Keywords
Refugees; War; Psywar; Phywar; Treatment by repeating phrases of positive thoughts; Unstable countries; Iraq; Syria
Highlights
1. The first study to examine the potential effects of Treatment by Repeating Phrases of Positive Thoughts (TRPPT) to reduce mental-war disorders in Syrian refugees populations war victims.
2. After 7 days TRPPT, positive treatment effects were found on post-traumatic disorder and psywar and phywar difficulties such as depression, anxiety, stress symptoms, low selfesteem, and dissatisfaction in life.
3. Study uses an important group of subjects, with a valid therapeutic cognitive therapy tool and positive psychotherapy on mental-war disorders in War.
Introduction
According to Acarturk, et al. [1], the most common mental health problems among refugees are depression and post traumatic stress disorder.
Syria is currently in the midst of a crisis level complex emergency, which started in 2011. United Nations (UN) and Government of Syria joint assessment mission, highlighted mental health and psychosocial support (MHPSS) as one of the most urgent concerns resulting from the crisis [2]. According to McKenzie et al. [3] the burden of neuropsychiatric disorders in refugees is likely high, but little has been reported on the neuropsychiatric disorders that affect Syrian and Iraqi refugees. Neuropsychiatric disorders are an important burden to health among Iraqi and Syrian refugees [3]. Depression or mental illness is now starting to be recognized by the UN and aid agencies as a real problem facing many Syrian refugees [4].
Among mental and psychological troubles, depression, anxiety, and stress are significantly more common in people with neurologic disorders than in the general population, and its presence is associated with increased symptom burden, morbidity, and treatment costs [5]. High levels of depression have been found among multiple sclerosis (MS). Depression among patients with multiple sclerosis (MS) is common and has a significant impact on quality of life. As many as two-thirds of depressed MS patients receive no treatment for their depression [6].
Depression in this patient population is often unrecognized owing to a high level of symptom overlap between mood and neurologic disorders [4]. The development of diagnostic criteria and treatment that are specific for depression in the context of neurologic disease is warranted. In the patient with MS, psychotherapy also should be considered. The presence of negative automatic thoughts is one aspect of negativity in cognition in people with depression [7]. Kendall suggested that examination of both negative and positive cognitions could contribute to a better understanding of the health-pathology relationship [8].
Depression is prevalent among individuals, but research suggests that it remains under-detected [9-12] and under-treated [6,13].
Untreated depression may contribute to a decrease of quality of life and an increase of morbidity and mortality associated with MS, and among student. This Untreated depression will increase during the war among clinical and non-clinical population [14-24].
In the past ten years, several randomized controlled trials [25-27] and a 2006 Cochrane review [28] have found that cognitive behavioral interventions are efficacious in treating depressive disorders and symptoms in individuals with MS [29]. In addition, cognitive behavioral interventions delivered by telephone were found to be effective in treating depression relative to usual care [25] and to telephone-delivered supportive-expressive therapy [27]. Telephone-delivered interventions are potentially quite valuable in MS because they mitigate barriers such as transportation and fatigue which may interfere with accessing psychotherapy [29].
This study was to emphasis on the role positive thoughts for the treatment the mental and psychological troubles in patients with MS and also students who are victims of the current war in Syria.
The article 5 of the Universal Declaration of Rights Man states that "no one shall be subjected to torture, or to cruel, inhuman or degrading" [30]. Between 20 and 35% of the refugee population in the world have been victims of torture or extreme violence [31-35]. In this context, France, with more than 55,000 new asylum applications a year, is the fourth consecutive year placed second in the world of industrialized countries to receive more requests for obtaining refugee status [36-38].
Asylum, displacement, migration, leave the original housing, leave the family home of origin, leave the village and the original town and leave the country to other countries in inhumane conditions such as war are most forms extremes of human violence, its consequences and treatments have been few studies in scientific research compared to other forms of traumatogenic events.
In this context, Syria, with over 1000 000 new asylum applications per year; with more than 13 million refugees and among them millions suffer psychological and physical difficulties, is the fifth consecutive year placed first among the countries suffering the effects of war, the international silence, religious lethargy and inhuman anesthesia.
The psywar and phywar difficulties leave scars in psychophysiological level among people face war.
Psywar is the psychological consequence of torture and war violence as post-traumatic stress disorder (PTSD), fear, anxiety and major depressive episode (MDE) [24].
Phyguerre is the physical consequence of torture and war violence as distortions, deformation, loss of an arm or feet, etc. [24].
Steel et al. [39] in their meta-analysis of 181 studies, representing more than 81 800 refugees have indeed shown that the prevalence of PTSD and SHS in victims of torture was respectively 46.2% and 49.6% [39]. Fazel et al. [40] have also determined that the refugees were ten times more likely to present a traumatic disease than the general population of the host country in which they are received [40].
However, all research agrees today that the treatment of psychological disorders such as PTSD by cognitive behavioral therapy focused on trauma (CBT) and therapy Movement Desensitization and Reprocessing Eyes (EMDR) but access to these treatments in the war is not easy all the time [41-45].
So, the objective of this study was to explore the short-term effects of the treatment program (TRPPT: Treatment by Repeating Phrases of Positive Thoughts) in the war which is easy all the time.
Methods
Hypotheses
The main hypothesis was to obtain a significant improvement in symptoms of depression after treatment, and possibly other dimensions of psychological functioning as symptomatology’s anxious, stressed, low self-esteem, and dissatisfaction in life.
