Srinivas Pentyala1,2,3,4*, Aleef Rahman1, Pooja Mysore1, Thomas Tumillo1, Avijit Roy1, Sahana Pentyala1, John Muller1, Krupali Chokshi and Sardar Khan2
Departments of Anesthesiology, School of Medicine and School of Health Technology Management, Stony Brook University, Stony Brook, New York, USA
Departments of Urology, School of Medicine and School of Health Technology Management, Stony Brook University, Stony Brook, New York, USA
Departments of Health Sciences, School of Medicine and School of Health Technology Management, Stony Brook University, Stony Brook, New York, USA
Departments of Physiology & Biophysics, School of Medicine and School of Health Technology Management, Stony Brook University, Stony Brook, New York, USA
Corresponding Author:
Sinivas Pentyala
Departments of Anesthesiology
School of Medicine and School of Health Technology Management
Stony Brook University, Stony Brook, New York, USA
Tel: 6314442974
E-mail: srinivas.pentyala@stonybrook.edu
Keywords
Bone mass density, lactation, nutrition, osteoporosis, pregnancy
Introduction
Although osteoporosis is considered a rare complication of pregnancy and lactation, it ranks among the three most common diseases affecting women in the United States, besides breast cancer and cardiovascular disease [1-3]. This disease affects approximately ten percent of the female population. Around 500,000 vertebral fractures [4] and 247,000 hip fractures [5] are reported annually. Hip fracture is considered the most serious osteoporosis-associated complication. Health care costs to treat this complication range from seven to ten billion US dollars annually [6]. This review focuses on the prevalence of osteoporosis associated with pregnancy, which occurs in pregnant women in the last trimester or shortly after delivery [7-9].
Anatomy and Physiology
The skeletal system, which consists of 206 bones, supports and maintains the framework of the body, aids in body movement, protects vital internal organs, acts as a mineral reservoir [10,11] and houses the bone marrow. Bone is a dynamic structure, composed of an organic framework embedded in an inorganic salt [10]. This organic framework is 80% cortical (compact) bone that provides rigidity and tensility and 20% trabecular (cancellous) bone that provide strength and elasticity [10-13].
The period of bone growth involves a continuous coupling process of bone resorption and formation, also known as the bone remodeling process [11,13-15]. Bone remodeling is a process initiated by the osteoclasts whose activity is regulated by several factors like PTH, glucocorticoids, vitamin D, sex steroids, insulin, prostaglandin and growth factors [16-21]. Cytokines, growth substances, hormones, prostaglandins and nitric oxide also affect the bone remodeling cycle [22,23]. Endothelial cells are also reported to be involved in the bone’s complex communication network with osteoblasts, osteoclasts, macrophages, stromal cells, and other cells present within the bone tissue [24].
Osteoblasts secrete osteoid, a bone matrix protein [11,13,16] and osteogenin [25], which initiate and promote osteogenesis. The newly formed matrix mineralizes in a span of 3 months, completing the bone formation process [11]. Through this process, people achieve maximum bone mass at the age of thirty-five [1]. After reaching maximum bone mass [5], the bone remodeling process becomes uncoupled, possibly due to impaired osteoblast function. Thus, especially for women who begin menopause, the rate of bone formation remains constant, but the rate of bone resorption increases due to the bone’s increasing sensitivity to PTH [1]. This uncoupling process Results in a net loss of bone mass density (BMD), which may lead to osteoporosis [4,15,23,24]. This pattern of bone loss is not uniform throughout the skeleton [4,25- 29], but most commonly occurs at the vertebrae, proximal femur, and distal radius, which are highly trabecular in nature [4,27,29].
Pathogenesis
There are three types of diseases associated with bone. (A) Osteopenia is decrease in bone calcification or bone density. (B) Osteomalacia is a disease of adults that is characterized by softening of the bones. (C) Osteoporosis is a metabolic bone disease that reduces BMD, without any reorganization in its chemical composition, resulting in a high potentiality of bone fracture [1,30].
The two types of age-related osteoporosis are the postmenopausal (type I) and the senile (type II) osteoporosis [1,4,31,32]. Type I affects people within the ages of 51 to 75 years during the period of menopause. It is recognized as accelerated trabecular bone loss due to an insufficient level of estrogen present in the body. This increases the bone resorption rate leading to fractures of the vertebrae, distal radius and hip. Type II affects elderly people exceeding the age of 70 years with fractures of the hip and vertebrae [1,4,25,26,33]. Type II is characterized by nonaccelerated trabecular and cortical bone loss related to an insufficient level of vitamin D [1,4].Estrogen deficiency is the most dominant factor in the pathogenesis of this disorder [34].
Osteoporosis induced softening of the bones usually occurs at the femoral necks, lumbar spine and other sites during the second or third trimester of pregnancy. The loss of BMD increases the possibility of bone fractures, which may seriously injure either the mother or child. Physiological adaptation to pregnancy under the control of complex hormonal regulating mechanisms prevents excessive resorption of calcium by the women’s skeleton [35-37]. Thus the increase in maternal blood calcium in turn meets the demands of fetal requirement for calcium. Calcium deficiency may not be the only cause of transient osteoporosis. Several authors reported temporary failure of calcitrophic hormones and decreased activities of osteoblasts as other causes. Calcitrophic hormones and osteoblasts help the maternal skeleton adapt to the stress of childbirth [38,39]. Calcium homeostasis is affected by tocolytic therapy with magnesium sulfate [40,41]. Bone mass density declined in patients that were exposed to magnesium sulfate during the first to eleventh week postpartum [42]. Mothers with preeclampsia have reported paradoxical bone mineralization in twin-to-twin transfusion syndrome. Bone mineral content is reported to be higher in the osteopenic and polcythemic child than in the anemic and osteoporotic child [43]. However, by three months of age, the mineral homeostasis and biochemical levels return to normal [44].
