Keywords
Outpatient; Health service utilization; Pastoralist
Abbreviations
BSS: Behavioral Surveillance Survey; CHA: Community Health Agent; CI: Confidence Interval; CSA: Central Statistics Agency; DHS: Demographic and Health Survey; FGD: Focus Group Discussion; FMOH: Federal Minister of Health; FP: Family Planning; GTP: Growth and Transformation Plan; HSDP: Health Sector Development Programme; MCH: Maternal and Child Health; MOH: Ministry of Health; NGO: Non-Governmental Organization; OPD: Out Patient Department; OR: Odds Ratio; RHB: Regional Health Bureau; SNNPR: Southern Nations and Nationalities People Region; SOZ: South Omo Zone; STD: Sexually Transmitted Disease; TBA: Traditional Birth Attendant; HH: House Holds
Introduction
In sub-Saharan African, mobile pastoralists are as vulnerable to exclusion from health services as other scattered populations. Pastoralist’ vulnerability is mostly due to factors specific to their way of life and to related everyday constraints, to as well as to their marginality within countries [1]. Pastoralists have had contact to modern medicine for many decades. Health facilities in areas, however, most often lack adequate infrastructure, drugs, quality of care and supervision. Therefore, they may have a weak performance as seen in developing countries in the world [2].
The geographical dispersion of groups and their spatial relationship to each other and to health services interact with other factors linked to every day constraints. Socio-economic and behavioral factors common to rural African settings influence the steps from being concerned about an illness to the decision to seek help as well as to actual utilization of health services. Pastoralists have common cultures and traditions with sedentary communities. Yet, the identification of factors influencing the health service utilization patterns typical for pastoralist remains an additional challenge due to the scarce knowledge of nomad characteristics [2]. Studies demonstrate that females health service utilization lower than men due to men’s discrimination towards women, which is translated into social and economic disparities, causes a special vulnerability of women. Men largely control access to outside practitioners, treatments and knowledge within pastoralist utilization of health services [3]. The studies which were undertaken in Afar Region of Ethiopia showed there is significant difference in modern health utilization between mobile pastoralist and settled communities. Also FMOH health and health related indictors of 2005 confirmed the per capita outpatient visit difference between pastoralists and settled communities [4,5]. Health care utilization/demand literatures show that there is usually lower level of illness reporting and health care utilization in low income countries specially. Health care use is affected by a variety of factors which range from individual attributes to system based factors [6]. The Ethiopian Demographic and health Survey (EDHS) conducted in 2005 showed that 44% of household utilized some type of health service, including treatment sought for sick individuals (31%) and immunization (24%). The findings also revealed that there was high urban to rural difference in outpatient service utilization, which was explained by the fact that the urban population had more access to information. The majority of households (42%) utilized health services from government health center, where as one in two rural household visited government health facilities. About 15% of households that utilized health care did so at private health facilities, with little difference between urban and rural households [7]. The study which was conducted in Chad with 1023 sampled population on mobile camel breeder pastoralists on health service utilization showed that 102(10%) individuals were visited once, 56(5%) twice and 4(0.4%) three times per year [2]. In Ethiopia pastoralists represent about 12% of the total population inhabiting nearly 60% of the country’s geographic area; the outpatient service utilization rate in the pastoralist communities is significantly lower than that of settled communities. According to the Federal Ministry of Health, reports the per capita outpatient attendance rate is reported to be 0.25 at national level, 0.54 at the level of SNNPR but less than 0.09 in one of pastoralist Region [8]. Therefore, this study was carried out to assess outpatient service utilization of pastoralist communities at household level and identify determinants of utilization in pastoralist community, in SNNPR South Omo Zone in Dassanch, Nyangatom and HamarWoredas.