Sample
The total sample consisted of 20 students (20 women) from the University of Damascus, aged 19 to 27 years and 7 MS patients (3 men and 4 women) from Damascus Hospital and Ibn Alnafees Hospital, aged 20 to 35 years. Participation is voluntary. Our study is a randomized controlled trial. After randomization, participations are divided into two groups. It was composed of two groups: experimental group (17 participants=7 MS patients (M: 26.6 years; SD ± 6.18) and 10 students, aged 19 to 24 years (M: 21.30 years, SD ± 1.33) and control group (10 participants=10 students, aged 19 to 27 years (M: 22.20 years; SD ± 2.65). The method of RPPT involved repeating positive thoughts related or not related to psywar and phywar difficulties. Participants received training in the designated method and then practiced it for one week, before attending for reassessment. The treatment took place over 7 days, based on RPPT exercises (Annex 1). Participants will repeat and generate the Phrases of Positive Thoughts. Before the first SMS by phone, the students and MS patients have received education in the RPPT in 15 minutes (Annex 1), led by a psychologist, with an explanation on the progress of research and measurement tools.
Intervention and participants
This RPPT procedure was performed with Syrian refugees populations war victims in order to reduce the severity of psychological and emotional disorders (depression, anxiety stress and their symptoms) and to see the effects of this approach on health in general under monstrosity conditions. Experimental group was compared to a control group (Figure 1).
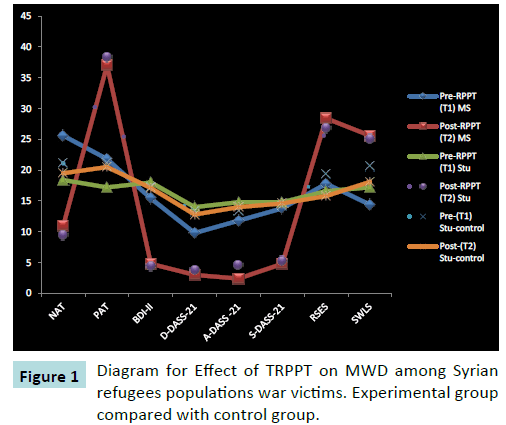
Figure 1: Diagram for Effect of TRPPT on MWD among Syrian refugees populations war victims. Experimental group compared with control group.
Practical proceedings of study
According to this scheme, the data collection process and TRPPT take place in several stages.
Description of the TRPPT method
Treatment by Repeating Phrases of Positive Thoughts (TRPPT) has been originated as a treatment for emotional disorders (depression, anxiety and stress) among French students by Alsaleh in 2016.
This study presents a description of the TRPPT method, with some initial pilot testing of its effectiveness in the research of Alsaleh in 2016 on this method. The objective of her study was the first to evaluate the short-term effects of the method of RPPT (Repeating Phrases of Positive Thoughts) on sample that consisted of 44 students (11 men and 33 women) from the University of Caen, aged 18 to 23 years.
However, futures researches are may be increasingly reused and reexamined the TRPPT with chronic and mental illnesses for improve psychosocial health outcomes.
For it, Alsaleh is in the process of reproduce the work and its results on a clinical sample at the Hospital of Caen.
In this study, a maximum of four sessions (25-35 min per session) of TRPPT were conducted. Each treatment consisted of three or four phases. Phase 1 consists of agreement taking, initial evaluation after the agreement and treatment planning. In Phase 2 the individuals were prepared for TRPPT by explaining this therapy. Participants also learned techniques of reformation the phrases and positive self-talk techniques in this stage (Annex 2). The motivation of participants for RPPT showing the effectiveness of PT and RPPT in everyday life, in a stressful situation, the mental and psychological illness, psychosomatic illness, physical illness and in brain activity. Before the first SMS by phone, participants have received education in the RPPT in 15-25 minutes (Annex 2), led by a psychologist, with an explanation on the progress of research and measurement tools. Participants (patients and/ or students) in the experimental group repeated the phrases of positive thoughts every day at least three times for 3 to 5 min from the morning awakening and evening before sleeping [24]. The benefits obtained are related with the intensity of the daily practice of RPPT.
In Phase 3, participants have received SMS by phone (Annex 1) for 7 days, led by a psychologist. The method of RPPT involved repeating positive thoughts related or not related to mental-war disorders and difficulties. Participants received training in the designated method and then practiced it for one week, before attending for reassessment. The treatment took place over 7 days, based on RPPT exercises (Annex 1). Participants will repeat and generate the Phrases of Positive Thoughts [13].
Phase 4 is reassessment and the remotivation phase for continue to use RPPT and positive self-talk techniques [13].
Ethical review
Participation was voluntary and responses were anonymous. This study received approval from the neurology service, Damascus Hospital and Ibn Alnafees Hospital. The Ethics and Research Committee of the Damascus Hospitals Complex approved the study protocol, informed consents were obtained from the participants after the aims and objectives of the study have been explained. Human ethics committee approval protocol number was 07/2015/10 -?/ 5174 .
All participants gave the informed consent prior being included into the study.
Assessment of Clinical Symptoms and Automatic Thoughts
All participants completed an assessment and clinical evaluation that utilized the following structured interview and questionnaires.