PTH-related peptide (PTHrP) was recently identified as one possible factor that may contribute to the pathogenesis of pregnancy-associated osteoporosis [45]. PTHrP is produced during lactation [46] and is present in high concentrations in milk [47]. PTHrP concentrations are elevated during pregnancy, presumably contributing to a state of maternal hyperparathyroidism (Table 1).
| (1) |
Increase bone resorption of the maternal skeleton |
| (2) |
Regulating cellular proliferation and differentiation |
| (3) |
Development of the fetal cartilage and bone skeleton |
| (4) |
Relaxing the vascular and nonvascular smooth muscle |
| (5) |
Maintenance of reproduction system |
| (5) |
Maternal-fetal calcium transfer |
| (6) |
Parturition |
| (7) |
Embryogenesis |
| (8) |
Milk production |
Table 1: Functions of parathyroid hormone-related peptide.
Osteoporosis could also occur with high doses of methotiexate and oral coagulants [48-50], through chronic estrogen deficiency associated with hypogonadotrophic hypgonadism, and through magnesium deficiency, which can be caused by chronic alcoholism [51,52]. Osteoporosis is associated with patients requiring large dosages of heparin [53,54]. Women, who have a history of thromboembolism, receive prophylactic antithrombotic therapy with heparin during pregnancy [55,56]. Heparin reduces BMD, causing osteoporosis or osteopenia [57,58,54-60]. Though it has been reported that, use of low-molecular-weight heparin instead of regular heparin, may avoid maternal osteoporosis [59]; further investigation is needed in this area. Ringe and Keller reported that the use of ossein-hydroxyapatite-compound (OHC), in conjunction with heparin, causes no significant change in bone mass [60].
Etiology
Hormonal, mechanical, and dietary factors are crucial to the maintenance of the skeleton, regulation of the bone remodeling process, and skeletal growth [26, 61,62]. Other supplementary factors involved in the development of osteoporosis are classified into demographic and genetic, reproductive status and history, dietary, environmental, behavioral, disease states, and drug therapeutic categories. The degree of osteoporosis varies in ethnic backgrounds due to differences in maximum bone mass, physical characteristics, and family history. West Indians and blacks have a lower frequency of osteoporosis than white Americans, northwestern Europeans and Asians [16] Insufficient sunlight exposure and anorexia nervosa, which could be causes of vitamin D deficiency and malnutrition, may lead to osteoporosis [63,64]. Geographic area may also play an important role in the occurrence of this syndrome [6, 65].
Various lifestyles can also lead to osteoporosis. Sustained immobilization or a sedentary life-style may cause osteoporosis, by decreasing the activity of the osteoblasts resulting in an uncoupled bone remodeling process [6,10,26,66-68]. Environmental conditions like space flight may also affect the growth of the skeleton [69]. Astronauts experience loss of BMD in bones that carry weight and pressure under normal gravity [70]. Bone loss occurs in bones that carry weight under life-styles involving cigarette smoking, excessive alcohol consumption, and coffee drinking which inhibits the activity of the osteoblasts [5,25,26,68,71-73]. The development of osteoporosis may also be related to various medical conditions [74-78], diseases and pharmacological agents [4-6,79-85]. Breuil et.al., reported the first case of insufficient fracture of the sacrum revealing a pregnancy-associated osteoporosis. Medical conditions like hyperthyroidism, hyperparathyroidism, paralysis, chronic obstructive lung disease, intestinal malabsorption, renal dysfunction, malignancy, diabetes mellitus, pregnancy, and rheumatoid arthritis may cause osteoporosis. Pharmacological agents like corticosteroids, thyroid hormone, anticonvulsant, antacids containing aluminum, heparin, cancer chemotherapy, tetracycline, isoniazid and immunosuppressive agents, may lead to the development of osteoporosis (Figure 1).
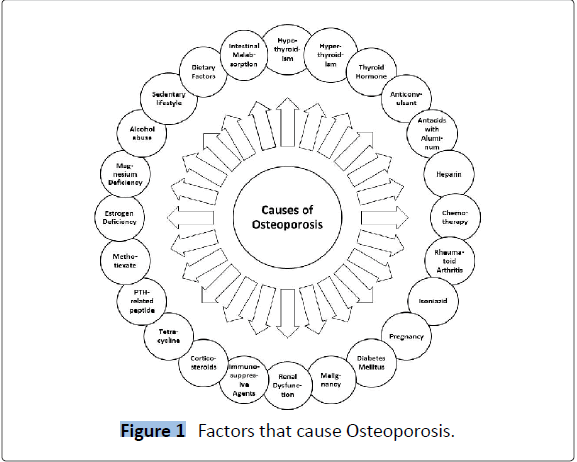
Figure 1: Factors that cause Osteoporosis.
Female Athletes in particular, have a tendency to develop osteoporosis, since they are under a lot of pressure to maintain a low percentage of body fat to achieve peak performance. Female athlete triad, which consists of disordered eating, amenorrhea, and osteoporosis becomes a common clinical entity amongst female athletes [86-91]. In addition, female athletes have decreased levels of sex hormones, together with other hormonal imbalances, such as sex steroid metabolism and menstrual irregularities, which lead to physiologic changes that result in bone loss [92-95].