Methods
The study was conducted in three pastoralist Woredas (districts) of South Omo Zone (SOZ), Southwest Ethiopia. A community based cross-sectional study design that employed both qualitative and quantitative data collection methods. The sample size was determined using a single population proportion formula with the following assumptions. Expected outpatient utilization was assumed to be 50%. This is due to lack of similar study in the pastoralist areas and making p=0.5. A 95% confidence interval (data are correct in 95% of cases); A sampling error of 5% (sample values do not deviate from the true population values by more than 5%). Therefore, the calculation was made as follows:
n=Zα/2P [P-1]/d2
=(1.96)2 *(0.46) (0.54)/(0.05)2
=384 individuals
Multiplied by 2 for the design effect
=768
=844 (with addition of potential 10% non-response rate)
For quantitative part, three Woredas (Dassench, Gnagatom and Hamar) were included purposively because of the nature of existing mobile pastoralist communities. Total of 16 kebeles which are six kebeles in both Hamar and Dassenech Woredas each and four kebeles in Gnagatomworeda was included in survey. These kebeles were selected using simple random sampling technique. Samples were allocated proportional to the size of the households in each kebeles. Systematic sampling technique was employed to select households. The list of all household in each kebeles were taken from health extension workers and the first household was selected by lottery method and then every 4th household in the right side of data collectors were included. These samplings of households were achieved because at season of the data collection the community was in their permanent kebeles around Omo River. The mobility of all households in South Omo Pastoralists only twice per year from June to October by basing overflew of Omo River and in the rest season they live around Omo River. The household head or spouse was included to detailed interview and incase when both husband and wife available husband included purposively. The number of households’ was allocated proportional to the size of the households in the Kebeles after simple random selection of Kebeles.
For qualitative part, the participants of FGD were traditional birth attendants, kebeles administrators, clan leaders and elders’ total of 8 members were selected and each Woreda had two Focus Groups. The first Focus Group was containing male and the second Focus Group was female in considering cultural challenge of female get-together with male. The kebeles managers, health extension workers and other local government employee were assisted the selection of discussants in FGD by identifying clan leaders, traditional birth attendants, elders and kebeles administrators.
The data collection was carried out using interviewer administered structured questionnaire. The data collection tools were developed from related literatures and Ethiopian Demographic and Health Survey (EDHS) and then adopted to answer both general and specific objectives of the study. Prior to the actual data collection, the instrument and the guideline was pre-tested on 5% of mobile pastoralists who are live in Salamago Woreda in Mursi tribe in order to check feasibility of the questionnaires. Data was collected through pre-tested interviewer administered structured questionnaires. These questionnaires were containing socio-demographic factors, accessibility, and individual factors which affect outpatient service utilization. The supervisors had closely followed up the data collection processes. Incomplete and inconsistent data was identified and necessary corrections were made in the field. Semi-structured open ended and non-directive focus group discussion (FGD) guide was designed having four sections in order to triangulate response obtained by structured questionnaire which was contained the knowledge of discussant on modern health facilities, factors affecting outpatient service utilization, decision making process within and outside of household to visit health facilities and comparing the costs between modern and traditional services. Six FGDs were conducted with participants from traditional birth attendants, elders, kebele administrator, and clan leaders. The focus group discussions were proposed to clarify subjective issues within the findings of the quantitative part of the study and to benefit from the group interactions in getting further insight on the socio-cultural issues that impose on outpatient service utilization. Each focus group was consisting of eight members that were homogenous in sex but drawn from different villages of the selected Woredas native local clan residents. In each Woredas the female group was include three traditional birth attendants and five elderly ladies, and the male group was included three male elders, two kebele administrators and three clan leaders. The principal investigator had moderated the discussion of the group and data collector was assisted in translating from Amharic to local languages. All FGDs were conducted in a quiet place and selection of the place is based on interest of participant. Each discussion was carefully recorded, not to miss any issues raised during the discussion. In order to get appropriate information, translators who have good knowledge of both Amharic and local langue was selected in each Woreda and two days training was given. The issues had addressed during FGDs were; knowledge about health facilities, factors affecting outpatient service utilization, decision making and comparing the cost of modern health service and traditional treatment.
Frequencies of different variables were computed for description as appropriate. Cross tabulation was done to see the effect of independent variables on the dependent variable which is modern health care service utilization. Binary logistic regression was then carried out to see the association between the significant variables and the dependent variable. Odds ratio with 95% confidence interval was computed to assess the presence and degree of association between dependent and independent variables. For qualitative data the response was transcribed to Amharic and translated to English and the response was categorized in to four themes. The main response from the respondent was reported using narrative sentences. Data on every issue raised was recorded during discussion. In addition, during data collection, note taking and tape-recording was also employed.
