Keywords
Patients; Safety; Jordan; Arab; HSOPSC
Background and Objectives
It is a challenge for any healthcare organization to implement new practices to improve the quality of the overall system, as well as patient care and/or patient safety. The first challenge is complexity of healthcare organizations, which tends to be more complex than other organisations for several reasons. Leap et al. [1] stated that essential practices of healthcare employees are often invisible. Secondly, there is the need for major changes in individual behaviour to shift from the culture of ‘blame’ to an objective response to errors. This means shifting the blame toward the systems that allow such errors, rather than blaming the individual. Thirdly, healthcare staff’s fear of losing others' confidence and trust, and thus, fear of damage to personal reputation, need to also be alleviated.
The Ministry of Health (MoH) is one of the largest healthcare providers in Jordan and is making an effort to improve patient safety. Introducing the concept of a ‘culture of safety’ to Jordanian hospitals is a big challenge; it requires efforts from all levels of management, from administrators to supervisors, to make health care safer. This process, however, is expected to progress slowly.
Patient safety, if not measured, cannot be improved. Changing the culture, or even a few practices and policies, requires health-care professionals and especially the top-level administrators and their employees to share a common vision. A good safety system depends on having a culture that supports and encourages employees to report their errors and near misses [1].
Measuring the safety culture will help managers understand its impact on the occurrence of errors. It will help to identify the relative contribution of causal factors to errors [2,3]. All managers should consider the importance of encouraging and supporting the people they supervise when errors are reported by Helmreich et al. [4] Parker [5].
Promoting a culture of reporting errors is applicable to the patient care environment so that staff members learn from each other and help to avoid the occurrence of future errors [6-8]. When addressing safety within one particular health care organization, measuring the existing safety culture may help enlighten management regarding issues that impede making progress in improving safety [9].
Measurement of the patient safety culture has been carried out in several ways, one of which is the use of surveys. Some surveys used have assessed patient-safety features and evaluate the health-professionals’ perceptions of actions and behaviours in their work environment. The results may help to determine which actions and behaviours, relative to safety requirements and regulatory goals, should be prioritized for process improvement programmes. The Hospital Survey on Patient Safety Culture (HSOPSC) was developed by the U.S. health department’s Agency for Healthcare Research and Quality (AHRQ) and has been widely used in the U.S. at Jordanian MoH hospitals, the current measurement of safety focuses on counting errors and incidents that occur. As an alternative, a proactive approach would provide the hospitals’ management with the status of the safety culture in their hospitals as well as a baseline measurement to guide strategies to improve the safety culture related to increased patient safety. Since there has been no previous literature or current research studies in Jordanian hospitals that measure an organization’s safety culture, the purpose of this study is to validate a modified measurement tool (i.e. survey). At the same time, the survey offers the opportunity to measure health-staff perceptions of the safety culture in Jordanian MoH hospitals. This study will provide these hospitals with an empirical baseline measurement of the safety culture and an important quantitative outcome by which future safety improvements can be evaluated.
These goals can be accomplished through the following initiatives:
1. Provide a validated questionnaire version in Arabic of the survey tool that has been applied in more than 1,000 hospitals in the United States.
2. Test the validity and reliability of a modified measurement tool (survey) for the patient safety culture in Jordanian MoH hospitals.
3. Pilot test the perceptions of the health staff about the patient safety culture in Jordanian MoH hospitals using this survey tool.
Methodology
Using a cross-sectional design, a survey was used to measure the dependent variable of health-staff perceptions about the safety culture in their respective hospital departments: Medical, Surgical, Intensive Care Unit, Obstetrics and Gynaecology, Paediatrics, Accident and Emergency and Theatre.
The setting for the study was public (i.e. MoH) hospitals. A letter was sent to three MoH hospitals inviting them to participate as entire organisations in the study. Two replied; one was selected for the first round as a pilot site.