Symptoms
Transient osteoporosis, also known as idiopathic osteoporosis, primarily affects the femoral neck of the hip and sometimes the lumbar spine and ribs [63,96,97]. Patients usually complain of a sudden onset of sharp pain following fracture or chronic backache [26]. Pain is generally felt in the periarticular, groin, buttock, upper anterior thigh, or hip pain during pregnancy [97-103]. However, pain in the hips can be mistaken for lower abdominal soreness [104,105]. Gunnar and Lindholm [100] stated four features that would represent a case of transient osteoporosis: “(a) Progressive hip pain that accentuates by weight bearing and develops shortly before or in the last trimester of pregnancy, (b) roentgenograms showing reduction of radiodensity of the femoral head and at times of the femoral neck and acetabulum, (c) excellent prognosis, thus pain subsides and the roentgenographic appearance returns to normal within several months after delivery and (d) negative laboratory findings.”
Diagnosis
Diagnosing osteoporosis during pregnancy is a challenging problem to the clinician as many of the available diagnostic procedures are recommended not to be performed on pregnant women. Osteoporosis patients are often recognized accidentally on X-rays taken for other purposes, such as fractures. On X-rays, radiolucency may indicate osteoporosis [13,27] of the appendicular skeleton, showing cortical thinning and the loss of trabecular bone, especially in the femoral neck. About thirty percent of the bone mineral content must be lost in order for it to appear on standard x-rays [13,104-106]. Vertebral fractures can be detected through x-rays, but radiographs are not an accurate method of detecting this syndrome Table 2.
| Type of trace elements |
Functions of trace elements |
| Aluminum |
Inhibits osteoblasts causing hindering bone formation |
| Copper |
Suppresses the functions of osteoclasts and osteoblasts, lowering bone turnover |
| Flouride |
Increases bone mass by storing in new sites of bone formation |
| Gallium |
Suppresses bone turnover in humoralhypercalcemia of malignancy |
| Iodine |
Increases bone turnover when forming thyroxine and triiodothyronine |
| Magnesium |
Stimulates osteoclastic cells to enhance bone turnover |
| Zinc |
Influences bone turnover by secretion of calcitonin from the thyroid gland |
Table 2: Trace elements involved in skeletal growth and development
Osteoporosis may be determined by examining one’s BMD [6,107] by invasive or noninvasive procedures; invasive procedures include a bone biopsy taken from the iliac crest [6,70], which is the most accurate technique to identify osteoporosis [6]. A histomorphometry determines the degree of bone mineralization, the quantity and structure of the trabecular bone, the number of active bone cells, and the rates of bone formation and resorption. Noninvasive techniques include plain radiographs [6,13,70,77,106], radiogrammetry [6,106], single photon absorptiometry [70,106], dual photon absorptiometry [6,77,106], computed tomography [6,77,108-111], quantitative digital radiography [112], nuclear scanning of total body calcium and retention of Tc-labeled pyrophosphate. Without causing discomfort, these techniques provide accurate measurements of BMD. Reid et al. reported that total body fat is the best indicator of BMD in the skeleton [113].
Bone densitometry is the safest and easiest way of diagnosing existing osteoporosis [114]. Techniques used to diagnose low BMD are [1] the Quantitative Computed Tomography (QCT) of the spine, which images the vertebrae using low-dosage radiation and measures the mineral content [4] and the X-ray Absorptiometry (DXA) which images the spine and hip [115].
Lactation and Osteoporosis
Breast-feeding for three months in the United States is common with significant bone loss [63,102,116] followed by complete recovery of the cancellous bone, six months postpartum [56,63]. During this time, loss of BMD is reported to occur in the appendicular skeleton, particularly the trabecular bone [117]. Studies investigating longer periods of lactation have yielded different conclusions; they include lower bone mineral content at the lumbar spine [60,63],or radius [32,63] or no reduction in bone mass [52,63,96]. Lactation brings about physiological changes, which includes an increase in bone resorption and a rise in prolactin levels. Longitudinal studies revealed that periods of lactation greater than six months leads to significant bone loss at the lumbar spine (5.1%) [63,116], femoral neck (4.8%) [63,116], and distal forearm (7.0%) [46,63]. Nursing periods exceeding nine months have been associated with a significantly greater deficit in bone mass at one year as compared to women who nursed for only six to nine months [63,116]. Despite these documented bone losses, radial BMD seems to return to normal by as early as four months post weaning [46,63].
Osteoporosis has been shown to occur without the influence of lactation [40], but continuous lactation after the onset can further promote resorption [117,118]. In a nine-month time span, 400 mg/day of calcium is provided for the infant during lactation, which is four times greater than the amount of calcium lost in pregnancy [40].
Treatment
Once osteoporosis is diagnosed, appropriate treatments should be instituted immediately to control its development (Figure 2). Treatments include calcium supplementation, salmon calcitonin, estrogen, vitamin D, anabolic steroids, diphosphonates, fluoride, and coherence therapy. The use of calcium supplementation has positive effects towards achieving peak bone mass. Salmon calcitonin is used to prevent postmenopausal osteoporosis and to treat progressing osteoporosis [119]. Treatment with estrogen elevates the calcium balance and reduces bone loss. Estrogen Replacement Therapy (ERT) reduces the rate of bone turnover and inhibits bone resorption [116]. Other inhibitors of bone resorption are biophosphonates, which are consumed by the skeleton. Biophosphonates also increase bone formation and bone mineral content. Biophosphonates include etidronate and alendronate sodium [1, 120]. Stimulators of bone formation include sodium fluoride, calcitriol, PTH, growth hormone, growth factors (IGFs and TGF-beta), prostaglandin (PGE2), strontium salts and anabolic steroids [1]. Though reported to be effective agents, none of the above-mentioned factors have been extensively studied, except for sodium fluoride. Magnesium therapy was reported to prevent fracture and increase bone mass density in patients with osteoporosis [46,121]. Some of the treatment modalities interfere with the normal development of the fetus and maintenance of pregnancy and hence the physicians should use extreme caution in the treatment aspect Table 3.
