Keywords
Nutrition, Carbohydrates, fats, Proteins, Vitamins, Minerals
Introduction
The World is in the midst of an unprecedented 'exercise?boom', reflected by the ever?growing number of people engaged in some form of physical activity for pleasure as well as health. Indeed, while for many decades it was almost prohibited in patients with certain medical conditions (e.g., heart disease, rheumatoid arthritis, and diabetes), it has now become apparent that physical activity is an important element of the rehabilitation process in such medical conditions [1,2]. However, fundamental to these issues are the nutritional status and dietary intakes of the exercising individuals. It has been established that diet can affect physical performance and health in both athletes [3] and non?athletes [4,5].
Citizens of industrialised countries tend to regard the intake of food in a rather passive manner. This seems to be the result of a general lack of understanding of what constitutes optimal nutrition, and how the latter regulates our bodily functions. Some of the food we eat is used to build, maintain or repair the body cells, while the majority is processed (i.e. metabolised) for energy (ATP) production [6,7]. Most of this energy appears as heat and is used to keep the body warm; some is used for work of cells, and some for muscular work. Body building requirements determine the quality of diet, whereas the energy needs of the individual determine the quantity of diet [8,9]. Therefore, optimal nutrition is a dietary balance of different nutrients to keep the bodily functions at the required levels. In the watery medium of the cell, delicate blending of carbohydrates, proteins and fats, along with vitamins and minerals make it possible. In this chapter, aspects related to these nutrients will be briefly discussed.
Carbohydrates
Carbohydrate is the body's preferred energy source, and the most important fuel for the working muscle. During exercise of high intensity and brief duration, this nutrient provides most of the energy needs [10]. As a practical rule, both men and women should eat 7?10 g of carbohydrate per kg body weight per day [11]; each gramme of carbohydrate will produce 4 calories of energy and in the process will use 0.7 litres of oxygen.
Carbohydrates should constitute around 60% of the total daily energy intakes. Carbohydrates are stored as glycogen in the liver (80?100 g) and in the muscle (300?400 g); both stores can be exhausted by hard exercise; the entire store of this fuel in the body will last for about 100 minutes of strenuous steady paced cycling, running, dancing, etc. Liver glycogen can be made available to muscle when it is broken down to glucose and then released into the blood. This blood glucose is also taken up and used by many other tissues, including the brain, while liver glycogen content falls rapidly if no food is consumed.
Scientists agree that increased stores of muscle glycogen can enhance physical performance in terms of its intensity and duration [12]. However, muscle glycogen is utilised rapidly during intense exercise, and fatigue occurs when it is depleted to low levels [13]. Muscle glycogen is restored at a rate about 5% per hour. Thus, provided that an appropriate diet is used, it takes at least 20 hours to fully replenish stocks. However, during the first 1½ hours after exercise glycogen is restored at faster rates (7+%).
Carbohydrates can be found in two food?groups. One group would include complex (or 'slow') carbohydrates, such as unrefined grains, potatoes, and fruits. However, the general desire to choose sweet and palatable foods has led to the formation of the second food?group containing simple (or 'fast') carbohydrates, such as refined flour and sugar. In these carbohydrates, vitamins, mineral salts, and trace elements are often reduced, or missing. Over?consumption of refined carbohydrates can impose a pathogenic strain on the pancreas ? among other organs ? and thus may be the essential cause of 'diabetes mellitus' (or an inability to control blood glucose) [14].
Approximately 40g of sugar can be swallowed in a single can of cola drink in one to two minutes. For the same 40g of sugar to be ingested in unrefined form, one has to chew 330g of, say, apples in about 10?15 minutes. However, the type and/or volume of carbohydrate are normally associated with insulin release, which facilitates the storage of excess sugar as liver glycogen, thus, maintaining optimal blood sugar levels. For example, whole grain food, cereals, pasta, fruit and vegetables have a low glycemic response (or the rate of glucose absorption) compared with the white bread standard. Foods such as honey and processed cereals have relatively high glycemic response. Consuming, for instance, a rapidly digested chocolate bar would cause a great glycemic response, i.e., rapid and high blood glucose rise and a corresponding high insulin response; as a result, sometimes there is a rebound hypoglycemia, which can lead to fatigue during physical exertion [15?17].
