Keywords
Pneumo sinus dilatans, sinusitis, endoscopic sinus surgery
Introduction
Pneumosinus dilatans (PD) is a rare condition that results in facial deformity. PD is caused by an abnormal dilatation of the Paranasal sinuses, which contain only air and are lined by normal mucosa. Meyes first described the disease now known as PD in 1898 [1]. However, in 1918, Benjamin first assigned the name Pneumosinus dilatans to this facial deformity [2]. An exhaustive review of the literature by Borelli et al in 1979 yielded only 51 reported cases of PD. [3]. In recent years, a few more cases have been reported. Most involved the frontal sinus, although the Maxillary sinus, Ethmoidal cells, and Sphenoidal sinus can also be affected [4-6].
Abnormal expansions of the frontal sinuses have also been given the diagnosis of pneumocele, pneumosinus frontalis, sinus hypertrophy, aerocele, hyperpneumatization, and sinus ectasia. It is possible that these terms describe the same clinical condition. Urken et al. [7] classified paranasal sinus pneumatic dilatations into three categories according to clinical symptoms, radiologic enlargement, and thinning of the sinus walls. In order of increasing severity, the classific
ations were hypersinus, pneumosinus dilatans, and pneumocele. However, it is not clear how these diseases are related.
The etiology and pathogenesis of this unusual process are not yet determined. PD is often an unexpected radiologic finding; however, in most cases, it is diagnosed by the recognition of a frontal deformity. Common complaints patients present with include local pain caused by tissue expansion or frontal nerve compression, headache, frontal paraesthesia or sensory deficit, olfactory loss, and ophthalmic disturbances. Stretch and Poole also reported a case of PD-associated blindness caused by osteodysplasia of the optic canals and compression of the optic nerves [8].
X-rays, clinical findings, and hormonal examinations may help to differentiate PD from other acquired deformities of the frontal bones, such as acromegaly, exostosis, and mucocele frontalis. PD has been described in both an isolated form and in association with other diseases, such as arachnoid cyst, [9] cerebral hemiatrophia, [10] meningioma, [5,11,12] and Klippel-Trenaunay-Weber syndrome [13].
Case report
A 38 -year-old female patient presented with history of left sided nasal obstruction since 2 years which was insidious in onset and progressive in nature, associated with intermittent anterior and post nasal discharge, with no history of Headache, Fever or swelling over the sinuses. Thorough ENT examination was done and there was mild septal deviation to the left side and mucopus was seen in the left middle Meatus and there was no Para Nasal Sinuses tenderness.
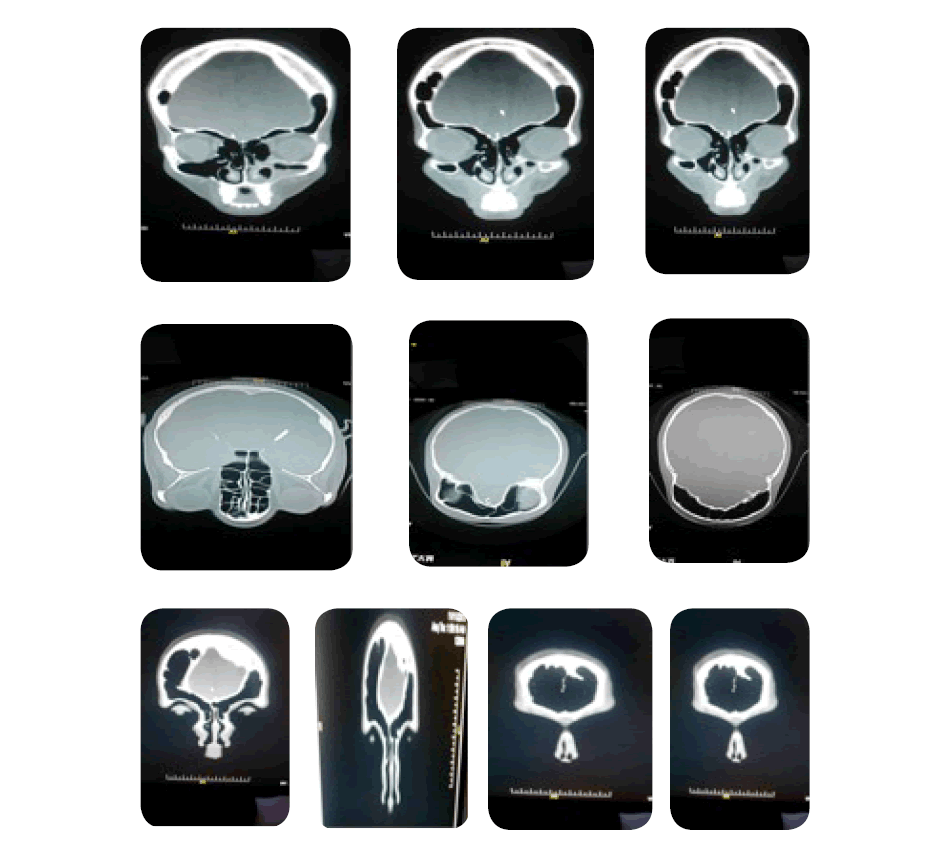
Computed tomography of PNS revealed mucosal thickening of the left maxillary sinus along with obstruction of left ostio meatal complex and abnormally dilated bilateral frontal sinus occupying the whole of the frontal bone and almost extending till the parietal bones. No signs of pathologic formations like sinusitis, cyst, or mucocele were detected in the frontal sinus cavity. Radiologic examinations did not reveal any sign of frontal fracture. Incidentally PD of frontal Sinus was found in this case in CT scan of Paranasal sinus and Left Maxillary Sinusitis was surgically treated by Middle Meatal Antrostomy by Endoscopic sinus surgery.