Automatic thoughts questionnaire-Arabic (ATQ- 18-Ar)
The ATQ [46,47] measures the frequency of cognitive selfstatements associated with depressed mood. The Syrian version of the ATQ-18-Ar includes 8 items on negative automatic thoughts (NAT) and 10 items on positive automatic thoughts (PAT). ATQ- 18-Ar validated by the authors [48] All items are scored on a 5-point Likert scale, with 1=not at all and 5=all the time. The validity and reliability of the Syrian version of the ATQ-18-Ar was demonstrated by the authors. The internal consistency reliability of the 18-item ATQ-18-Ar was very satisfactory. Cronbach’s alpha was 0.87 for the NT (Negative thought) total score and 0.85 for the PT (Positive thought) total score. The split-half reliability was 0.86 for the NT total score, 0.90 for the PT total score, and 0.81 for the ATQ-18-Ar total score. The results suggested that the ATQ-18-Ar possessed high internal consistency.
Beck depression inventory-II (BDI-II)
The BDI-II [49] is a 21-item self-report instrument that assesses the severity of depressive symptoms in adolescents and adults over the last two weeks.
Depression anxiety stress scale-21
The patients were assessed by the Depression Anxiety Stress Scale-21 (DASS-21), a 21-item self-report scale measuring characteristic attitudes and symptoms of depression, anxiety and stress [50,51].
Rosenberg self-esteem scale (RSES)
The RSES [52] consists of 10 Likert-type scale items designed to assess positive evaluations of the self.
Satisfaction with life scale (SWLS)
The SWLS is a 5-item scale designed to measure global life satisfaction [53].
Statistical Analysis
Statistical analysis was performed on 27 participants [17 (10 students and 7 MS patients) for the experimental group following the treatment of the RPPT and 10 students women for the control group not following the treatment of the RPPT]. The objective of the statistical analysis is to describe and assess changes in Mental-war disorders (MWD) associated with repeating phrases positive thoughts (RPPT). To evaluate the effectiveness of this procedure, a comparison of scores before and after (T1 vs T2) was performed for both depression scales (BDI-II and DASS-21), using a test of mean comparison Wilcoxon, considering the scale of DASS-21 as the main variable.
The effect size, using the coefficient "r" of Cohen and standardized response mean between T1 and T2 were calculated.
The threshold of significance tests is 0.05. All statistical analysis was performed using R.
Results
Results analysis
To study the TRPPT with Syrian refugees populations war victims, 20 students were analyzed (10 for the experimental group following the treatment of the RPPT and 10 for the control group not following the treatment of the RPP), and 7 MS patients for the experimental group following the treatment of the RPPT.
TRPPT and mental-war disorders (MWD)
The treatment of the RPPT has had an effect on the experimental group compared to a control group. The hypothesis tested (H0) is rejected because the threshold used Wilcoxon test of significance (0.05) shows that there is a difference between the experimental group who repeated the RPPT and the control group did not follow the RPPT. The RPPT, thus, significantly reduce depression, anxiety and stress and confirms our hypothesis tested (H1) (Figure 2).
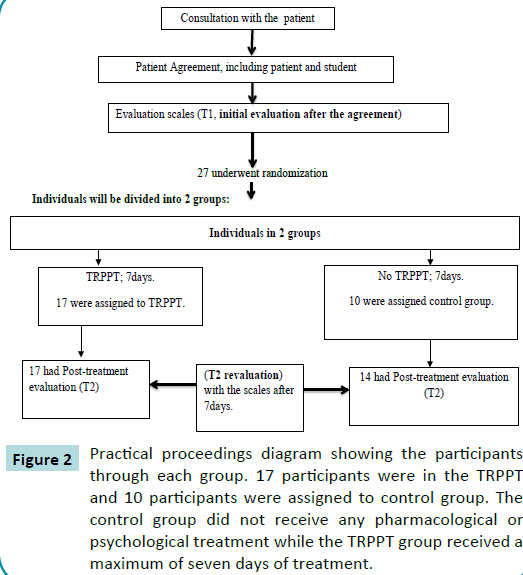
Figure 2: Practical proceedings diagram showing the participants through each group. 17 participants were in the TRPPT and 10 participants were assigned to control group. The control group did not receive any pharmacological or psychological treatment while the TRPPT group received a maximum of seven days of treatment.
TRPPT, anxiety and stress-DASSS-21
The measures in the pre- and post-treatment (treatment) showed significant differences in the two groups (experimental and control) (Table 1 and Figure 1). In the experimental group (students and MS patients), there is a significant reduction in stress following the RPPT protocol (p<0.001, p<0.05). Participants have a diminished stress between beginning and end of the experiment. At the level of anxiety, measures pre- and posttreatment showed a significant difference in the experimental group. Participants have less anxiety due to RPPT protocol (p<0.001, p<0.05).