Fats
Fats (or lipids) serve a variety of functions, including all three purposes of nutrition: to form and maintain body structures, to regulate metabolism, and to provide the second main source of energy. The importance of fat as an energy source depends on the intensity of exercise as well as on the availability of carbohydrates [18]. Fats are used along with carbohydrates when the body performs low intensity/long duration type of work, thus, sparing the store of carbohydrate; the fitter the athlete the greater the carbohydrate sparing. However, if the body starts to run low on carbohydrate it will increase its use of fat. This may affect physical performance as fat utilisation is generally associated with low intensity muscular activity.
Fat, stored as triglyceride in the adipose tissue (i.e., fat cells), is mobilised by lipolysis to provide free fatty acids which are released into blood and, therefore, transported to the active muscle; the process of free fatty acid transport is stimulated by the hormones adrenaline and noradrenaline [19?21]. Under normal conditions, the body's stored fat could provide energy for continuous exercise lasting for several days, unlike the carbohydrate stores which would last less than 2 hours. If fat was the only substrate, this would theoretically enable individuals to exercise continuously at marathon speeds for more than 70 hours [22].
Fats provide 40?45% of the total daily energy intake in sedentary people living in industrialised countries [23]. Athletes are generally advised to reduce fat intakes to 20?30%, with a simultaneous increase of carbohydrate intakes. It should be noted, however, that the body will convert excess amounts of carbohydrates and proteins into fat if caloric expenditure is less than caloric intake. Research has indicated the potential health and fitness related benefits of ingesting an omega?3 family of fatty acids found mainly in the oils of fish, such as mackerel. Increased intakes of omega?3 fatty acids may prevent blood clotting, contribute to lower blood pressures, and result in better red blood cell plasticity [24,25].
The fat content in foods can vary from 100% (eg, cooking oils), to minor amounts of less than 5?10% in most fruits and vegetables. In foods such as butter, margarine, and mayonnaise, fat has an obvious high content. However, in other foods, the fat content may be high but not as obvious; this is known as hidden fat (e.g. nuts, and commercially prepared potato chips). It would be interesting to note, for example, that while 142g baked potato contain 145 calories, the same 142g of fried potato chips contain 795 calories!
Proteins
Protein is one of the most essential and multi?purpose nutrient, as it has a wide variety of physiological functions associated with optimal physical performance and health [26,27]. Protein forms the structural basis of muscle tissue (which is the largest protein pool within the body), it is involved in growth and repair of damaged tissue, and has a role in the metabolic process that converts both carbohydrate and fats into energy. If carbohydrate and fat fail to provide enough energy, protein will be switched on to provide any extra energy.
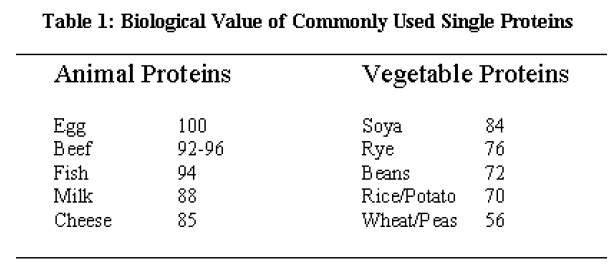
Protein is broken down into amino acids. There are 25 main amino acids; 8 of them (called essential amino acids) cannot be manufactured in the body and have to be found in our food. Animal sources such as meat, fish, eggs and/or dairy products are often referred to as 'complete protein foods' as they contain all of the 8 essential amino acids, and therefore, higher biological value (Table 1). Vegetable sources are described as being 'incomplete' as they lack at least one of the essential amino acids.
The human body has no protein reserve/store comparable to its large energy stores of fat and moderate stores of glycogen. So, optimal levels of protein should be maintained in the dancers' body. The average person needs 0.8 g of protein per kg of his/her body?weight per day, which provides 10? 15% of total daily energy intakes. However, individuals who engage in repeated, high intensity physical activities of up to several hours, would probably benefit from an increased protein intake of 1?2 g of his/her body?weight [28]; elite performers in sports which require to build muscle bulk, may need up to 4 g per kg body?weight [29]. It is generally agreed that most conventional diets provide more than 4 g of protein per kg body?weight per day, and that protein supplements are not required. The above may not be applicable to individuals who consume low caloric diets (e.g., gymnasts), or to those who have relatively low daily protein intakes, because of the reduced protein density in their diets (e.g., vegetarians). Even if protein sources are appropriately mixed, vegetarians should consume approximately 10?20% more protein due to differences in digestibility between vegetable and animal protein sources. In such cases, protein supplementation may be necessary for maintaining an optimal nitrogen balance and for reducing impairment in training status. Excess protein intake, is used as energy, converted to fat and stored, or excreted.