Discussion
The etiology and pathogenesis of PD is still a matter of discussion. Various hypotheses have been proposed to explain its pathogenesis. Benedikt et al proposed spontaneous drainage of a frontal mucocele as a pathogenic mechanism [14]. Other authors have described cases in which patients reported spontaneous, profuse nasal discharge, supporting this mechanism [7]. However, most patients fail to give such a history.
Alterations of growth -and sex- hormone levels have also been implicated in PD [15]. Such alterations result in a disturbance in the control of osteoblastic activity, leading to excessive bone growth and abnormal sinus pneumatization and expansion. Unfortunately, there is no evidence to support this theory, as stated by Smith et al. [16] who did not record any hormonal alterations in the case they reported. Prott, who also found no hormonal alterations in his patients, suggested that enlargement of the sinus could have been secondary to an increase in intrasinus pressure [17]. This increase in pressure could have been caused by an efferent duct obstruction with a valve mechanism; Harrison and Young described evidence for this in 1955 [18]. However, few simple, anatomically demonstrable valves have been reported by other authors. Candan et al. demonstrated an increased intrasinus pressure caused by a check-valve mechanism [19]. Carta et al. reported a case of PD with diplopia, proptosis, ophthalmoplegia, and compressive optic neuropathy [20]. The authors attributed the amaurosis to changes in air pressure. These changes, caused by probable valve obstruction of the frontal sinus, resulted in optic nerve compression. Endoscopic restoration of nasalantral communication resulted in a full recovery.
Urken et al. also discussed the valve mechanism theory [7]. However, they were unable to formulate a clear, possible etiology and pathogenesis for PD, despite examining a large number of asymptomatic patients and six reported cases of PD. This was because of the focal nature of many of the reported cases and the remoteness of the involved areas from the nasofrontal recess. In our case, the finding of a mucosal extroflexion in the frontal recess could support a valve mechanism, but no clinical signs or surgical evidence of increased sinus pressure was detected.
Although our experience is limited to this case, based on a review of the reported cases we have reached the opinion that, regardless of etiology, only two different forms of PD likely exist, each with specific related clinical signs. The first form leads to increased sinus pressure with early optical signs and symptoms. In the second form, the frontal deformity is the major complaint, and optical signs may be absent or late.
Despite the confusion about the pathogenesis and classification of PD, in our opinion, the therapeutic options for treating PD are quite clear. In hypertensive patients with symptomatic PD but without significant frontal bossing, the treatment of choice appears to be functional endoscopic sinus surgery directed at treating the sinus duct obstruction. When frontal bossing is the major complaint, endoscopic surgery is not effective; in such cases, open surgery with anosteoplastic flap is indicated.