| |
experimental group, RPPT (N=17) |
control group (N=10) |
| |
7 MS |
10 students |
10 students |
| |
Pre-RPPT (T1) MS |
Post-RPPT (T2) MS |
ES T1-T2 |
SRM |
Pre-RPPT (T1) Stu |
Post-RPPT (T2) Stu |
ES T1-T2 |
SRM |
Pre (T1) |
Post (T2) |
| NAT |
25.6 (9.15) |
11 (4.52)* |
1.595 |
1.590 |
18.40 (4.94) |
9.40 (1.64)*** |
1.822 |
1.982 |
21.10 (3.31) |
19.50 (3.10)£ |
| PAT |
21.8 (9.28) |
37 (3.60)*** |
1.643 |
2.314 |
17.20 (9.76) |
38.30 (4.83)*** |
2.162 |
1.903 |
21.20 (4.31) |
20.50 (3.43)£ |
| Depression-BDI-II |
15.4 (7.33) |
4.8 (2.16)* |
1.446 |
1.715 |
18.00 (5.20) |
4.40 (1.26)*** |
2.615 |
2.845 |
17.30 (4.00) |
17.10 (4.30)£ |
| Depression- DASS-21 |
9.8 (6.61) |
3.0 (1.41)* |
1.028 |
1.281 |
14.00 (4.39) |
3.80 (1.03)*** |
1.962 |
2.138 |
13.30 (3.36) |
12.80 (2.65)£ |
| Anxiety- DASS -21 |
11.8 (6.30) |
2.4 (1.51)** |
1.492 |
1.818 |
14.80 (4.46) |
4.6 (1.07)*** |
2.286 |
2.487 |
13.40 (2.83) |
14.00 (3.39)£ |
| Stress- DASS -21 |
13.8 (6.45) |
4.8 (2.86)* |
1.395 |
1.657 |
14.80 (4.02) |
5.30 (2.35)*** |
2.363 |
2.393 |
14.20 (2.97) |
14.60 (2.17)£ |
| RSES |
17.8 (4.81) |
28.4 (1.14)** |
2.204 |
2.711 |
16.6 (5.07) |
26.8 (2.04)*** |
1.676 |
2.546 |
19.40 (4.29) |
15.8 (4.31)£ |
| SWLS |
14.4 (7.82) |
25.6 (0.89)* |
1.432 |
1.362 |
17.2 (5.39) |
25.10 (1.19)*** |
1.781 |
1.775 |
20.60 (2.95) |
18.10 (3.14)£ |
Means and standard deviations (in parenthesis) obtained at baseline (T1) and after treatment (T2), with comparisons of means between T1 and T2 and calculation of effect sizes between T1 and T2.
MS=Multiple Sclerosis. Stu= Students. NAT=Negative Automatic Thought.PAT=Positive Automatic Thought. DASS-21: Depression Anxiety Stress Scales-21. D: Depression. A: Anxiety. S: Stress. BDI-II:Beck Depression Inventory-II.RSES:Rosenberg Self-Esteem Scale. SWLS:Satisfaction with Life Scale. T1: First stage (initial assessment). T2:Second stage (revaluation). Pre- RPPT: Pre- Repeating Phrases of Positive Thoughts. Post- RPPT: Post- Repeating Phrases of Positive Thoughts.
*p<0.05, **p<0.01, ***p<0.001, £p>0.05
p*: Test de Wilcoxon. ES: effect size. SRM: standardized response mean. |
Table 1 Effect of TRPPT on MWD.
TRPPT and depression-BDI-II and DASS-21
At the measure of depression, measures pre- and post-treatment showed significant differences in the experimental group (Table 1 and Figure 1). Participants (students and MS patients) in the experimental group also exhibit less depression following the RPPT protocol (p<0.001, p<0.05).
In general, results of experiments show an effect of RPPT protocol among students and MS patients on variables such as stress, and anxiety. It’s also observed a decrease in depressive symptoms.
TRPPT, RSES and SWLS
At the measure of self-esteem and satisfaction with life, measures pre- and post-treatment showed significant differences in the experimental group (Table 1 and Figure 1). Participants (students and MS patients) in the experimental group also improved selfesteem and satisfaction of life following the RPPT protocol (p<0.001, p<0.05).
Sizes effect and responsiveness
In this study, the benefit of the RPPT was estimated by the effect size (ES) and standardized response mean (SRM). An effect size or larger standardized response mean suggests greater sensitivity to change of the tool. The standardized response mean (SRM) is calculated by dividing the mean difference in scores by the SD of the difference scores. The ES and SRM can be interpreted as small (0.2-0.49), moderate (0.5-0.79), and large (≥0.8). Effect sizes t students test calculated for each instrument is large (>0.80) between T1 and T2 (Table 1 and Figure 1). According to the criterion of Cohen "d", the short-term effect is RPPT large and significant. SRM and its interpretation thresholds show that sensitivity to change (responsiveness) for depression, stress, anxiety, self-esteem and satisfaction with life are large (Table 1 and Figure 1).
Discussion
This research aims to study the effects of the treatment of the RPPT on a group refugees and people subjected to war, very few people solicited so far in the literature.
The results of this research show effectiveness TRPPT protocol on the mental health of a people (patients and students) in the war. These results are consistent with a large body of research on the psychotherapeutic approach conducted with refugees torture survivors as BCT [38].
Research has shown that the amendments on negative thoughts are ways to treat depression [54,55], Other research has shown that positive thoughts have the important role on psychological troubles [13,56]. So, our results show that using positive thoughts are ways to treat depression and other MWD (ANX, STR, LSE (low self-esteem) and DSIV (dissatisfaction in life). According to our results, positive automatic thoughts and RPPT are absent in cognition depressive, anxious and stressed subjects. The presence of positive automatic thoughts is then an aspect of positivity in cognition that can reduce MWD in anxious and depressive stressed subjects.
Before TRPPT, Syrian refugees populations war victims (students and MS patients) have a high level of depression, anxiety, stress, and a low level of self-esteem and Satisfaction with Life. After TRPPT, Syrian refugees populations war victims have a low level of depression, anxiety, stress, and a high level of self-esteem and satisfaction with life. In other words, psychological and mental disorders decreased and psychological well-being increased with the TRPPT.
We can interpret these results depending on the positive psychological outcomes of the “process of RPPT” which can introduce many “positive feelings”, such as: comfortable, relax, and the feelings of trust and hopefulness and these positive feelings support emotional vitality and happiness. These results are consistent with other research [57,58]. Repeatedly, a person can get “positive emotional state” which can reduce the common negative feelings in depression, anxiety and stress.