| |
Osteoporosis of the Hip during Pregnancy (OHP) |
Pregnancy Spinal Osteoporosis (PSO) |
| Effects |
Bone mass density loss in the hips, spine and ribs; may lead to possible hip fractures |
Bone mass density loss in the axial skeleton: the lumbar spine and proximal femur |
| Time of Onset |
Late second or third trimester during pregnancy |
Appears within three months after delivery of the first child |
| Symptoms |
Pain to the periarticular, groin, buttock upper anterior thigh, and hips |
Back pain, loss of height, and vertebral compression fracture |
| Diagnosis |
Serum and urine content, radiogammetry, radiographs, single and dual absorptiometry, quantitative computed tomography and nuclear scanning |
X-rays, serum and urine content, radiogammetry, radiographs, single and dual absorptiometry, quantitative computed tomography and nuclear scanning |
| Etiology |
Deficiency of 1,25 (OH) 2D3, elevated levels of PTHrP, local ischemia, failure of calcitrophic hormones, high dosages of methotiexate and oral coagulants, deficiency of estrogen, deficiency of calcium and magnesium, impaired venous flow, heparin therapy Magnesium sulfate and tocolytic agents |
Cytokines: interleukin I (IL-I) Elevated levels of PTHrP |
| Treatment |
Supplementation of calcium, estrogen, vitamin D, anabolic steroids, fluoride, diphosphonates, corticosteroids, calcitonin, Biophosphonates. |
|
Table 3: Differences between two types of osteoporosis associated with pregnancy
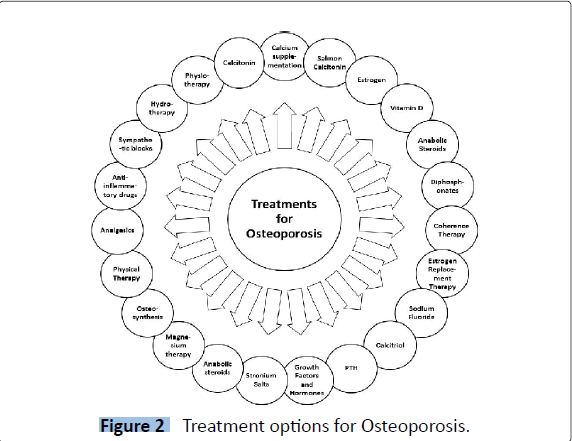
Figure 2: Treatment options for Osteoporosis.
Osteosynthesis consists of repairing fractures by internal fixation with a mechanical device. In rare cases, osteosynthesis is used to help patients recover from bone fractures of the femoral neck, and from osteoporosis in pregnancy [99,122]. Fractures of the femoral neck are diagnosed a few days before birth [123-125]. Hence, osteosynthesis is performed during the post-partum period to reduce the risk of injury to the mother and infant [99].
Goldman et al. advised bed rest as the appropriate treatment for most cases without the need of any specific therapy [119]. Other therapies for transient osteoporosis include proper positioning of the patient, physical therapy to increase strength, analgesics, nonsteroidal anti-inflammatory drugs, oral or interarticular corticosteriods, sympathetic blocks, hydrotherapy, traction, physiotherapy and calcitonin to reduce bone resorption [100,101,126-131]. Remaining physically active, enhancing one’s balance and coordination, and increasing muscular strength may reduce the occurrence of osteoporosis [132-134].
Discussion
During pregnancy and lactation, the fetus’ physiological requirement of calcium burdens the maternal’s calcium reservoir of the skeleton. The RDA intake of calcium for women is 1,200 mgs per day during these periods. During the third trimester, approximately thirty grams of calcium are needed for the fetal skeletal growth [135]. The National Institutes of Health Consensus reported that if the recommended levels of dietary calcium are met, there would be no loss in the mother’s calcium level [135]. During lactation, women lose 160-300 mg of calcium per day in order to meet the infant’s requirement for growth. Many women do not have enough calcium in their diet and are undernourished. A deficiency of calcium propagates the mother’s body to search for another source of calcium; one source is the maternal’s skeleton. Losing the BMD in the mother’s skeleton is recognized as osteoporosis associated with pregnancy.
Bones are largely composed of calcium [40]; more calcium is required during pregnancy and lactation because of “extra-cellular fluid volume expansion, increased renal filtration, placental transport to calcify the fetal bones and possibly, an increase in the maternal mass for the calcium demands of lactation” [40]. During the first trimester, the amount of calcium needed by the fetus is 2 to 3 mgs but increases to 250 mgs during the last trimester for skeletal growth. Deficiency of calcium causes the loss of BMD of the maternal’s skeleton, through resorption, [98,136,137] leading to osteoporosis [58].
Despite the growing number of people suffering from osteoporosis or related fractures and the enormous financial support spent in managing osteoporosis, prevention of this disease has become the leading concern of health care systems worldwide. The health care systems are trying to detect the disease early to prevent further damaging. They are also limiting the number of disabilities, by providing rehabilitation [78] and moderate weightbearing exercise programs, [68,118] for patients who are at a high risk or suffer from osteoporosis. The best way to prevent this syndrome is to increase awareness, to make a precise diagnosis, and to institute prompt treatments and avoid invasive studies.