Vitamins
Although most of the 13 known vitamins cannot be synthesised by the human body, they are nevertheless essential for maintaining optimal bodily function [30]. These nutrients contribute to the various chemical processes which regulate metabolism, release energy and repair tissue. Vitamins are either water?soluble or fat?soluble in nature.
The 9 water?soluble vitamins (i.e., C, B1, B2, B6, B12, niacin, pantothenic acid, folic acid, and biotin) have an important role in protein metabolism. They are not stored in the body?tissues to any appreciable extent, they are depleted as a result of strenuous exercise [31], and they are easily destroyed in processing and cooking [32]. These vitamins can be mainly received through fresh fruit and vegetables. Apart from vitamin C, excess supplementation can aggravate existing medical conditions [33]. The 4 fat?soluble vitamins are A, D, E, and K. Daily ingestion of these vitamins is not necessary, given that they are normally stored in the liver and in the fat cells of the adipose tissue. As in the case of water?soluble vitamins, excess intake of fat?soluble vitamins can produce toxic effects [33].
Foods that are rich in vitamins C and E may provide some protection against cancer and heart diseases. These vitamins serve as antioxidants to counter the damaging effects of the reactive chemicals known as free radicals, on the cell membranes [34]. Preliminary research has also shown that increased incidence of musuloskeletal injuries may be due to low levels of vitamins C and E. Citrus fruits, cabbage, and broccoli are good sources of vitamin C; E can be obtained from vegetable oils and green leafy vegetables. However, there is only limited evidence that intakes above the recommended daily allowance are beneficial [35]. In general, most studies have revealed that active individuals are receiving the recommended daily allowance for vitamins through their normal diets. Nevertheless, individuals who are on weight?reduction programmes, or on low body?weight maintenance programmes may not receive adequate vitamin nutrition.
Minerals
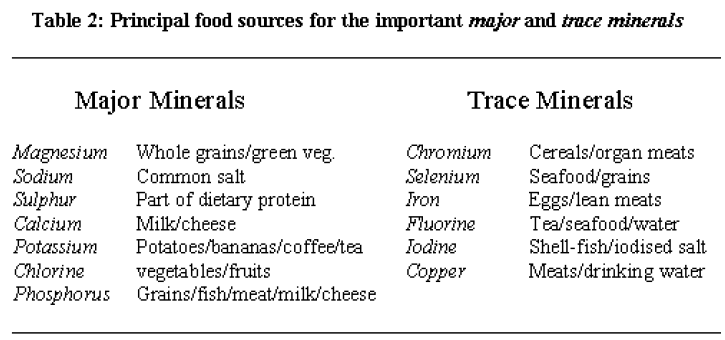
The body is composed of at least 31 known chemical elements. The most abundant non?metal chemical element is oxygen which amounts to 65% of a person's body weight. Three other non?metal elements constitute 31% of the body mass; these are carbon (18%), hydrogen (10%), and nitrogen (3%). The remaining 4% of our body weight is composed of a group of 22 metallic elements called minerals. These minerals can further be classified into major minerals and trace minerals (Table 2).
Minerals are essential substances for the musculoskeletal system as well as for numerous biological functions. For instance, insufficient supply of calcium and phosphate is normally associated with impaired skeletal development, and with increased incidences of bone and muscle injuries [36,37]. Together with vitamins, minerals are also necessary for the efficient extraction and utilisation of energy form carbohydrates, fats, and proteins, and they play important and highly specific roles in activating energy transfer throughout the body. The bulk of this 'metabolic' mineral pool is present in blood plasma and interstitial fluid, and represents a tiny fraction of total mineral content found in healthy individuals.
Most minerals are bound to or are part of functional structures and/or systems of the human body. For instance, 80% of the 3?5 g of the iron contained in the body is actively combined with haemoglobin in the red blood cells, and which can increase the oxygencarrying capacity of blood about 65 times. Regarding calcium, the body contains about 1,200 g of which approximately 99% is built into the skeleton [38]; the remaining 1% represents the metabolically available pool of this mineral, much of it in muscle.