Sample
Multistage-stratified simple random sampling was used. Staff subgroups working in each hospital that had direct contact with patients, or whose work directly affected the patients, were stratified by work group into:
1. Physicians
2. Nurses
3. Pharmacists
4. Dieticians
5. Physiotherapists
6. Laboratory specialists and technicians
7. Radiologists and technicians.
A simple random sample was selected from each group. The participants were recruited by invitation letter distributed to all of the staff in the target hospital by the nursingdevelopment unit staff and students from the Faculty of Nursing at Mutah University. Participation in the study was voluntary and no personal information was collected.
Instrument design and development
Survey design
The HSOPSC survey (2009 version) was modified and used for this study. Although the survey is provided free of license, the first author (AN) contacted the owners and gained permission to translate it into Arabic. The survey consists of 12 safety-culture dimensions. Forty-two items are scored on five point Likert-type response scales.
The survey places an emphasis on patient safety issues and on error and event reporting. The survey measures seven unit-level aspects of the safety culture:
1. Supervisor/Manager expectations and actions promoting safety (4 items)
2. Organizational learning—continuous improvement (3 items)
3. Teamwork within units (4 items)
4. Communication openness (3 items)
5. Feedback and communication about error (3 items)
6. Non-punitive response to error (3 items)
7. Staffing (4 items)
In addition, the survey measures three hospital-level aspects of the safety culture:
1. Hospital management support for patient safety (3 items)
2. Teamwork across hospital units (4 items)
3. Hospital handoffs and transitions (4 items)
Finally, four outcome variables are included:
1. Overall perceptions of safety (4 items)
2. Frequency of event reporting (3 items)
3. Patient safety grade (of the hospital unit) (1 item)
4. Number of events reported (1 item)
This survey was adapted from a tool that was originally developed to assess the culture of patient safety in American hospitals. It was fitted to an Arabic setting and particularly the Jordanian context, before commencing with research activities.
Ethics approval
Approval was obtained from the Research Ethics Committee in the University of Mutah. A package of invitation cards, information sheet, survey and consent forms was forwarded to the study population by their hospital directorate and those participating dropped their consent forms in a designated box within the hospital or handed them back to the survey distributors. The keys of the box were securely kept, only with the principal investigator.
Data collection
The hospital directorate sent invitation cards to the potential study participants using the internal mail, along with posters promoting the study. Only those who expressed willingness to take part completed the survey.
Data analysis and results
This study used Excel and SPSS 16.0 for Windows to perform the statistical analysis. Descriptive statistics of the demographic characteristics of respondents, characteristics of hospitals and the average percentage of positive responses on the patient safety culture were computed.
The average percentage of positive responses, defined as the average of the item-level percent positive responses within an HSOPSC dimension, represented positive reaction(s) toward the patient safety culture.
The data was coded and entered to Excel and then converted to SPSS for further analysis. Open-ended items in the survey were analysed by categorising and giving codes to similar items. The rest of the items was analysed primarily using frequencies. The analysis involved the patterns of the responses; survey items were grouped according to the safety culture dimensions. Results were disseminated through presentations in Faculty of Nursing and in the hospital, and a report presented to the hospital.
Results
Demographic statistics
We distributed 480 surveys to all staff members supposed to have direct contact with patients in a MoH regional hospital in Jordan. A total of 287 respondents from this group completed the survey and returned it; thus representing a response rate of nearly 60 percent.
Survey reliability and validity
The English version of the survey was initially translated to Arabic. This was then pretested during cognitive interviews with university hospital staff in Jordan to make sure that items were easy to understand and relevant to patient safety in an Arabic hospital setting. Then the items were appropriately revised and the survey was given to an academic professional in translation for back-translation. A comparison between the original English version and the translated one showed that source and target were equivalent.
A committee composed of five quality and research officers (from two hospitals that were asked to participate in the pilot) and two faculty members from Mutah university was assembled to discuss the results and the comments provided by the participants regarding the questionnaire items. Minor changes were made to the content of the survey based on the participants’ comments and the committee members’ suggestions.