6490
References
- Chung PH, Maroulis GB (1996) Osteoporosis- An Update on Prevention and Treatment. The Female Patient 2:39-50.
- Liel Y, Atar D, Ohana N (1998) Pregnancy-associated osteoporosis: preliminary densitometric evidence of extremely rapid recovery of bone mineral density. South Med J 91: 33-35.
- Dunne F, Walters B, Marshall T, Heath DA (1993) Pregnancy associated osteoporosis. Clin Endocrinol (Oxf) 39: 487-490.
- Riggs BL, Melton LJ 3rd (1986) Involutional osteoporosis. N Engl J Med 314: 1676-1686.
- Kelsey JL, Hoffman S (1987) Risk factors for hip fracture. N Engl J Med 316: 404-406.
- (1987) Bone mineral densitometry. Health and Public Policy Committee, American College of Physicians. Ann Intern Med 107: 932-936.
- Khovidhunkit W, Epstein S (1996) Osteoporosis in pregnancy. Osteoporos Int 6: 345-354.
- Smith R, Ostlere S, Athanasou N, Vipond S (1996) Pregnancy-associated osteoporosis. Lancet 348: 402-403.
- Rizzoli R, Bonjour JP (1996) Pregnancy-associated osteoporosis. Lancet 347: 1274-1276.
- Spence AP (1990) The Skeletal System. (3rd edtn), The Benjamin/Cummings Publishing Co, New York, USA.
- Arnaud CD (1985) Mineral and bone homeostasis. WB Saunders Co, Philadelphia, USA.
- Ganong WF (1985) Review of Medical Physiology. Lange medical Publications, Los Altos, California, USA.
- Silverberg SJ, Lindsay R (1987) Postmenopausal osteoporosis. Med Clin North Am 71: 41-57.
- Frost HM (1979) Treatment of osteoporoses by manipulation of coherent bone cell populations. Clin Orthop Relat Res : 227-244.
- Eriksen EF (1986) Normal and pathological remodeling of human trabecular bone: Three-dimensional reconstruction of the remodeling sequence in normals and in metabolic bone disease. Endocr Rev 7:379-408.
- Riis BJ (1996) The role of bone turnover in the pathophysiology of osteoporosis. Br J Obstet Gynaecol 103 Suppl 13: 9-14.
- Teitelbaum SL (1993) Bone remodeling and the osteoclast. J Bone Miner Res 8 Suppl 2: S523-525.
- Weryha G, Leclère J (1995) Paracrine regulation of bone remodeling. Horm Res 43: 69-75.
- Titus L, Jackson E, Nanes MS, Rubin JE, Catherwood BD (1991) 1,25-Dihydroxyvitamin D reduces parathyroid hormone receptor number in ROS 17/2.8 and prevents glucocorticoid-induced increase in these receptors: Relationship to adenylate cyclase activation. Journal of Bone & Mineral Research 6:631-637.
- Matsumoto T, Yamato H, Okazaki R, Kumegawa M, Ogata E (1992) Effect of 24,25-dihydroxyvitamin D3 in osteoclasts. Proc Soc Exp Biol Med 200: 161-164.
- Kimmel DB (1993) A paradigm for skeletal strength homeostasis. J Bone Miner Res 8 Suppl 2: S515-522.
- Raisz LG (1993) Bone cell biology: new approaches and unanswered questions. J Bone Miner Res 8 Suppl 2: S457-465.
- Collin-Osdoby P, Nickols GA, Osdoby P (1995) Bone cell function, regulation, and communication: a role for nitric oxide. J Cell Biochem 57: 399-408.
- Ripamonti U, Ma S, Cunningham NS, Yeates L, Reddi AH (1992) Initiation of bone regeneration in adult baboons by osteogenin, a bone morphogenetic protein. Matrix 12: 369-380.
- Ivey JL, Baylink DJ (1981) Postmenopausal osteoporosis: proposed roles of defective coupling and estrogen deficiency. Metab Bone Dis Relat Res 3: 3-7.
- Nordin BE, Need AG, Morris HA, Horowitz M (1985) New approaches to the problems of osteoporosis. Clin Orthop Relat Res : 181-197.
- Riggs BL (1985) Osteoporosis. (17th edtn). WB Saunders Co, Philadelphia, USA.
- Aurbach GD, Marx SJ, Spiegel AM (1985) Metabolic bone disease. WB Saunders Co, Philadelphia, USA.
- Delany AM, Dong Y, Canalis E (1994) Mechanisms of glucocorticoid action in bone cells. J Cell Biochem 56: 295-302.
- Krane SM, Holick MF (1987) Metabolic bone disease. (11th edtn), McGraw-Hill Book Co, New York, USA.
- Teotia M, Teotia SP, Singh RK (1979) Idiopathic juvenile osteoporosis. Am J Dis Child 133: 894-900.
- Scileppi KP (1983) Bone and joint disease in the elderly. Med Clin North Am 67: 517-530.
- Parfitt AM (1987) Trabecular bone architecture in the pathogenesis and prevention of fracture. Am J Med 82: 68-72.
- Anderson HC (1995) Molecular biology of matrix vesicles. Clin Orthop Relat Res : 266-280.
- Anai T, Tomiyasu T, Arima K, Miyakawa I (1999) Pregnancy-associated osteoporosis with elevated levels of circulating parathyroid hormone-related protein: a report of two cases. J Obstet Gynaecol Res 25: 63-67.
- Dunne F, Walters B, Marshall T, Heath DA (1993) Pregnancy associated osteoporosis. Clin Endocrinol (Oxf) 39: 487-490.