Humans obtain their mineral nutrition from both plants and animals. Drinking water is also an excellent source of many minerals. Healthy and physically active people who eat well?balanced meals consume enough of the essential mineral elements to maintain proper physiological functioning [38,39]. However, supplementation may also be necessary in individuals on diets with restricted intakes of dairy foods [40,41]; 75% of dietary calcium usually comes from dairy products.
The minerals sodium, potassium, and chlorine have quite similar functions and they are collectively called electrolytes. The major function of electrolytes is to control and maintain the proper rate of fluid exchange within the body. When sweating excessively, the body loses the electrolytes present in sweat, leading to impairment in exercise performance. One litre of sweat loss is accompanied by a loss of about 1.5 grammes of salt. It is common, therefore, for active individuals to increase their normal salt intake to offset the effects of dehydration [42,43].
Conclusion
In the watery medium of the cell, delicate blending of carbohydrates, proteins and fats, along with vitamins and minerals is necessary to keep the bodily functions at the required levels. Healthy individuals who eat well?balanced meals consume enough of these nutrients and there is no need for supplementation. However, prolonged deficits in any of the nutrients can cause health and physical performance impairments.
3697
References
- Braun M U, Rauwolf T, Zerm T, et al. Long term biventricular resynchronisation therapy in advanced heartnfailure: effect on neurohormones. Heart 2005; 91(5): 601‐5
- Eurenius E , Stenstrom C H. Physical activity, physical fitness, and general health perception amongnindividuals with rheumatoid arthritis. Arthritis Rheum 2005; 53(1): 48‐55
- Montero A, Lopez‐Varela S, Nova E, et al. The implication of the binomial nutrition‐immunity onnsportswomen's health. Eur J Clin Nutr 2002; 56 Suppl 3: S38‐41
- Johansen K L, Kaysen G A, Young B S, et al. Longitudinal study of nutritional status, body composition, and physical function in hemodialysis patients. Am J Clin Nutr 2003; 77(4): 842‐6
- Johansen K L, Chertow G M, Ng A V, et al. Physical activity levels in patients on hemodialysis and healthynsedentary controls. Kidney Int 2000; 57(6): 2564‐70
- Bohnsack B L , Hirschi K K. Nutrient regulation of cell cycle progression. Annu Rev Nutr 2004; 24: 433‐53
- Sudi K, Ottl K, Payerl D, et al. Anorexia athletica. Nutrition 2004; 20(7‐8): 657‐61
- Helge J W. Long‐term fat diet adaptation effects on performance, training capacity, and fat utilization. Med ScinSports Exerc 2002; 34(9): 1499‐504
- Liu S , Manson J E. Dietary carbohydrates, physical inactivity, obesity, and the 'metabolic syndrome' asnpredictors of coronary heart disease. Curr Opin Lipidol 2001; 12(4): 395‐404
- Burke L M, Kiens B , Ivy J L. Carbohydrates and fat for training and recovery. J Sports Sci 2004; 22(1): 15‐30
- Brewer J, Williams C , Patton A. The influence of high carbohydrate diets on endurance runningnperformance. Eur J Appl Physiol Occup Physiol 1988; 57(6): 698‐706
- Costill D L. Carbohydrate for athletic training and performance. Bol Asoc Med P R 1991; 83(8): 350‐3
- Febbraio M A , Dancey J. Skeletal muscle energy metabolism during prolonged, fatiguing exercise. J ApplnPhysiol 1999; 87(6): 2341‐7
- Schulze M B , Hu F B. Primary prevention of diabetes: what can be done and how much can be prevented?nAnnu Rev Public Health 2005; 26: 445‐67
- Jentjens R L, Venables M C , Jeukendrup A E. Oxidation of exogenous glucose, sucrose, and maltose duringnprolonged cycling exercise. J Appl Physiol 2004; 96(4): 1285‐91
- Jentjens R L, Moseley L, Waring R H, et al. Oxidation of combined ingestion of glucose and fructose duringnexercise. J Appl Physiol 2004; 96(4): 1277‐84