Internal consistency of the instrument was measured by calculating Cronbach’s coefficient alpha for the 12 composites. The values ranged from 0.119 for ‘Staffing’ and 0.845 for ‘Frequency of events reported’ (Table 1). A good overall scale Cronbach’s alpha score of 0.797 was obtained. Reliability test was conducted using Cronbach’s alpha and indicated reliable consistency.
| Dimension |
Cronbach’s alpha |
| Teamwork within units |
0.764 |
| Supervisor/Manager expectations and actions promoting patient safety1 |
0.57 |
| Organizational learning—continuous improvement |
0.502 |
| Management support for patient safety |
0.536 |
| Overall perceptions of patient safety |
0.64 |
| Feedback and communication about errors |
0.644 |
| Communication openness |
0.347 |
| Frequency of events reported |
0.845 |
| Teamwork across units |
0.595 |
| Staffing |
0.119 |
| Handoffs and transitions |
0.723 |
| Non-punitive response to errors |
0.418 |
| Overall scale Cronbach’s alpha |
0.797 |
Table 1: Internal consistency of the instrument.
Patient safety in the hospital was measured by assessing different components (Figure 1).
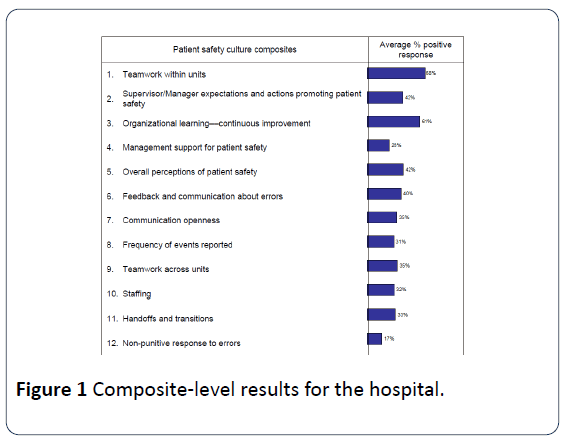
Figure 1: Composite-level results for the hospital.
The component that gained the highest positive response from participants was the
Teamwork within units’ with an average of 68% (Figure 2). On the other hand, the lowest average percentage was the ‘Non-punitive response to errors’ with 17% average positive response. Meanwhile, the overall perception of patient safety was only 42%.

Figure 2: Number of patient-safety events reported by the participants.
The survey has a specific question on the number of events related to patient safety filed by the participants during the year immediately prior to conducting the survey (Figure 2).
More than one-third of participants (40%) reported at least one event while 60% reported no event. An alarming result was that 20% reported three or more events.
Participants’ self-assessment of the level of patient safety within their units showed that most were satisfied. However, almost 10% rated patient safety as poor or failing. Regarding self-assessment of team work and supervisor’s promotion of team work, more than two-thirds of participant held positive views on team work, while half of participants reported being positive regarding ‘Supervisor/Manager expectations and actions promoting patient safety’.
With regard to patient safety within the hospital overall, nearly two-thirds (63%) of participants reported ‘excellent’ (20%) or ‘very good (43%). Only 10% reported ‘poor’ (8%) or failing (2%) (Figure 3).
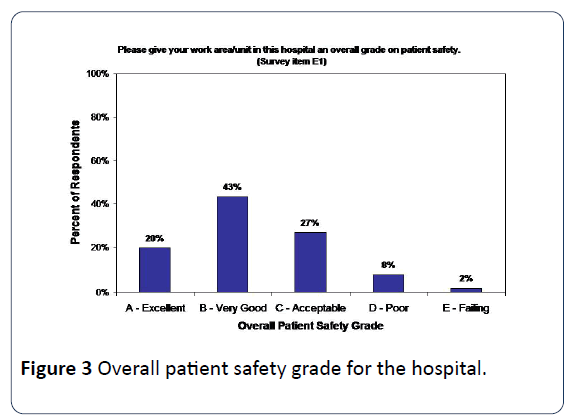
Figure 3: Overall patient safety grade for the hospital.