According to our results, by thinking positively, people who perceive the stress and stressful life as less threatening, are able to cope with it effectively. People who think negatively do not expect things to go as planned therefore anticipating bad outcomes. Their coping with daily stressors becomes dysfunctional and they develop psychological and physical health problems while positive thinkers encounter circumstances with optimism and if they encounter stressful situations they appraise it as controllable and use coping strategies that are functional, efficient and problem focused. They feel that life is going well, their goals are being met, and resources are adequate [59,60]. The effective coping with stress enable the person to have a lot of positive experiences, which become "functional information" in future [61] and this can support “positive self- image” and “positive future- image”, which are the opposite images of those are common in depression.
Our research has shown that mental-war disorders in Syrian refugees with physical illness and /or without physical illness is associated with a view of the future characterized by reduced anticipation of future positive experiences, but also necessarily increased anticipation of future negative experiences. The control group not following the RPPT anticipated significantly fewer future positive events than the experimental group following the RPPT. The group with mental-war disorders was characterized by a lack of positive thoughts about the future, but also an increased number of negative thoughts. Psychological models of depression, anxiety, stress, low self-esteem, and dissatisfaction in life have long recognized the important role of positive future cognitions in emotional disorder, and the way in which people with mental-war disorders think about their future is an interesting area for study.
According to Hurt et al. [62] therapeutic interventions should focus on enhancing positive perceptions of chronic illness. Our study showed that positive thoughts about illness but also in the war will develop optimistic outlook associated with increased well-being across a range of health conditions. Holding positive perceptions predicted better well-being. TRPPT and /or positive thoughts appears to provide protection against some negative perceptions of mental-war disorders and was associated with better mood and health-related quality of life (HRQoL).
Conclusion
This study suggests that RPPT treat the depression, stress, anxiety, low self-esteem, and dissatisfaction in life. The results show that TRPPT are important in treat mental-war disorders (MWD).
The TRPPT allows significantly reduce depressive symptoms, anxiety and stress, with a short-term effect maintained. The results of this study lead us to offer an appropriate treatment, may prevent chronicity and complications. It is therefore plausible that the fact to act on positive thoughts modifies depression and other MWD since they are characterized by interdependence.
The TRPPT improve the quality of life, mental health and adaptation to the social and professional environment among refugees and people subjected to war. The TRPPT used to help these people improve their concentration, confidence, selfesteem, regulate effort and academic work and monitor cognitive and emotional reactions.
Treatment by Repeating Phrases of Positive Thoughts in War in Syria (War without Compassionate)
In this experimental study has shown that positive thinking effects the appraisal and treatment of MWD and stress, which determines our coping strategies.
Thus the result in this study supports the researchers' conceptual model that positive thinking increases the ability to deal with stressors effectively and causes many successful health outcomes among refugees and people subjected to war.
In Syria where negativity due to illiteracy and poverty is prevailing everywhere in these moments because of the war. Geopolitical situations in the country are alarming and people are under constant strains of bomb blasts. In these circumstances there should be measures to protect them from negativity. There are implications for educationists and clinicians who wish to reduce the stressors of their students and patients by preparing them to face the challenges of teaching-learning situations and professional life, etc. Educationists and clinicians can initiate programs to cultivate positive thinking in their students and patients. Positive thinking interventions should focus on how learners can identify their strengths, adopt new practices and habits, and restructure their lives in ways that allow for a stream of positive emotions and experiences.
Furthermore, many of the characteristics observed in positive thinkers can help them improve their conditions as well as others. These findings can also be used by the counselors to reduce their clients’ negativity by inducing positive thinking in them. Community members can change negative perceptions of the people into positive ones to make them healthy and productive citizens of Syria and other unstable countries like Iraq etc.
The TRPPT help refugees populations war victims to develop a more optimistic attitude in general. Those refugees with very negative perceptions of life and illness during the war and a very pessimistic attitude should specifically be targeted as these refugees are most at risk of poor psychological well-being and health-related quality of life. The findings have significant implications for clinical practice and therapeutic interventions for refugees populations war victims not only with students but also with other chronic degenerative diseases (MS). This study said RPPT have been associated with increased wellbeing across a range of health conditions during the war. However, this study warned that it would be wrong to encourage “potentially overenthusiastic views or unrealistic positive health beliefs”. TRPPT to challenge negative thinking would be one potential treatment.
TRPPT and Relationship Difficulties
In terms of mental health and coping, refugees and people subjected to war with significant relational difficulties with family are twice as likely as others to evoke a real psychological suffering. MWD (e.g. depression) among them can have negative impacts on social and relational situation. Our result shows that TRPPT reduce the intensity of depression, also anxiety and stress, and raises self-esteem, and satisfaction in life. This could well improve social relations of refugees and people subjected to war with their surroundings (e.g.: “There are many people who care about me”) [2,63-68].