Various open procedures have been described, and most are effective. However, increased attention to aesthetic results requires some technical improvement. Prott described frontal bone infracturing, but the aesthetic results are unpleasant [17]. Urken et al. treated frontal bossing by creating an osteoplastic flap, with a recession of the anterior table into the sinus, followed by fat obliteration of the remaining cavity [7]. The aesthetic results were not reported. Pospisil and Balmer proposed frontal osteotomy with ostectomy [21]. The space created by the difference in size of the remaining reduced anterior frontal bone and the margins of the original sinus was packed with bone chips and Surgicel. However, a large deformity causes a difference in curvature, which can require excessive fragmentation of the anterior plate to fit the frontal bone. We think that a radial or an ‘alternate’ osteotomy (a series of alternating osteotomies on opposite sides of a very convex piece of bone that allow the bone to be pulled apart in a zigzag manner) of the anterior sinus wall permits its compression, leading to better control of frontal projection and contour. Sinus exclusion and fat or bone obliteration help to minimize the possibility of recurrence.
In conclusion, when endoscopic sinus surgery is not suitable for correcting a clear frontal valve obstruction, and when a frontal deformity needs to be corrected, open treatment is the first choice of treatment in PD.
5836
References
- Meyes, WP. Mittheilung eines Falles vermatchlicher Pneumatocoele des Sinus frontalis. Montatsschr Ohrenheilkd 1898; 32: 467-9.
- Benjamin, LE. Pneumosinus frontalis dilatans. Acta Otolaryngol 1918; 1: 412-22.
- Borelli, G., Torsello, G., Gualtieri, G. Sphenoidal pneumosinus dilatans. A case report. Radiol Med. 1979; 65: 735-9.
- Tovi, F., Gatot, A., Fliss, DM. Air cyst of the maxillary sinus (pneumosinus dilatans, pneumocoele). J Laryngol Otol. 1991; 105: 673-5.
- Hirst, LW., Miller, NR., Hodges, FJ III. et al. Sphenoid pneumosinus dilatans. A sign of meningioma originating in the optic canal. Neuroradiology 1982; 22: 207-10.
- Reicher, MA., Bentson, JR., Halbach, VV. et al. Pneumosinus dilatans of the sphenoid sinus. Am J Neuroradiol. 1986; 7: 865- 8.
- Urken, ML., Som, PM., Lawson, W. et al. Abnormally large frontal sinus. II. Nomenclature, pathology, and symptoms. Laryngoscope 1987; 97: 606-11.
- Stretch, JR., Poole, MD. Pneumosinus dilatans as the aetiology of progressive bilateral blindness. Br J Plast Surg. 1992; 45: 469-73.
- Dross, PE., Lally, JF., Bonier, B. Pneumosinus dilatans and arachnoid cyst: A unique association. Am J Neuroradiol. 1992; 13: 209-11.
- van Schayck, R., Niedeggen, A. Pneumosinus dilatans after prolonged cerebrospinal fluid shunting in young adults with cerebral hemiatrophy. A report of two cases and review of the literature. Neurosurg Rev. 1992; 15: 217-23.
- Dhillon, RS., Williams, DC. Pneumosinus dilatans. J Laryngol Otol. 1987; 101: 828-32.
- Spoor, TC., Kennerdell, JS., Maroon, JC. et al. Pneumosinus dilatans, Klippel-Trenaunay-Weber syndrome, and progressive visual loss. Ann Ophthalmol. 1981; 13: 105-8.
- Benedikt, RA., Brown, DC., Roth, MK. et al. Spontaneous drainage of an ethmoidal mucocele: A possible cause of pneumosinus dilatans. Am J Neuroradiol. 1991; 12: 729-31.
- Gardel, J., Maduro, M. Une observation de pneumosinus dilatans. Ann Otolaryngol Chir Cervicofac. 1965; 82: 619-21.
- Smith, IM., Maran, AG., von Haacke, NP. Pneumosinus dilatans. Ann Otol Rhinol Laryngol 1987; 96: 210-12.
- Prott, W. Pneumosinus dilatans der stirnholen. Laryngol Rhinol Otol. 1977; 56: 277-82.
- Harrison, MS., Young, A. Pneumonsinus frontalis. J Laryngol. 1955; 69: 108-14.
- Candan, S., Muhtar, H., Ciftci, A. Der pneumonsinus dilatans frontalis. Laryngorhinootologie 1998; 69: 552-3.
- Carta, A., Castelnuovo, P., Delitala, F. Neuro-ophthalmological presentation of pneumosinus frontalis. Neuro-ophthalmology 1999; 21: 233-240.
- Pospisil, OA., Balmer, MC. Pneumosinus dilatans. Br J Oral Maxillofac Surg. 1988; 26: 375-80.