- Khastgir G, Studd J (1994) Pregnancy-associated osteoporosis. Br J Obstet Gynaecol 101: 836-838.
- Rillo OL, Di Stefano CA, Bermudez J, Maldonado Cocco JA (1994) Idiopathic osteoporosis during pregnancy. Clin Rheumatol 13: 299-304.
- Cruikshank DP, Pitkin RM, Donnelly E, Reynolds WA (1981) Urinary magnesium, calcium, and phosphate excretion during magnesium sulfate infusion. Obstet Gynecol 58: 430-434.
- Cholt M, Spatenka J, Slezák Z (1984) [Radiographic study of acute venous thrombosis of the lower extremities. Multilevel skiascopically monitored phlebography]. Cesk Radiol 38: 2-13.
- Shenolikar IS (1970) Absorption of dietary calcium in pregnancy. Am J Clin Nutr 23: 63-67.
- Pitkin RM, Reynolds WA, Williams GA, Hargis GK (1979) Calcium metabolism in normal pregnancy: a longitudinal study. Am J Obstet Gynecol 133: 781-790.
- Mazanec DJ, Grisanti JM (1989) Drug-induced osteoporosis. Cleve Clin J Med 56: 297-303.
- Ginsberg JS, Hirsh J (1989) Anticoagulants during pregnancy. Annu Rev Med 40: 79-86.
- Griffiths HT, Liu DT (1984) Severe heparin osteoporosis in pregnancy. Postgrad Med J 60: 424-425.
- Abbott L, Nadler J, Rude RK (1994) Magnesium deficiency in alcoholism: possible contribution to osteoporosis and cardiovascular disease in alcoholics. Alcoholism, Clinical & Experimental Research 18:1076-1082.
- Sojka JE, Weaver CM (1995) Magnesium supplementation and osteoporosis. Nutr Rev 53: 71-74.
- Reid IR, Ames R, Evans MC, Sharpe S, Gamble G, et al. (1992) Determinants of total body and regional bone mineral density in normal postmenopausal women--a key role for fat mass. J Clin Endocrinol Metab 75: 45-51.
- Thiede MA, Rodan GA (1988) Expression of a calcium-mobilizing parathyroid hormone-like peptide in lactating mammary tissue. Science 242: 278-280.
- Budayr AA, Halloran BP, King JC, Diep D, Nissenson RA, et al. (1989) High levels of a parathyroid hormone-like protein in milk. Proc Natl Acad Sci U S A 86: 7183-7185.
- Siragusa S, Cosmi B, Piovella F, Hirsh J, Ginsberg JS (1996) Low-molecular-weight heparins and unfractionated heparin in the treatment of patients with acute venous thromboembolism: Results of a meta-analysis. Am J Med 100: 269-277.
- Ginsberg JS, Hirsh J (1992) Use of antithrombotic agents during pregnancy. Chest 102: 385S-390S.
- Niebyl JR (1991) Drug therapy during pregnancy. Curr Opin Obstet Gynecol 3: 24-27.
- Wunderer G, Müller G (1990) [Osteoporosis and pre- and postpartal heparin therapy]. Geburtshilfe Frauenheilkd 50: 61-63.
- deSwiet M (1985) Antihypertensive drugs in pregnancy. Br Med J (Clin Res Ed) 291: 365-366.
- Dahlman T, Lindvall N, Hellgren M (1990) Osteopenia in pregnancy during long-term heparin treatment: a radiological study post partum. Br J Obstet Gynaecol 97: 221-228.
- Dahlman TC (1993) Osteoporotic fractures and the recurrence of thromboembolism during pregnancy and the puerperium in 184 women undergoing thromboprophylaxis with heparin. Am J Obstet Gynecol 168:1265-1270.
- Barbour LA, Kick SD, Steiner JF, LoVerde ME, Heddleston LN, et al. (1994)A prospective study of heparin-induced osteoporosis in pregnancy using bone densitometry. Am J Obstet Gynecol 170:862-869.
- Kohlmeier L, Marcus R (1996) Osteoporosis associated with pregnancy. Academic Press, New York, USA.
- Thompson RC Jr (1973) Heparin osteoporosis. An experimental model using rats. J Bone Joint Surg Am 55: 606-612.
- Starcher BC, Hill CH, Madaras JG (1980) Effect of zinc deficiency on bone collagenase and collagen turnover. J Nutr 110: 2095-2102.
- Melissari E, Parker CJ, Wilson NV, Monte G, Kanthou C, et al. (1992) Use of low molecular weight heparin in pregnancy. Thromb Haemost 68: 652-656.
- Ringe JD, Keller A (1992) [Risk of osteoporosis in long-term heparin therapy of thromboembolic diseases in pregnancy: attempted prevention with ossein-hydroxyapatite]. Geburtshilfe Frauenheilkd 52: 426-429.
- Sandler RB, LaPorte RE (1983) The sparing interaction of bone mass determinants: a hypothesis with implications for osteoporosis. Med Hypotheses 12: 67-75.
- White MK, Martin RB, Yeater RA, Butcher RL, Radin EL (1984) The effects of exercise on the bones of postmenopausal women. Int Orthop 7: 209-214.
- Taguchi Y, Gorai I (1998) [Secondary osteoporosis in gynecology]. Nihon Rinsho 56: 1609-1612.
- Aloia JF, Vaswani AN, Yeh JK, Ross P, Ellis K, et al. (1983) Determinants of bone mass in postmenopausal women. Arch Intern Med 143: 1700-1704.
- Matkovi V, Kostial K, Simonovi I, Buzina R, Brodarec A, et al. (1979) Bone status and fracture rates in two regions of Yugoslavia. Am J Clin Nutr 32: 540-549.