Recommendations
RPPT (Repeating Phrases of Positive Thoughts) must begin at an early age, i.e. from primary school or earlier. This RPPT help to people to confront the bad conditions and psywar trauma, to avoid and confront unexpected situations like war, coup and to increase awareness and good citizenship culture among people
Future Prospects and Researches
Treatment by Repeating Phrases of Positive Thoughts (TRPPT) originated as a treatment for emotional disorders (depression, anxiety and stress) among French students by Alsaleh in 2016. However, it is increasingly used to help people with chronic illnesses manage symptoms and improve psychosocial outcomes, such as depression and quality of life. Alsaleh is in the process of reproduce the work and its results on a clinical sample at the Hospital of Caen, especially patients with renal impairment. The TRPPT will be reused and reapplied to these patients. In addition, we will study the most activated brain areas when patients practice the RPPT. TRPPT may be effective in treating mentalwar disorders in refugees populations war victims and may be an alternative or adjunct to pharmacological treatment. TRPPT is an effective treatment for depression, anxiety, stress, low self-esteem, and dissatisfaction in life in war. Further research should explore optimal durations and modalities of treatment for refugees populations war victims with different characteristics.
For this, we recommend researchers to use and examine the TRPPT in refugees populations war victims with mental-war disorders, in addition of physical illnesses. In this article, we focus on uses of TRPPT in refugees with mental-war disorders.
The TRPPT is now reapply on children, the patient chronic renal failure, and other samples
Conflict of Interest
All the authors declare that they have no conflicts of interest with respect to this study or its publication.
Acknowledgments
The authors thank all the participants in this study.
I am very happy [47].
Life is beautiful.
I have energy.
I sleep well.
My health is improving. |
There are many people who care about me[66].
My positive attitude will be beneficial to my health and my day[65].
I think positively all the time [67]. |
I try to see it in a different sight, to make it seems more positive [59].
I feel good[47].
I am proud of me[47]. |
I will succeed [66].
I'm in a good mood [66].
I have many good qualities[66]. |
I am very relaxed[66].
I am satisfied of my appearance [66].
I pamper myself[66]. |
I have a good sense of humor [66].
I have several useful qualities[66].
Today I will accomplish much things[66]. |
I'm warm[47].
I feel comfortable in life[66].
I can accomplish anything, I know I'll get there[66]. |
Annex 1 List of positive phrases used
Annex 2 Instructions given to subjects in the first training session.
Depression is a common condition in the general population. It can affect anyone (regardless of age, gender, social status, education, economic level, environment ...) but it is the most common among MS patients and students. Indeed, over a third of students and more 50% patients with MS are affected by depression. Depression among students and patients has negative consequences on social and family relationships, education, quality of daily life (emotional, intellectual functioning, physical fitness, vital and body mechanisms and social and academic life).
According to Beck and Bredemeier [63] , depression is an adaptation to the perceived loss of vital human resources that provide access to the necessities of life or basic needs of life (including the loss of a member of the family, a romantic partner, a peer group or membership, employment, health). According to Beck and Bredemeier [63], the primary function of the “depression program” is to promote energy conservation to face the perceived loss of resources. This program can be stopped when vital resources are restored, or because of new information emerge that "correct" bias and/or negative bias or because the situation changes. External factors such as the support of friends and family, the advice of a psychotherapist and biological treatment (e.g. medications) can help to stop the cycle of depression. Especially among patients in the first years with MS and among students in the first year, the time of life that can be considered as a kind of crossroads and opportunities in life of an individual, commits its psychological resources, personal, family and environmental which, if they are insufficient to confront the state of stress and / or anxiety and depression. These situations are numerous: the young adult who returns to college, or who undertakes steps to get a job, or one that is facing problems of technological change or periods of unemployment ... All these events life are opportunities for new experiences as potential sources of stress, depression and anxiety seeking resources to address it.
It is very important to treat depression among MS patients and students. Depression is misdiagnosed and mistreated. Depressive students have more difficulties in their studies. Depression can compromise adherence to disease-modifying medications. Depression is a curable disease today. The treatment of depression in MS patients and also in students has positive effects on daily activities, work, social and family relationships, quality of life, improving education, reducing fatigue...
Positive thinking affects self-image, self-esteem, creating a sense of selfacceptance and self-love. It also affects confidence.
So that the RPPT is a force, it must master.
• As soon as you start to have negative thoughts that invade your mind, you say "STOP".
• When a negative thought crosses your mind, detect it and train yourself to formulate the idea positively.
Example: Negative thought: I'm tired. ///// Positive thinking: Don't say: I’m not tired. Instead you can say: "I need to sleep". Because the brain does not distinguish between positive words and negative words, it absorbs all the words and stored.
• All negative thoughts must be transformed into positive ones: these positive thoughts can be either purposeful or teaching. •• The motivating positive thoughts are useful when you need to extend effort in time or that it takes you a lot of energy (e.g. academic work, revision of exams...). •• Educational positive thoughts may be technical but are required to orient and fix your attention on a goal set up directly in the field (e.g. exam success, organizing time, work, behavior, social relationships, communication, citizenship...)
• To be able to properly manage your internal dialogue and be positive, it is important to diagnose the cause negative thoughts and positive thoughts.
17649
References
- Acarturk C, Konuk E, Cetinkaya M, Senay I, Sijbrandij M, et al. (2015). EMDR for Syrian refugees with post-traumatic stress disorder symptoms: results of a pilot randomized controlled trial. Eur J Psychotraumatol6: 27414.
- Quosh C, Eloul L, Ajlani R (2013) Syria - Refugees and Displaced in the past and current crises: Systematic Review Assessing the Mental Health Profile and System. International Journal of Mental Health, Psychosocial Work &Counselling in Areas of Armed Conflict 11.
- McKenzie ED, Spiegel P, Khalifa A, Mateen FJ (2015) Neuropsychiatric disorders among Syrian and Iraqi refugees in Jordan: a retrospective cohort study 2012-2013. Conflict and Health9:10.