Despite nearly two-thirds of respondents indicating high scores for patient safety, almost half of the participants (46%) responded positively to Item 2.3 of figure 3, i.e. “Whenever pressure builds up, my supervisor/manager wants us to work faster, even if it means taking shortcuts.”
Two behaviours that are closely related to patient safety are the level of ‘Teamwork within units’ and ‘Supervisor/Manager expectations and actions to promote patient safety’. Participants tended to be very positive about ‘Teamwork within units’ with some two-thirds (65%) to nearly threequarters (71%) of the participants holding very positive views of teamwork (Figure 4).
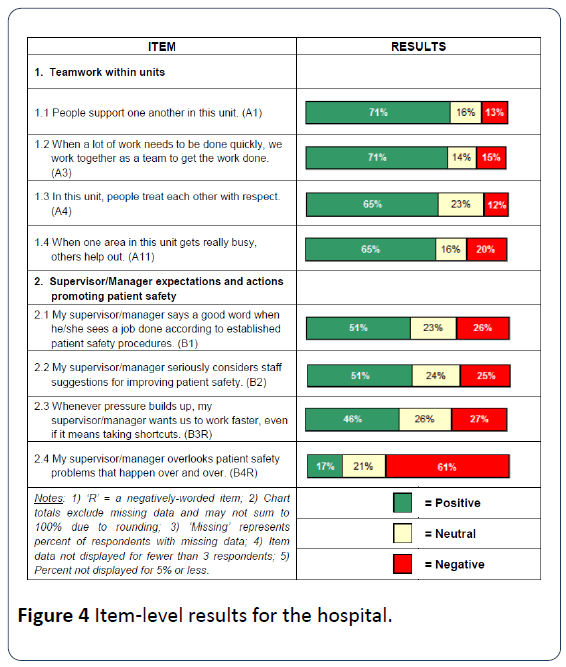
Figure 4: Item-level results for the hospital.
When asked to assess management behaviour in support of patient safety, the participants held positive views; i.e. slightly more than half (51%) felt that management encouraged good behaviours related to patient safety. Even more participants (61%) responded that management wouldn’t tolerate repeated errors in patient safety. However, a fairly large number of participants (46%) responded that under pressure, management insists on faster work that could include shortcuts.
Clearly this impacts patient safety, and a much smaller segment (27%) disagreed that management insisted on faster work, including shortcuts.
Discussion
Assessing the patient safety culture is the first step in improving the quality of health service provided to patients and to reducing errors in service provision. Many assessment tools have been developed by leading healthcare organizations (e.g. World Health Organization, Institute of Healthcare Improvement and Agency for Healthcare Research and Quality (AHRQ), the Health Division of the Organization for Economic Development and Cooperation (OECD) and the Agence nationale d'accréditation et d'évaluation en santé (ANAES). The application of any of these organizations’ tools in the Arabic-speaking region has not been previously tested. This study adopted the HSOPSC and translated it into Arabic. The tool was found to be valid and reliable after piloting it in one of the public hospitals in Jordan on a sample of 287 respondents.
The results of this study indicate health personnel in Jordanian hospitals perceive the patient safety culture as positive. The highest positive perception was for the component of ‘Teamwork within units,’ which corresponds with findings from other studies in other areas of the world described by Chen et al. [10], Rudman et al. [11] and Smit et al. [12,13]. However, the lowest positive perception was for ‘Non-punitive response for errors’. This may indicate that the hospital management is not sufficiently focused on improving patient safety, and this affects the perceptions of the staff.
The results from this study point to the importance for Jordanian hospitals to work on multiple issues:
1. Assess patient safety in all health organizations in the country.
2. Develop regulations for patient safety in all types of health organizations.
3. Support and encourage a non-punitive culture in order to improve the quality of health-care services.
We recommend an emphasis on improving the organizational processes in order to improve the patient safety culture. This can be developed through adoption of organizational initiatives that emphasize certain policies:
1. The organization focuses on process improvement that sees measurable consistency and eventual standardization of all processes in the organization as benchmarks achieved.
