ávila C, Geffner SD (2003) Una rara alteración del habla de origen neurológico: el síndrome del acento extranjero. rev neurol 36: 227-234.
- Checa MA, Quevedo BR (2017) Revisión sistemática en el Síndrome del Acento Extranjero: intervención y terapia del lenguaje. Revista Iberoamericana de Psicología y Salud 8: 1-8.
- Pinillos CP (2014) This is not my voice: A review of the foreign accent syndrome. Estudios interlingüísticos 2: 107-116.
- Sosa F, Bustamante J, Rodríguez F, Argañaraz R, Rubino P, et al. (2016) de aneurisma luego de exéresis de MAV con aparición de síndrome del acento extranjero. Rev Argent Neuroc 30: 81-85.
- Blasco TE. Apraxia del habla. Presentación de un caso clinic. Lingüística clínica y neuropsicología cognitiva. Actas del Primer Congreso Nacional de Lingüística Clínica. Investigación e intervención en patologías del lenguaje. Valencia: Universitat.
- Keulen S, Verhoeven J, DeWitte E, De Page L, Bastiaanse R, et al. (2016) Foreign accent syndrome as a psychogenic disorder: A review front Hum. Neurosci 10: 168.
- Whitaker HA (1980) Levels of impairment in disorders of speech. In: Proceedings of the NATO Advances Study Institute of Neuropsychology and Neurocognition, Augusta, Georgia. pp. 168-207.
- Gurd JM, Coleman JS, Costello, Marshall J (2012) Organic or functional? A new case of foreign accent syndrome. Cortex 37: 715-718.
- Keulen S, Verhoeven J, Bastiaanse R, Mariën P, Jonkers R, et al. (2016) Perceptual accent rating and attribution in psychogenic FAS: Some further evidence challenging whitaker’s operational definition. Front Hum Neurosci 10: 62.
- Alegre AJ (2017) Esclerosis Múltiple: Alteraciones cognitivas y actividades de la vida diaria.
- Villaverde GR, Fernández VE, Moreno EA, Alías LE, García SJM (2003) Foreign accent syndrome as the first manifestation of multiple sclerosise. Rev Neurol 36: 1035-1039.
- Ghazi SL, Dash (2015) How native-like can you possibly get: fMRI evidence for processing accent. Front Hum Neurosci 9: 587.
- Moreno TI, Berthier ML, MarCid MD, Green C, Gutiérrez A, et al. (2013) Foreign accent syndrome: A multimodal evaluation in the search of neuroscience-driven treatments. Neuropsychologia 51: 520-537.
- Katz WF, Garst DM, Briggs RW, Cheshkov S, Ringe W, et al. (2012) Neural bases of the foreign accent syndrome: A functional magnetic resonance imaging case study. Neurocase 18: 199-211.
- Tomasino B, Marin D, Maieron M, Ius T, Budai R, et al. (2013) Foreign accent syndrome: A multimodal mapping study. Cortex 49: 18-39.
- Poulin S, Macoir J, Paquet N, Fossard M, Gagnon L (2007) Psychogenic or neurogenic origin of agrammatism and foreign accent syndrome in a bipolar patient: a case report. Ann Gen Psychiatry 6: 1.
- Moreno TI, Mariën P, Dávila G, Berthier ML (2016) Editorial: Language beyond words: The Neuroscience of Accent. Front Hum Neurosci 10: 639.
- Keulen S, Mariën P, Wackenier P, Jonkers R, Bastiaanse R, et al. (2016) Developmental foreign accent syndrome: Report of a new case. Front Hum Neurosci 10: 65.
- Carbary TJ, Patterson JP, Snyder PJ (2000) Foreign accent syndrome following a catastrophic second injury: MRI correlates, linguistic and voice pattern analyses. Brain Cogn 43: 78-85.
- Berthier ML, Dávila G, Moreno TI, Beltrán CÁ, Santana MD, et al. (2015) Loss of regional accent after damage to the speech production network. Front Hum Neurosci 9: 610.
- Berthier ML, Roé-Vellvé N, Moreno TI, Falcon C, Thurnhofer HK, et al. (2016) Mild developmental foreign accent syndrome and psychiatric comorbidity: Altered white matter integrity in speech and emotion regulation networks. Front Hum Neurosci 10: 399.