Results
Overall 771 participants were involved in the study yielding the response rate 91.3%. Out of the study participants, 605(78.5%) were male, 751(97.4%) were married. Six hundred fifty (86.9%) were illiterate. Seven hundred twenty six (94.2%) were followers of traditional and cultural beliefs. Three hundred and two (39.2%) respondents owned as many as 50 livestock. The medianage was 35 years, 315(40.9%) were 40 years of age and above. Concerning the ethnicity of respondents, threehundred four (39.4%) were Hamar, 178(23.1%) Dassanech and 105(13.6%) Nyangatomrespectively (Table 1).
Table 1 Socio-demographic characteristics of the study participants South Omo Zone Southwest Ethiopia.
| Variable |
Number (n=771) |
Percentage |
| Age in years |
| <20 |
39 |
5.1 |
| 20 – 29 |
176 |
22.8 |
| 30 – 39 |
241 |
31.3 |
| 40 – 49 |
170 |
22 |
| ≥50 |
145 |
18.8 |
| Sex |
| Male |
605 |
78.50% |
| Female |
166 |
21.50% |
| Educational level |
| Illiterate |
670 |
86.9 |
| Primary |
101 |
13.1 |
| Religion |
| Cultural |
726 |
94.2 |
| Protestants |
45 |
5.8 |
| Marital status |
| Married |
751 |
97.4 |
| Divorced/single |
20 |
2.6 |
| Ethnicity |
| Hamar |
304 |
39.4 |
| Dassanech |
178 |
23.1 |
| Nyangatom |
105 |
13.6 |
| Arbore |
60 |
7.8 |
| Murula |
47 |
6.1 |
| Kwego |
39 |
5.1 |
| Kara |
38 |
4.9 |
| Asset |
| No livestock |
77 |
10 |
| 1 to 50 livestock |
302 |
39.2 |
| 51 to 100 livestock |
223 |
28.9 |
| More than 100 livestock |
169 |
21.9 |
A total of 536(69.5%) individuals (414 males and 122 females) reported to have at least one episode of illness within the one year recall period from January 2011 to January 2012. With regard to response to illness episodes, 242(45.1%) selftreated, 217(40.5%) went to traditional healers and only 77(10.0%) used modern health facilities. Among those who used modern facilities, 76(98.7%) went to government health facilities, and only one respondent went to private health facilities (Figure 1).
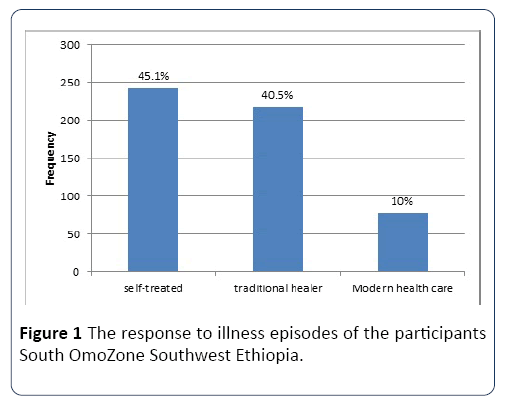
Figure 1: The response to illness episodes of the participants South OmoZone Southwest Ethiopia.
Out of the 217 sick people who went to traditional healers 170(78.3%) were males and 47(21.7%) were females. Sixty two (28.6%) were between the age of 40 to 49 years, 66(30.4%) were above 50. Two hundred nine (96.3%) were married. Only seven (3.2%) had primary education while the rest were illiterate. The majority (61.8%) were from Hamar and Dassanech (Table 2).
Table 2 Socio-demographic characteristics of the people who went to traditional healers South Omo Zone Southwest Ethiopia.
| Variable |
Number (n=217) |
Percentage |
| Age in years |
| <20 |
3 |
1.4 |
| 20-29 |
27 |
12.4 |
| 30 – 39 |
59 |
27.2 |
| 40-49 |
62 |
28.6 |
| ≥50 |
66 |
30.4 |
| Sex |
| Male |
170 |
78.3 |
| Female |
47 |
21.7 |
| Educational level |
| Illiterate |
210 |
96.8 |
| Primary |
7 |
3.2 |
| Religion |
| Cultural |
214 |
98.6 |
| Protestants |
3 |
1.4 |
| Marital status |
| Married |
209 |
96.3 |
| Single or divorced |
8 |
3.7 |
| Ethnicity |
| Hamar |
100 |
46.1 |
| Dassanech |
34 |
15.7 |
| Nyangatom |
32 |
14.7 |
| Murula |
15 |
6.9 |
| Kara |
13 |
6 |
| Kwego |
12 |
5.5 |
| Arbore |
11 |
5.1 |
| Asset |
| No livestock |
25 |
37.3 |
| 1 to 50 livestock |
43 |
31.3 |
| 51 to 100 livestock |
68 |
19.8 |
| More than 100 livestock |
81 |
11.5 |
Those 217 people who went to traditional healers in response to their illness were further asked about the possible factors hindering them from using modern health facilities. One hundred (46.1%) replied that modern health care was somehow not compatible with their cultural beliefs. Long distance was mentioned as a hindering factor by 90(41.5%) responders; service cost of care, unmet expectations and perceived poor quality accounted for 16(7.4%), 8 (3.6%) and 3(1.4%) respectively (Figure 2).
