Casanova-Peño I, Gómez-Vicente L, Cuadrado ML, Porta-Etessam J*
Neurology Department. Hospital Clínico San Carlos. Madrid. Spain
*Corresponding Author:
Jesús Porta-Etessam C/ Andrés Torrejón
15, 7º 28014 Madrid,
Phone: +34 667 062 490
E-mail: a.larner@thewaltoncentre.nhs.uk, jporta@yahoo.com,
Primary orbital varices are infrequent congenital vascular abnormalities resulting from the pathological enlargement of one or more venouschannels of the orbit. We report a patient suffering ocular pain that appeared when the patient was bending over or lying.A 68 years-old woman consulted in our office because of an ocular pain that appeared when the patient was bending over or lying. Therewas no proptosis and neuro-ophthalmological examination including pupils’ reflexes, ocular mobility and visual acuity was normal. Thepatient was evaluated by computed tomography examination which revealed a faintly, enhancing lesion in the left inferomedial retrobulbararea.The clinical presentation of primary orbital varices typical presents with exophthalmos that becomes evanescent in dependent positionsand in certain situations that increase intraorbital pressure. However, in patients suffering from bending over and lying ocular pain wemust suspect orbital varices even without positional exophthalmos.
Key words
Orbital varix, postural headache, ocular pain, bending over, intracranial hypotension.
Introduction
Primary orbital varices are infrequent congenital vascular abnormalities resulting from the pathological enlargement of one or more venous channels of the orbit [1,2]. The clinical syndrome is usually characterized by intermittent filling and emptying of the varix, resulting in variable proptosis. In infants, eye bulging during crying or orbital ecchymoses should raise this diagnostic possibility [3]. We report a patient suffering ocular pain that appeared when the patient was bending over or lying.
Case reports
A 68 year-old woman consulted in our office because of a 3-month history of ocular pain with a characteristic postural pattern. It appeared when lying flat or bending over, and was relieved by standing. The patient denied any autonomic feature, or the association with dizziness, vertigo, visual or auditory disturbances. There was no proptosis and physical, neurological and neuroophthalmological examination including pupils’ reflexes, ocular movility and visual acuity was normal. There was not fatigability or ocular bruit. The patient was evaluated by orbital computed tomography examination (figure 1a-b) which revealed an enhancing lesion in the left inferomedial retrobulbar area and an MR angiogram ruled out caroid-cavernous fistulas.
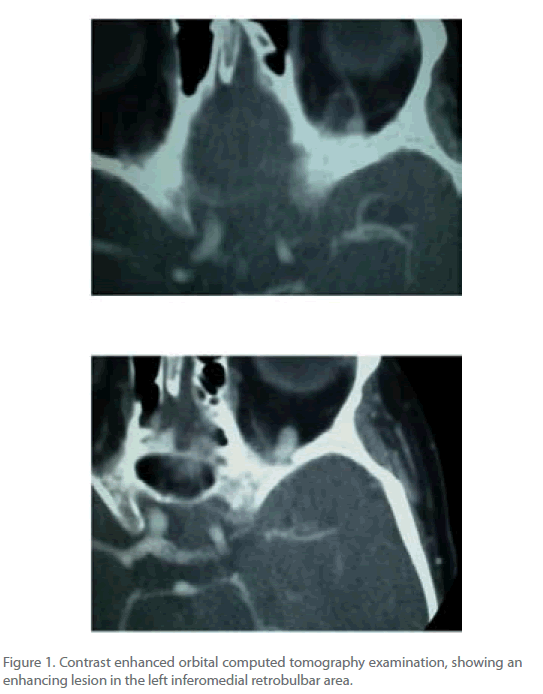
Figure 1. Contrast enhanced orbital computed tomography examination, showing an enhancing lesion in the left inferomedial retrobulbar area.
Discussion:
We present a case of postural headache. Postural headaches are usually related to low pressure organic fluid physic changes. The most common postural headache is intracranial hypotension headache. In these patients the headache usually worsens within 15 minutes after sitting or standing and improves upon lying over [4-5]. The traction of pain sensitive intracranial and meningeal structures and bridging veins is thought to cause headache and other related symptoms. Paradoxical postural headaches have also been described with cerebrospinal fluid leaks, with the head pain occurring in horizontal positions and fading when the patient is upright. The pathophysiology of these latter headaches could be related to congestion and dilation of cerebral venous sinuses and large veins [6].
We present a postural headache related to an orbital varix. Usually the clinical presentation of primary orbital varices includes exophthalmos that becomes evanescent in dependent positions. Our patient did not have exophthalmos at the time of consultation and the only symptom was a postural pain. The pain could be due to an increase of intravenous and intraorbital pressure when the patient was lying over. However, in patients suffering from bending over and lying ocular pain we must suspect orbital varices even without positional exophthalmos.
2321
References
- Weill A, Cognard C, Castaings L, Robert G, Moret J. Embolization of an orbital varix after surgical exposure. Am J Neuroradiol 1998;19:921-3.
- Secil M, Soylev M, Ada E, Saatci AO. Computerized Medical Imaging and Graphics 2001; 25: 243-247.
- Orbital disease in neuro-ophthalmology. In: LiuGT, Volpe NJ, Galetta SL (eds). Neuroophthalmology: diagnosis and management. Pp 651-697. Philadelphia. WB Saunders Company. 2001.
- Headache Classification Subcommittee of the International Headache Society. The international classification of headache disorders, 2nd edn. Cephalalgia 2004; 24 Suppl 1:1–160.
- Garcia-Morales I, Porta-Etessam J, Galán L, Lagares A, Molina JA. Recurrent subdural haematomas in a patient with spontaneous intracranial hypotension. Cephalalgia 2001; 21: 703-705.
- Mokri B, Aksamit AJ, Atkinson JLD. Paradoxical postural headaches in cerebrospinal fluid leaks. Cephalalgia 2004; 24: 883.