- Seitzer U, Bodo M, Müller PK, Açil Y, Bätge B (1995) Microgravity and hypergravity effects on collagen biosynthesis of human dermal fibroblasts. Cell Tissue Res 282: 513-517.
- Lane JM, Werntz JR, Healey JH, Vigorita VJ (1986) Metabolic bone disease and Paget's disease in the elderly. Part I: Metabolic bone disease. Clin Rheum Dis 12: 49-70.
- Aström J, Ahnqvist S, Beertema J, Jónsson B (1987) Physical activity in women sustaining fracture of the neck of the femur. J Bone Joint Surg Br 69: 381-383.
- Whedon GD (1984) Disuse osteoporosis: Physiological aspects. Calcif Tissue Int 36(Suppl):146-150.
- Haram K, Thordarson H, Hervig T (1993) Calcium homeostasis in pregnancy and lactation. Acta Obstet Gynecol Scand 72: 509-513.
- Hughes-Fulford M, Lewis ML (1996) Effects of microgravity on osteoblast growth activation. Exp Cell Res 224: 103-109.
- Jensen GF (1986) Osteoporosis of the slender smoker revisited by epidemiologic approach. Eur J Clin Invest 16: 239-242.
- Heath H (1983) Progress against osteoporosis. Ann Intern Med 98: 1011-1013.
- Long RG, Meinhard E, Skinner RK, Varghese Z, Wills MR, et al. (1978) Clinical, biochemical, and histological studies of osteomalacia, osteoporosis, and parathyroid function in chronic liver disease. Gut 19: 85-90.
- Adinoff AD, Hollister JR (1983) Steroid-induced fractures and bone loss in patients with asthma. N Engl J Med 309: 265-268.
- Baylink DJ (1983) Glucocorticoid-induced osteoporosis. N Engl J Med 309: 306-308.
- Burckhardt P (1984) Corticosteroids and bone: a review. Horm Res 20: 59-64.
- Need AG, Philcox JC, Hartley TF, Nordin BE (1986) Calcium metabolism and osteoporosis in corticosteroid-treated postmenopausal women. Aust N Z J Med 16: 341-346.
- Spencer H (1982) Osteoporosis: goals of therapy. Hosp Pract (Hosp Ed) 17: 131-138, 143-8.
- Breuil V, Brocq O, Euller-Ziegler L, Grimaud A (1997) Insufficiency fracture of the sacrum revealing a pregnancy associated osteoporosis. First case report. Ann Rheum Dis 56: 278-279.
- Sanborn CF, Horea M, Siemers BJ, Dieringer KI (2000) Disordered eating and the female athlete triad. Clin Sports Med 19: 199-213.
- Gibson JH, Mitchell A, Reeve J, Harries MG (1999) Treatment of reduced bone mineral density in athletic amenorrhea: a pilot study. Osteoporos Int 10: 284-289.
- Anderson JM (1999) The female athlete triad: disordered eating, amenorrhea, and osteoporosis. Conn Med 63: 647-652.
- Manore MM (1999) Nutritional needs of the female athlete. Clin Sports Med 18: 549-563.
- West RV1 (1998) The female athlete. The triad of disordered eating, amenorrhoea and osteoporosis. Sports Med 26: 63-71.
- Timmerman MG (1996) Medical problems of adolescent female athletes. Wis Med J 95: 351-354.
- Rutherford OM (1999) Is there a role for exercise in the prevention of osteoporotic fractures? Br J Sports Med 33: 378-386.
- Ryan AS, Elahi D (1998) Loss of bone mineral density in women athletes during aging. Calcif Tissue Int 63: 287-292.
- De Crée C (1998) Sex steroid metabolism and menstrual irregularities in the exercising female. A review. Sports Med 25: 369-406.
- Bennell KL, Malcolm SA, Wark JD, Brukner PD (1997) Skeletal effects of menstrual disturbances in athletes. Scand J Med Sci Sports 7: 261-273.
- Christiansen C, Rodbro P, Heinild B (1976) Unchanged total body calcium in normal human pregnancy. Acta Obstet Gynecol Scand 55: 141-143.
- Funk JL, Shoback DM, Genant HK (1995) Transient osteoporosis of the hip in pregnancy: natural history of changes in bone mineral density. Clin Endocrinol (Oxf) 43: 373-382.
- Carbone LD, Palmieri GM, Graves SC, Smull K (1995) Osteoporosis of pregnancy: long-term follow-up of patients and their offspring. Obstet Gynecol 86: 664-666.
- Junk S, Ostrowski M, Kokoszczynski L (1996) Transient osteoporosis of the hip in pregnancy complicated by femoral neck fracture: a case report. Acta Orthop Scand 67: 69-70.
- Lose G, Lindholm P (1986) Transient painful osteoporosis of the hip in pregnancy. Int J Gynaecol Obstet 24: 13-16.
- Schapira D1 (1992) Transient osteoporosis of the hip. Semin Arthritis Rheum 22: 98-105.
- Lakhanpal S, Ginsburg WW, Luthra HS, Hunder GG (1987) Transient regional osteoporosis. A study of 56 cases and review of the literature. Ann Intern Med 106: 444-450.
- Zasacki W1 (1993) [Transient osteoporosis of the hip]. Pol Tyg Lek 48 Suppl 3: 43-45.
- Beaulieu JG, Razzano CD, Levine RB (1976) Transient osteoporosis of the hip in pregnancy. Clin Orthop Relat Res : 165-168.