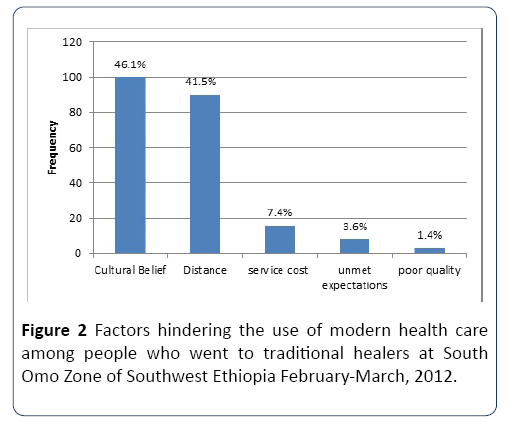
Figure 2: Factors hindering the use of modern health care among people who went to traditional healers at South Omo Zone of Southwest Ethiopia February-March, 2012.
The people who went to traditional healers in response to their illness were also asked about the type of treatment or care they sought from the traditional healers. One hundred eleven (51.2%) of the respondents claimed that they were looking for some forms of herbal medications that are commonly used by people in their locality while 73(33.6%) of the respondents were seeking for massage. The rest claimed that they intended to find a word of advice (13.8%) and cauterization (1.4%). Out of the 242 people who were selftreated, 187(77.3%) were males and 55(22.7%) were females. Most of them (97.1%) were married, 226(93.4%) were uneducated and 232(95.9%) were followers of traditional and cultural beliefs. One hundred (41.3%) were from Dassanech, 55(21.5%) and 35(14.5%) were from Hamar and Nyangatom respectively. Eighty (33.1%) were between 20 to 29 years of age, 38(15.7%) and 16(6.6%) were above 50, and below 20 years of age respectively (Table 3).
Table 3 Socio-demographic characteristics of the people who self-treated their illness South Omo Zone Southwest Ethiopia.
| Variable |
Number(n=242) |
Percentage |
| Age in years |
| <20 |
16 |
6.6 |
| 20 – 29 |
47 |
19.4 |
| 30 – 39 |
80 |
33.1 |
| 40 – 49 |
61 |
25.2 |
| ≥ 50 |
38 |
15.7 |
| Sex |
| Male |
187 |
77.3 |
| Female |
55 |
22.7 |
| Educational level |
| Illiterate |
226 |
93.4 |
| Primary |
16 |
6.6 |
| Religion |
| Cultural |
232 |
95.9 |
| Protestant |
10 |
4.1 |
| Ethnicity |
| Dassanech |
100 |
41.3 |
| Hamar |
52 |
21.5 |
| Nyangatom |
35 |
14.5 |
| Arbore |
22 |
9.1 |
| Murula |
12 |
5 |
| Kara |
11 |
4.5 |
| Kwego |
10 |
4.1 |
| Asset |
| 1 to 50 livestock |
80 |
33.1 |
| 51 to 100 livestock |
75 |
31 |
| >100 livestock |
59 |
24.4 |
| No livestock |
28 |
11.6 |
The major reasons reported by the respondents who selftreated in response to their illness were that they lived very far from the place where modern health facilities are located (35.1%) and that they perceived their illness were not serious (30.2%). Cultural belief, high service cost, unmet expectations, and perceived poor quality of care were mentioned as other factors hindering them from accessing modern health care by 13.6%, 11.2%, 7.4% and 2.5% respectively (Figure 3).