- Orient Net (2016) Syrianrefugees face depression, mental illnessamongseries of trauma.
- Murray A,Raskind MD (2009) Diagnosis and Treatment of Depression Comorbid with Neurologic Disorders. Am J Med 121: S28-S37.
- Mohr DC, Hart SL, Julian L, Tasch ES (2007) Screening for depression among patients with multiple sclerosis: two questions may be enough. MultScler 13:215-219.
- Beck AT (1967) Depression: Causes and treatment. Philadelphia: University of Pennsyvania Press.
- Kendall PC (1984) Cognitive processes and procedures in behavior therapy Annual review of behavior therapy: Theory and practice New York: Guilford Press 9: 32-179.
- McGuigan C, Hutchinson M (2006) Unrecognized symptoms of depression in a community based population with multiple sclerosis. J Neurol253: 219-223.
- Bartha C, Parker C, Thomson C, Kitchen K (1999) Depressive Illness: A Guide for People with Depression and Their Families. Centre for Addiction and Mental Health.
- Matile PA (2007) La vulnérabilité dépressive. Psychiatrie et psychothérapie d’enfants et d’adolescents FMH.
- Csillik A, Aguerre C, Bay M (2012) Psychothérapie positive de la dépression: spécificités et apports cliniques. Annales Médico-Psychologiques 170: 541-546.
- Alsaleh M (2016) Analyse psychosociale et cognitive de la santé mentale chez les étudiants de première année : Validation du questionnaire des pensées positives et négatives et du questionnaire de la dépression de Beck; Effet des pensées positives et des facteurs psychosociaux. laboratoire du CERReV (EA 3918), Université de Caen Normandie.
- Martins da Silva A(2011) Depression and anxiety in a Portuguese MS population: Associations with physical disability and severity of disease. J NeurolSci306: 66-70.
- Ziemssen T (2009) Multiple sclerosis beyond EDSS: depression and fatigue. JNeurolSci 277: 37-41.
- Benedict RHB, Wahlig E, Bakshi R, Fishman I, Munschauer F, et al. (2005) Predicting quality of life in multiple sclerosis: accounting for physical disability, fatigue, cognition, mood disorder, personality, and behaviour change. J NeurolSci 231: 29-34.
- Lobentanz IS, Asenbaum S, Vass K, Sauter C, Klosh G, et al. (2004) Factors influencing quality of life in multiple sclerosis patients: disability, depressive mood, fatigue and sleep quality. ActaNeurolScand 110: 6-13.
- Mohr DC, Goodkin DE, Likosky W, Gatto N, Baumann KA, et al. (1997) Treatment of depression improves adherence to interferon B-1b therapy for multiple sclerosis. Arch Neurol 54: 531-533.
- Stenager EN, Stenager E, Koch-Henriksen N, Bronnum–Hansen H, Hyllested K, et al. (1992) Suicide and multiple sclerosis: an epidemiological investigation. J NeurolNeurosurg Psychiatry55: 542-545.
- Sadovnick AD, Eisen K, Ebers GC, Paty DW (1991)Cause of death in patients attending multiple sclerosis clinics. Neurology4: 1 1193-11196.
- Ossowska K, Lorenc-Koci E(2013)Depression in Parkinson's disease. Pharmacol Re65: 1545-1557.
- Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE (2005)Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 62: 617-627.
- Chabrol H, Choquet M (2009) Relations entre symptomatologie dépressive, désespoir et idées de suicide chez 1547 lycéens. L’Encéphale 35: 443-447.
- Alsaleh MA (2016) Therapy mental and psychological troubles (MPSYT) by Repeating Phrases of Positive Thoughts (TRPPT) with Women. Intercultural Comparison: Middle East and Europe, war and peace. A controlled and randomized study-Cognitive therapy & Positive psychotherapy. Journal of Psychology and Cognition 1.
- Mohr DC, Likosky W, BertagnolliA , GoodkinD,Van Der Wende J, et al. (2000) Telephone-administered cognitive-behavioral therapy for the treatment of depressive symptoms in multiple sclerosis. J Consult ClinPsychol68: 356-361.
- Mohr DC, Goodkin DE, Islar J, Hauser SL, Genain CP (2001)Treatment of depression is associated with suppression of non-speci?c and antigen-speci?c TH 1 responses in multiple sclerosis. Arch Neurol58: 1081-1086.
- Mohr DC, Hart SL, Julian L (2005) Telephone-administered psychotherapy for depression. Arch Gen Psychiatry62: 1007-1014.
- Thomas PW, Thomas S, Hillier C, Galvin K, Baker R (2006) Psychological interventions for multiple sclerosis. Cochrane Database of Systematic Reviews.
- Dyer J, Ehde DM (2010) Multiple Sclerosis: Depression. International Encyclopedia of Rehabilitation.
- Baker B (1992) Psychological consequences for tortures refugees seeking asylum and refugee status in Europe. In M.BasogluToture and its consequences: current treatment approaches NY, USA: Cambridge University Press p: 106.
- Gerrity E, Keane TM, Tuma F (2001) The mental health consequences of torture DonaldMeichenbaum. New York: Kluwer Academic/Plenum .
- IRCT (2010) About refugees, asylum seekers, IDPs and torture. Copenhagen: IRCT.
- IRCT (2011) Up to 35% of refugees are torture victims, highlights the IRCT on World Refugee Day. Copenhagen: IRCT.
- Williams AC, De C, Pena CR, Rice ASC (2010)Presistent pain in zurvivors of torture: acohort study. J Pain Symptom Manage 40: 715-722.