2. Continuous improvement of processes relies on a system that supports learning from mistakes and sharing knowledge.
3. An important element in the early implementation of a system of continuous improvement is the need to eradicate blame and to protect the health-care professional’s right to confidentiality when reporting errors. Eventually, though, the goal should be the transition to an ‘open environment’ where blame is seen as an impediment to improving patient safety. Errors, per se, present a learning opportunity and one goal should be the chance for open discussion and investigation to remove the cause(s) of an error from the system.
4. Managers’ actions should enhance evidence-based practice, teamwork and give credit to good supervision, audit and reporting practices as well as open disclosure and discussion when errors occur. Health-care professionals will need support and on-going training in order to improve safe practices that lead to provision of high-quality care.
5. Nevertheless, despite implementation of policies that encourage quality improvement, proper accountability for all actors involved is required and should be in place; actors include the providers, patients and other stakeholders.
Limitations
The study has some limitations. It was carried out in one hospital and in one rural region; therefore, it needs to be expanded. A large sample is required to reliably extend the results to larger groups. In addition, including the patients in the sample would enhance applicability of study results. The study also attempted to assess the overall safety culture. This might not necessarily assure patient safety; other benchmarks need to be considered and initially measured, as well.
Conclusion
The Arabic translation of the HSOPSC survey was found to be valid and reliable after piloting it in one of the public hospitals in Jordan. Hospital health-care personnel in Jordan perceive the patient safety culture as positive. The highest positive perception was for the component of ‘Teamwork within units’. Application of this tool and support for the patient safety culture should be priorities within the provision of health services in Jordan.
11306
References
- Leap LL, Berwick DM (2005) Five years after to err is human; what have we learned. JAMA 293: 2384-2390.
- Toole M (2002) The relationships between employees' perceptions of safety and organizational culture. Journal of Safety Research 33: 231-243.
- Zohar (2000) A group-level model of safety climate: Testing the effect of group climate on microaccidents in manufacturing jobs. Journal of Applied Psychology 85: 587-596.
- Helmreich RL (2000) On errors management: lessons from aviation. BMJ 320: 781-785.
- Parker D (2009) Managing risk in healthcare: understanding your safety culture using the Manchester Patient Safety Framework (MaPSaF). J NursManag 17(2): 218-222.
- Donnelly LF, Dickerson JM, Goodfriend MA, Muething SE (2009) Improving patient safety: effects of a safety program on performance and culture in a department of radiology. AJR Am J Roentgenol 193: 165-171.
- Hartmann CW, Meterko M, Rosen AK, Shibei Z, Shokeen P, et al. (2009) Relationship of hospital organizational culture to patient safety climate in the Veterans Health Administration. Med Care Res Rev 66: 320-338.
- Tiessen B (2008) On the journey to a culture of patient safety. Healthc Q 11: 58-63.
- Sorra J, Nieva V, Fastman BR, Kaplan H, Schreiber G, et al. (2008) Staff attitudes about event reporting and patient safety culture in hospital transfusion services. Transfusion, 48: 1934-1942.
- Chen IC, Li HH (2010) Measuring patient safety culture in Taiwan using the Hospital Survey on Patient Safety Culture (HSOPSC). BMC Health Services Research 10: 152.
- Rudman WJ, Bailey JH, Garrett PK, Peden A, Thomas EJ (2006) Team and safety culture in small rural hospitals in Missisippi Patient Safety and Quality Healthcare.
- Smits M, Wagner C, Spreeuwenberg P, van der Wal G, Groenewegen PP (2009) Measuring patient safety culture: an assessment of the clustering of responses at unit level and hospital level. QualSaf Health Care 18: 292-296.
- Agency for Healthcare Research and Quality (2009) Hospital Survey on Patient Safety Culture. Rockville, MD: Agency for Healthcare Research and Quality.