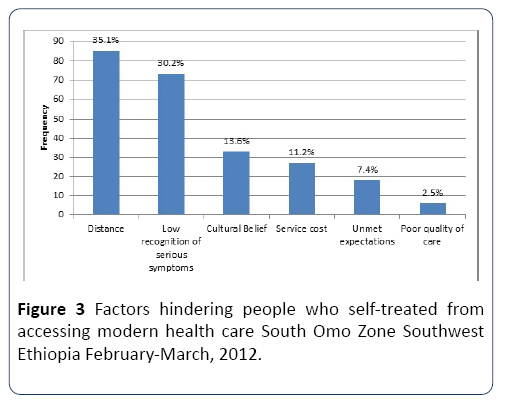
Figure 3: Factors hindering people who self-treated from accessing modern health care South Omo Zone Southwest Ethiopia February-March, 2012.
The most important factors hampering modern health care service utilization of people who self-treated and people who went to traditional healers were mentioned to be long distance of facilities by 175(38.1%) and cultural beliefs by 133(29%) of the non-users of modern health care. Low recognition of serious symptoms, perceived high service cost, unmet expectations, and perceived poor quality of care were mentioned as factors hindering them from accessing modern health care by 73(15.9%), 43(9.3%), 26(5.7%) and 9(2%) of the non-users of modern health care. Out of the 77 respondents who went to modern health facilities for their illness, 55(74%) were males and 22(26%) were females. Twenty eight (36.4%) were between the ages of 30 and 39 and 15(19.5%) were 50 years of age and above. All respondents who went to modern health facilities were married. Thirty nine (50.6%) had primary education, while 38(49.4%) were illiterate. (63.6%) had a family size ranging between five and ten. 38(49.4%) were from Hamar (Table 4).
Table 4 Socio-demographic characteristics of the people who went to modern health facilities for their illness South OmoZone Southwest Ethiopia.
| Variable |
Number (n=77) |
Percentage |
| Age in years |
| <20 |
4 |
5.2 |
| 20 – 29 |
20 |
26 |
| 30 – 39 |
28 |
36.4 |
| 40 – 49 |
10 |
13 |
| ≥ 50 |
15 |
19.5 |
| Sex |
| Male |
57 |
74 |
| Female |
20 |
26 |
| Marital status |
| Married |
70 |
97.1 |
| Single or divorced |
7 |
2.9 |
| Educational level |
| Primary |
39 |
50.6 |
| Illiterate |
38 |
49.4 |
| Religion |
| Cultural |
58 |
75.3 |
| Protestants |
19 |
24.7 |
| Ethnicity |
| Hamar |
38 |
49.4 |
| Nyangatom |
10 |
13 |
| Arbore |
8 |
10.4 |
| Dassanech |
7 |
9.1 |
| Murula |
6 |
7.8 |
| Kara |
5 |
6.5 |
| Kwego |
3 |
3.9 |
| Asset |
| Upto 50 livestock |
36 |
46.8 |
| >100 livestock |
19 |
24.7 |
| 50 to 100 livestock |
18 |
23.4 |
| No livestock |
4 |
5.2 |
Socio demographic variables were cross tabulated to see whether they had statistically significant association with the dependent variable. Among these variables, age, ethnicity, educational status, and religion were found to be statistically significant (Tables 5 and 6). Binary logistic regression was carried out for the statistically significant variables to look for strength of association after controlling confounding variables.
Table 5 Results of cross tabulation of socio-demographic variables on the dependent variable South Omo Zone Southwest Ethiopia February-March, 2012.
| Variables |
Modern health care service |
P value |
OR |
95% CI |
| Use |
Non use |
Lower |
Upper |
| Educational status |
| Primary |
39 |
23 |
0 |
19.46 |
10.542 |
35.904 |
| Illiterate |
38 |
436 |
|
|
|
|
| Religion |
| Cultural |
58 |
446 |
|
|
|
|
| Protestant |
19 |
13 |
0 |
0.089 |
0.042 |
0.19 |
| Ethnicity |
| Hamar |
38 |
152 |
0.002 |
1.968 |
1.209 |
3.203 |
| Others |
39 |
307 |
|
|
|
|
| Age |
| <40 years |
52 |
232 |
0.006 |
0.491 |
0.295 |
0.819 |
| >40 years |
25 |
227 |
|
|
|
|
| Sex |
| Male |
57 |
357 |
0.468 |
1.228 |
0.837 |
6.783 |
| female |
20 |
102 |
|
|
|
|
| Income |
| Owns livestock |
73 |
406 |
0.104 |
2.382 |
0.705 |
2.139 |
| Owns no livestock |
4 |
53 |
|
|
|
|
Table 6 Result of binary logistic analysis of statistically significant variables* modern health care utilization South Omo Zone Southwest Ethiopia February-March, 2012.