- Vinceneux P, Stevens-Dudragne D, Peckels B, Kaplan G (1979) [Transient osteoporosis of the hip in pregnancy. Report of three cases (author's transl)]. Sem Hop 55: 1701-1704.
- Ayers JW (1985) Hypothalamic osteopenia--body weight and skeletal mass in the premenopausal woman. Clin Obstet Gynecol 28: 670-680.
- Black DM1 (1996) Screening and treatment in the elderly to reduce osteoporotic fracture risk. Br J Obstet Gynaecol 103 Suppl 13: 2-7.
- Genant HK, Cann CE, Ettinger B (1982) Quantitative computed tomography of vertebral spongiosa: A sensitive method for detecting early bone loss after oophorectomy. Ann Intern Med 97:699-705.
- Pogrund H, Bloom RA, Menczel J (1986) Preventing osteoporosis: current practices and problems. Geriatrics 41: 55-6, 64-8, 71.
- Raisz LG, Johannesson A (1984) Pathogenesis, prevention and therapy of osteoporosis. J Med 15: 267-278.
- Hall FM, Davis MA, Baran DT (1987) Bone mineral screening for osteoporosis. N Engl J Med 316: 212-214.
- Sartoris DJ, Resnick D (1988) Digital radiography may spark renewal of bone densitometry. Diag Imaging 145-150.
- Reid IR, Wattie DJ, Evans MC, Budayr AA (1992) Post-pregnancy osteoporosis associated with hypercalcaemia. Clin Endocrinol (Oxf) 37: 298-303.
- Body JJ (1994) [Treatment of osteoporosis: current aspects and perspectives]. Rev Med Brux 15: 282-286.
- Anonymous (1996) Are You at Risk for Osteoporosis? UCSF Osteoporosis Research Group.
- Seibel MJ, Cosman F, Shen V, Gordon S, Dempster DW, et al. (1993) Urinary hydroxypyridinium crosslinks of collagen as markers of bone resorption and estrogen efficacy in postmenopausal osteoporosis. J Bone Miner Res 8:881-889.
- Gruber HE, Gutteridge DH, Baylink DJ (1984) Osteoporosis associated with pregnancy and lactation: bone biopsy and skeletal features in three patients. Metab Bone Dis Relat Res 5: 159-165.
- Smith R, Stevenson JC, Winearls CG, Woods CG, Wordsworth BP (1985) Osteoporosis of pregnancy. Lancet 1: 1178-1180.
- Goldman GA, Friedman S, Hod M, Ovadia J (1994) Idiopathic transient osteoporosis of the hip in pregnancy. Int J Gynaecol Obstet 46: 317-320.
- Harris ST, Watts NB, Jackson RD, Genant HK, Wasnich RD, et al. (1993) Four-year study of intermittent cyclic etidronate treatment of postmenopausal osteoporosis: three years of blinded therapy followed by one year of open therapy. Am J Med 95: 557-567.
- Transient osteoporosis of the hip. A nontraumatic variety of Südeck's atrophy
- Schiano A, Eisinger F, Detolle P, Laponche AM, Brisou B, et al. (1979) [Silicon, bone tissue and immunity]. Rev Rhum Mal Osteoartic 46: 483-486.
- Doury P (1980) Regional osteoporosis of the hip treated with calcitonin--continued. J Rheumatol 7: 114.
- O'Mara RE, Pinals RS (1970) Bone scanning in regional migratory osteoporosis. Case report. Radiology 97: 579-581.
- Scheinberg MA, Aristides RS, Svartman C (1978) Transient regional osteoporosis of the hip treated with calcitonin. J Rheumatol 5: 236-238.
- Doury P, Delahaye RP, Granier R, Pattin S, Metges PJ (1978) Highly localized transient osteoporosis of the knee. Arthritis Rheum 21: 992-993.
- Valenzuela F, Aris H, Jacobelli S (1977) Transient osteoporosis of the hip. J Rheumatol 4: 59-64.
- Drinkwater BL1 (1993) Exercise in the prevention of osteoporosis. Osteoporos Int 3 Suppl 1: 169-171.
- Reginster JY1 (1993) Calcitonin for prevention and treatment of osteoporosis. Am J Med 95: 44S-47S.
- Stendig-Lindberg G, Tepper R, Leichter I (1993) Trabecular bone density in a two year controlled trial of peroral magnesium in osteoporosis. Magnes Res 6: 155-163.
- Fingeroth RJ (1995) Successful operative treatment of a displaced subcapital fracture of the hip in transient osteoporosis in pregnancy. A case report and review of the literature. J Bone Joint Surg Am 77:127-131.
- Gouin F, Maulaz D, Aillet G, Pietu G, Passuti N, et al. (1992) [Fracture of the femoral neck complicating algodystrophy of the hip during pregnancy. Apropos of 2 cases]. Rev Chir Orthop Reparatrice Appar Mot 78: 45-50.
- Brodell JD, Burns JE Jr, Heiple KG (1989) Transient osteoporosis of the hip of pregnancy. Two cases complicated by pathological fracture. J Bone Joint Surg Am 71: 1252-1257.
- Shifrin LZ, Reis ND, Zinman H, Besser MI (1987) Idiopathic transient osteoporosis of the hip. J Bone Joint Surg Br 69: 769-773.
- Caesar RE, Kaplan GW (1994) Incidence of the bell-clapper deformity in an autopsy series. Urology 44: 114-116.
- Rizzoli R, Bonjour JP (1996) Pregnancy-associated osteoporosis. Lancet 347: 1274-1276.
- Kumar R, House R (1983) Idiopathic transient osteoporosis of the hip in pregnancy. Tex Med 79: 33-34.