- Jeukendrup A E. Modulation of carbohydrate and fat utilization by diet, exercise and environment. BiochemnSoc Trans 2003; 31(Pt 6): 1270‐3
- Green H J, Duhamel T A, Ferth S, et al. Reversal of muscle fatigue during 16 h of heavy intermittent cyclenexercise. J Appl Physiol 2004; 97(6): 2166‐75
- Carter S L, Rennie C , Tarnopolsky M A. Substrate utilization during endurance exercise in men and womennafter endurance training. Am J Physiol Endocrinol Metab 2001; 280(6): E898‐907
- Jacobson T L, Febbraio M A, Arkinstall M J, et al. Effect of caffeine co‐ingested with carbohydrate or fat onnmetabolism and performance in endurance‐trained men. Exp Physiol 2001; 86(1): 137‐44
- Hawley J A, Burke L M, Angus D J, et al. Effect of altering substrate availability on metabolism andnperformance during intense exercise. Br J Nutr 2000; 84(6): 829‐38
- Fallon K E, Broad E, Thompson M W, et al. Nutritional and fluid intake in a 100‐km ultramarathon. Int JnSport Nutr 1998; 8(1): 24‐35
- Thompson F E, Midthune D, Subar A F, et al. Performance of a short tool to assess dietary intakes of fruitsnand vegetables, percentage energy from fat and fibre. Public Health Nutr 2004; 7(8): 1097‐105
- Stern A H. A review of the studies of the cardiovascular health effects of methylmercury with considerationnof their suitability for risk assessment. Environ Res 2005; 98(1): 133‐42
- Harris W S. Are omega‐3 fatty acids the most important nutritional modulators of coronary heart diseasenrisk? Curr Atheroscler Rep 2004; 6(6): 447‐52
- Andersen L L, Tufekovic G, Zebis M K, et al. The effect of resistance training combined with timed ingestionnof protein on muscle fiber size and muscle strength. Metabolism 2005; 54(2): 151‐6
- Barr S I , Rideout C A. Nutritional considerations for vegetarian athletes. Nutrition 2004; 20(7‐8): 696‐703
- Burke L M. Energy needs of athletes. Can J Appl Physiol 2001; 26 Suppl: S202‐19
- Phillips S M. Protein requirements and supplementation in strength sports. Nutrition 2004; 20(7‐8): 689‐95
- Singh M. Role of micronutrients for physical growth and mental development. Indian J Pediatr 2004; 71(1):n59‐62
- Gleeson M , Bishop N C. Elite athlete immunology: importance of nutrition. Int J Sports Med 2000; 21 Suppln1: S44‐50
- Ajose O A, Adelekan D A , Ajewole E O. Vitamin A status of pregnant Nigerian women: relationship to dietarynhabits and morbidity. Nutr Health 2004; 17(4): 325‐33
- Youngkin E Q , Thomas D J. Vitamins: common supplements and therapy. Nurse Pract 1999; 24(11): 50, 53,n57‐60 passim; quiz 68‐9
- Chen J, Wanming D, Zhang D, et al. Water‐soluble antioxidants improve the antioxidant and anticancernactivity of low concentrations of curcumin in human leukemia cells. Pharmazie 2005; 60(1): 57‐61
- Shafat A, Butler P, Jensen R L, et al. Effects of dietary supplementation with vitamins C and E on musclenfunction during and after eccentric contractions in humans. Eur J Appl Physiol 2004; 93(1‐2): 196‐202
- Yannakoulia M, Keramopoulos A , Matalas A L. Bone mineral density in young active females: the case ofndancers. Int J Sport Nutr Exerc Metab 2004; 14(3): 285‐97
- Saito N, Tabata N, Saito S, et al. Bone mineral density, serum albumin and serum magnesium. J Am Coll Nutr 2004; 23(6): 701S‐3S
- Parsons L C. Osteoporosis: incidence, prevention, and treatment of the silent killer. Nurs Clin North Amn2005; 40(1): 119‐33
- McKevith B. The nation's diet: promoting healthy eating. Nurs Stand 2004; 18(48): 45‐52; quiz 54
- Lukaski H C. Magnesium, zinc, and chromium nutriture and physical activity. Am J Clin Nutr 2000; 72(2nSuppl): 585S‐93S
- Lukaski H C. Vitamin and mineral status: effects on physical performance. Nutrition 2004; 20(7‐8): 632‐44
- Rehrer N J. The maintenance of fluid balance during exercise. Int J Sports Med 1994; 15(3): 122‐5
- Maughan R , Shirreffs S. Exercise in the heat: challenges and opportunities. J Sports Sci 2004; 22(10): 917‐n27