| Variables |
Modern health care service |
P value |
Crude OR with 95% CI |
Adjusted OR with 95% CI |
| Use |
Non use |
| Educational status |
| Primary |
39 |
23 |
0 |
19.46(10.54, 35.90) |
20.32(9.76, 42.33) |
| Illiterate |
38 |
436 |
|
|
|
| Religion |
| Cultural |
58 |
446 |
|
|
|
| Protestant |
19 |
13 |
0 |
11.24(5.27,23.95) |
9.11(3.30, 25.19) |
| Ethnicity |
|
|
|
|
|
| Hamar |
38 |
152 |
0.002 |
1.97(1.21, 3.20) |
2.78(1.46, 5.30) |
| Others |
39 |
307 |
|
|
|
| Age |
| <40 years |
52 |
232 |
0.249 |
0.491 |
0.716(0.405, 1.264) |
| >40 years |
25 |
227 |
|
|
|
Individuals with a primary education were 20.3 times more likely to utilize modern health facilities as compared to individuals who are illiterate. Modern health service utilizers are 9.1 times more likely to be followers of protestant religion than cultural belief followers. In addition, having a Hamar ethnic background was found to have a statistically significant association with modern health care service utilization. The Hamar people were 2.8 times more likely to use modern health care service than people with other ethnic background.
Regarding to qualitative part, a total of 48 participants involved in six groups comprised of 8 members from traditional birth attendants, Kebele administrators, clan leaders and elders. A total of six groups were formed which were divided into three male and three female groups. The discussion was conducted using four major headings. The group discussion started with general question whether they had any knowledge about health facilities. Almost the entire group defined it as the place where they go when they get sick. The group discussants were asked the factors that affect outpatient service utilization. The main reasons which had been raised by most discussants were distance of health facilities and cultural belief of pastoralist communities of lack of efficacy for certain health problems which they believe is the acts of the Gods. Some of the participants agreed on the cost of the service, low perceived quality of care, low recognition of seriousness of symptoms and signs, and unmet expectations prevented them from accessing outpatient services.
Some discussants from female group said, According to our culture the female can visit health facilities if and only if she gets permission from her husband.
One of the elder discussants said that ‘’due to long distance of modern health facilities they mostly resort to using traditional healers for treatment’’.
The discussants were asked about decision making in order to visit health facilities. Both male and female groups generally agreed that within household, decisions were made by the husband, whereas when it is done outside of household, decisions made to visit health facilities were by elders.
Some of discussants also said that within the household in absence of the husband, the elder sons were responsible to make decision for any members of the household to visit health facilities.
With regard to the comparison of the costs incurred between modern and traditional treatments, most of both focus group discussants said, the cost of traditional treatment is higher than modern health service, because in case of traditional treatment the traditional healers charge more if they add animal blood on the body of patient and if the healer tells the sin the person has committed which resulted in his or her sickness.
Discussion
Around the world, there is significant unmet need for health care both developed and underdeveloped nations. But problem is very rampant in developing counties [6].
This study has revealed that only 10% of the people who reported to have at least one episode of illness within the one year recall period from January 2011 to January 2012. Visited modern health institutions. This finding is similar with the result of EDHS 2005 which showed 9% modern health utilization in Somali Region. However, the finding of this study differs from the 46.1% reported in mobile pastoralists of Afar region, in North East Ethiopia [5]. The socio cultural difference of two communities and physical access of health facilities might explain the result. Modern health service utilization in Ethiopia appears generally low. An earlier study which summarized the health profile of 52 districts reported that the per capita annual number of visits was 0.23 visits overall, with the mean for urban double that of the rural districts [9].
It was found that 38.1% of the respondents who reported, the most cited reason for not visiting health institutions were the far distance of health institutions from their place of residence. This result is consistent with the finding of studies in camel breeder mobile pastoralists of Chad [10].