- OFPRA (2014) Rapport d'activite 2013 Fontenay-seus-Bois: Office francais de protection des refugies et des apatrides.
- UNHCR (2013)Asyslum levels and trends in industrialized Europe and selected non-European counties. Geneva, Switzerland: United Nations High Commissioner for refugeez.
- De Fouchier C, Blanchet A, Jehel J (2015)Cognitive and behavioral therapy with refugees torture survivors: A literature review. Journal de thérapie comportementale et cognitive 25: 12-20.
- Steel Z, Chey T, Silove D, Marnane C, Bryant RA et al. (2009)Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: a systematic review and meta- analysis. JAMA 302: 537-549.
- Fazel M, Weeler J, Danesh J (2005) Prevalence of serious mental disorder in 7000 refugees resetlled in western countries: a systematic review. Lancet 365: 1309-1314.
- Bisson J, Ehler A, Matthew R, Pilling S, Richards D, Turner S (2007) Psychological treatment of chronic post-traumatic stress disorder (PTSD). Systematic review and meta- analysis. Br J Psychiatry 190: 97-104.
- Bisson J, Andrew M (2005) Psychological treatment of post-traumatic stress disorder (PTSD). Cochrane Database Sys Rev Online 2005 2. CD 003388.
- Bisson J, Andrew M (2009) Psychological treatment of post-traumatic stress disorder (PTSD). Cochrane Database of Systematic Reviews 18: CD003388
- Foa EB, Keane TM, Friedman MJ, Cohen JA (2005) Practice guidlines from the International Society for traumatic stress studies New York: Guilford Press.
- National Institue for Clinical Excellense (2005) Post-traumatic stress disorder (PTSD): The management of PTSD in adults and children in primary and secondary care. London: National Institue for ClinicalExcellense.
- Hollon SD, Kendall PC (1980) Cognitive self-statements in depression: development of an Automatic Thoughts Questionnaire. Cognitive Therapy and Research 4: 383-395.
- Kendall PC, Howard BL, Hays RC (1989) Self-referent speech and psychopathology: the balance of positive and negative thinking. Cognitive Therapy and Research 13: 583-598.
- Alsaleh MA, Kubitary A (2016) Validation of the Automatic Thoughts Questionnaire-18 item- Multiple Sclerosis-Arabic (ATQ-18-MS-Ar) Among Multiple Sclerosis Patients. Journal of Psychology and Cognition 1.
- Beck AT, Steer RA, Brown GK (1996) BDI-II Manual. London: The Psychological Corporation.
- Lovibond SH, Lovibond PF (1995) Manual for the Depression Anxiety Stress Scales (2nd ed.). Sydney: Psychology Foundation.
- Taouk M, Lovibond PF, Laube R (2001) Psychometric properties of an Arabic version of the Depression Anxiety Stress Scales (DASS21). Report for New South Wales Transcultural Mental Health Centre, Sydney: Cumberland Hospital.
- Rosenberg M (1989) Society and the adolescent self-image. Middletown, CT: Wesleyan University Press.
- Diener E, Robert A, Emmons RJL, Grif?n S. (1985)The Satisfaction with Life Scale. J Pers Assess 49: 71-75.
- Beck AT, Rush AJ, Shaw BF, Emery G (1979) Cognitive therapy of depression. New York: Guilford Press.
- Hollon SD, Beck AT (1979)Cognitive therapy of depression. In P.C. Kendall & S.D. Hollon (Eds.), Cognitive—behavioral interventions: Theory, research and procedures. New York: AcademicPress.
- Kirkegaard-Weston E (2005) Positive Thinking: Toward a Conceptual Model and Organizational Implications.Honors College Thesesp: 15.
- Pieffer V (1989) Positive thinking. Great Bretain: Element Books Limetid, Shaftesbury Dorset.
- Rimer S (2011)The biology of emotion—and what it may teach us about helping people to live longer. Harvard School of Public Health.
- Carver CS, Scheier MF (1998)On the self regulation of behavior. New York: C.
- Cantor N, Norem J, Langston C, Zirkel S, Fleeson W, et al. (1991) Life tasks and daily life experience. Journal of Personality 59: 425-451.
- Shapiro F ,Kaslow F, Maxfield L (2007) Handbook of EMDR and fmily therapy processes. NJ: John Wiley & Sons, Inc.
- Hurt CS, Burn DJ, Hindle J, Samuel M, Wilson K , et al. (2014) Thinking positively about chronic illness: An exploration of optimism, illness perceptions and well-being in patients with Parkinson's disease. Br J Health Psychol 19: 363-379.
- Beck AT, Bredemeier K (2016) A unified model of depression: Integrating clinical, cognitive, biological, and evolutionary perspectives. Clinical Psychological Science. Advance online publication.
- Carver CS, Scheier MF, Weintraub JK (1989)Assessing coping strategies: A theoretically based approach.J PersSocPsychol 56: 267-283.
- Greer S, Watson M (1987) Mental adjustment to cancer: Its measurement and prognostic importance. Cancer Surv 6: 439-453.
- Ingram RE, Wisnicki KS (1988) Assessment of positive automatic cognition. J Consult ClinPsychol56: 898-902.
- Temoshok L, Dreher H (1992) The Type C Connection: The Behavioral Links to Cancer and Your Health. New York: Random House.
- Wilkinson S, Kitzinger C (2000) Thinking differently about thinking positive: a discursive approach to cancer patients talk. SociScieMedi 50: 797-811.