Cultural belief of the pastoralists that modern health services lack of efficacy for certain health problems is another common reason identified in this study for not visiting health institutions which had been claimed by 29% of study subjects. Culture, often considered a barrier to health services, can influence knowledge and beliefs of illness as well as the course of treatment for illness. Different studies Chad, Tanzania and Mongolia have shown that culture shapes not only illness treatment, but also illness recognition, perception of illness severity, and confidence in the efficacy of specific treatments for specific illnesses [2,11,12]. The 15.9% of study subjects reported the reasons for not visiting health institutions were low recognition of serious symptoms which was also supported by FGD. Both male and female group agreed that many people only decide to seek care when the patient becomes seriously sick. People expect that most illnesses are simple and will be self-limiting, thus not requiring any investment to seek care. This finding similar with study conducted in 2011 in Southern Ethiopia [13]. The other reasons that were mentioned by 5.7% of study subject as barrier of outpatient service utilization was unmet expectations. Some of FG discussant also raised we expect that the nearest health unit should address all our health care needs when we fall ill; when it does not happen as expected, we become disappointed and then fail to come or delay to come for follow on visits. This finding is also supported by study in Southern Ethiopia [13].
Finally only the 2% of study subject claimed that perceived quality of health service also another barrier for outpatient utilization. This was also blamed by few of FG discussants the poor perceived quality of health service. They mentioned as factors of outpatient utilization with following evidences: lack of treatment according to our preference; absence of required laboratory and diagnostic services; drug shortages in health centers; and long waiting times, especially in government hospitals. This is also similar with study in Tanzania [11].
The most frequent reasons given by FG discussant regarding for not utilizing outpatient service were distance of health facilities and cultural belief of lack of efficacy were mentioned as the main reasons for low utilization of modern health service which is in line with quantitative result and other studies done in Afar and Chad [5,10].
The decision making to visit health facilities were also raised during FGD all discussants agreed up on the decision making within household was usually made by the husband but it is done the elderly outside of the household. This is consistent with study conducted in Afar North East Ethiopia and mobile pastoralists of Chad [5,10].
Another interesting finding came up during focus group discussion with regard to the comparison of the costs incurred between modern and traditional treatment was most of both male and female focus group discussants agreed, the cost of traditional treatment is higher than modern health service. This finding important to support the quantitative result, among the people who were gone to traditional healer and self-treated only 9.3% claimed that the cost of health service was mentioned as barrier for outpatient service utilization and the rest not raised cost as barrier. This finding not similar with pervious study from Afar region [5]. The possible explanations may be the socio-cultural difference of two communities.
The individual who had at least primary education had 20.3 times more likely to utilize modern health services as compared to that with no education. Studies show that education is one of the major socioeconomic factors that influence a person’s behavior and attitude. In general, the higher the level of education of a person, the more aware he or she is about the use of health facilities [14]. Our study has also shown that having at least a primary education is a significant positive predictor of outpatient service utilization.
There was no statistically significant association between gender of the patient and health service utilization in our study. However, another study conducted on modern health service utilization in Kenya pastoralist has shown that males are three times more likely to use modern health services than females because of male domination in decision making to seek health care [15].
This study has found no significant association between health service utilization and age of the patient. According to a study done in Tanzania by Masatu et al. teenagers and persons above the age of 60 were less likely to visit modern health services. The teenage is a period of transition from childhood to adulthood and the prevailing services do not generally seem appropriate for this group of population [16]. The individual whose religion was protestant were more likely to prefer outpatient service utilization than the individual who was cultural belief follower. This study is similar with findings in Afar Dubti and Ghana [14,17]. The Evangelical church of MekanEyesuse role in the provision of health service in different levels of health facilities may explain the observed tendency to outpatient service utilization among the individuals of this faith. The individuals who were from Hamar ethnic background were more likely to prefer outpatient service utilization than the individuals from other ethnic backgrounds. The fact that the Hamar people are relatively more settled than the other pastoralists, better distribution of health facilities due to existence of relatively large number of NGOs and the fact that they make up the majority of the study participants may explain the result. Otherwise the Hamar people have similar educational background, cultural beliefs and income as the rest of the study participants.
Conclusion
In conclusion, this study demonstrated that there is significantly low health service utilization among pastoralist of the South Omo zone of Southern Ethiopia. The most important factors influencing outpatient service utilization were distance of health facilities from their place of residence; cultural beliefs, that modern health institutions may not be helpful for certain disease conditions, low recognition of serious symptoms and unmet expectations. The education level of household head was found to be positive predictor of outpatient service utilization. The individual whose religion was protestant were more likely to prefer outpatient service utilization than the individual who was cultural belief follower. The individuals who were from Hamar ethnic background were more likely to prefer outpatient service utilization than the individuals from other ethnic backgrounds.
Acknowledgements
We would to acknowledge those individuals who support for this successful thesis work. We would like to thank. We would like to extend my appreciation to South Omo Zone Administration, Zonal Health Department and three Woredas for support and facilitating in getting study population. We thank the study respondents and the whole community at large for their wholesome effort and contribution in provision of the information.
Funding
Funding support for data collection was covered by Jimma University. Analysis and interpretation of data and the manuscript writing was done by authors for free.
Availability of Data and Materials
Data will not be shared. During ethical review, it was approved only to analyze data for study objectives and stated that it will not be shared except authors analyzing.
Authors’ Contributions
AK: Developed proposal, analyzed data, wrote report. GD: Participated in proposal development, report writing and coordinated overall process and TH: Participated in manuscript writing. All authors read and approved the final manuscript.
Ethics Approval and Consent To Participate
Ethical clearance was obtained from Jimma University College of Public Health and Medical Sciences Ethical Review Committee. Official letter of cooperation was written to South Omo Zone Administration by the University.
Consent for Publication
Not applicable, no individual detail is presented.
Competing Interests
All authors have no competing interest and declare that this study is original article.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
22963
References
- The decline of pastoralism (1994) In: J Coppock (eds) Conflict and the decline of pastoralism in the horn of Africa. London: The Mac Millan Press. pp: 45-62.
- Weibel D, Schelling E, Bonfoh B, Utzinger J, Hattendorf J, et al. (2008) Demographic and health surveillance of mobile pastoralists in Chad: Integration of biometric fingerprint identification into a geographical information system. Geospat Health 3: 113-124.
- Spicer NJ (2005) Pastoral Sedentarization and health utilization: Changing discourses in the northeast Badia of Jordan. Soc Sci Med 61: 2165-2176.
- Hausmann-Muela S, Ribera JM, Nyamongo IK (2003) Health seeking behavior and health system response. DCCP Working Paper, pp: 1-37.
- Dubale T, Mariam DH (2005) Determinants of conventional health service utilization among pastoralist in Northeast Ethiopia, Addis Ababa Ethiopia. Ethiop J Health Dev 21: 142-147.
- Makinen M, Waters H, Rauch M, Almagambetova N, Bitran R, et al. (2010) Inequalities in health care use and expenditures: Empirical data from eight developing countries and countries in transition. Bull World Health Organ 78: 55-65.
- EDHS (2005) Central statistical authority. Addis Ababa Ethiopia ORC Marco Calverton, USA. pp: 14-20.
- Health and health related indicators (2011) Planning and Programming Department, Ministry of Health Addis Ababa, Ethiopia.
- Larson C, Dessie T (1994) Health in Ethiopia; A summary of 52 Districts health profile. Ethiop J Health Dev 8: 87-96.
- Hampshire K (2002) Networks of nomads: Negotiating access to health resources among pastoralist in Chad. Soc Sci Med 54: 1025-1037.
- Magadia M, Madiseb N, Rodriguez R (2000) Frequency and timing of antenatal care in Tanzania: explaining the variations between women of different communities. Soc Sci Med 51: 551-561.
- Foggin P, Farkas O, Shiirev-Adiya S, Chinbat B (1997) Health status and risk factors of semi-nomadic pastoralists in Mongolia: A geographical approach. Soc Sci Med 44: 1623-1647.
- Damene HM, Gimono W (2011) Understanding barriers to health service utilization in SNNPR, Ethiopia, Addis Ababa Ethiopia.
- Addai I (1998) Demographic and Scio-cultural factors influencing use of maternal health services in Ghana. Afr J Reported Health 2: 1379-1387.
- Mwaniki P, Kambtu E, Mbugua G (2002) Modern Health service utilization by pastoralist in in Turkana District, Northern Province Kenya. Afr Med J 4: 184-187.
- Masatu Mc, Lugoe WL, kvale G, Klepp KI (2005) Health services utilization among marginalized community in Arush Region, Tanzania. East Afr Med J 78: 300-307.
- Melkamu F (2005) Assessment of Factors Affecting Utilization of Maternal Health Care Services in Ayssaita And Dubti, Afar Regional State North East Ethiopia. pp: 63-65.

