Keywords
Labour pain; Tigray regional hospitals; Pain management; Skilled attendant
Introduction
For all woman labour involves pain, often the pain of labour is the most severe pain that a woman ever has to face. The pain a woman experiences during labour and birth is subjective, individualized and caused by a number of interrelating factors. Physical, affective, psychosocial and environmental components all shapes the pain experience [1].
Pain relief in childbirth is subject to many social and cultural modifiers, which continue to change. There is no other circumstance in which it is considered acceptable for a person to experience untreated severe pain even while under a physician’s care [2]. Control of pain rather than absolute amelioration is seen by many to provide greater satisfaction. The importance of analgesia as a contribution to overall satisfaction has been recognized increasingly in the last century [3]. Sir James Simpson, professor of Obstetrics at the University of Edinburgh first advocated the use of ether for Obstetric analgesia in 1850’s [4]. Queen Victoria in 1853 had the pains of childbirth relieved by intermittent whiffs of chloroform and thereafter the opposition from churches regarding obstetric analgesia remained silent [5].
Supporting women at delivery is an essential part of public health care. The term 'labor support' refers to continuous nonmedical care of a laboring woman. It includes physical comforting such as touching, massaging, bathing, grooming, applying warmth or cold; and emotional support such as continuous companion, reassurance, encouragement, anticipatory guidance, information provision, and non-medical advice. Labor support and care may also involve procedures and facilitation of communication between the woman and staff to assist her in making informed choices. Furthermore, it may comprise emotional support for the woman's partner [6,7].
Labour pain management is generally classified in to two pharmacologic and non-pharmacologic labour pain management, the difference is by the use of drug for pain relief through pharmacologic pain management.
Utilization of labour pain management methods varies from place to place even it varies from one setup to another. In developed nation pharmacologic way of pain relief is the preferred one whereas in developing countries most of the time non-pharmacologic way of managing labor pain is utilized [8].
A study in Colombia reported inequity distribution of epidural analgesia in developed versus developing countries, in developed countries the use of epidural analgesia during labour is around 60% of deliveries; covering France 75%; Sweden 71% and Colombia 31.5%. In other less developed countries such as South Africa, only 21% of women used epidural [9]. In our country Ethiopia as a study conducted on all obstetric care givers in Amhara Regional State Referral Hospitals showed the overall utilization of obstetric analgesia in labour pain management was 40.1% which showed only non-pharmacologic methods. The utilization of pharmacologic obstetric analgesia methods was zero [10]. Which shows poor utilization of labour pain management methods in Ethiopia as compared to other countries, this study also report factors for poor utilization like professional’s qualification and knowledge were found statistically associated with utilization of obstetric analgesia. But in general factor for utilization of labour pain management methods broadly classified in to individual factor, institutional factor and background characteristics of health professional [8].
Materials and Methods
Study design
Hospital based cross-sectional study.
Study area and period
The study was conducted at all general hospitals found in tigray region from October 01-30, 2016. Tigray region is the northernmost of the nine regions of Ethiopia. Tigray is the homeland of tigray, irob and kunama people. Tigray is also known as region 1 according to the federal constitution. Its capital is Mekelle also known as the northern star. Tigray is bordered by Eretria to the north, Sudan to the west, afar region to the east and the Amhara region to the south and southwest. According to the projected census of 2007, the region has a total population of 4,806,843 (3,787,667 rural and 1,019,176 urban). According to the 2011 report of TRHB Health care coverage in Tigray region reaches around 83%. Health care services delivered through 2 referral hospitals, 14 general hospitals, 20 primary hospitals, 214 health centers and 613 health posts. Regarding human power, currently there are 21 specialist doctors, 55 general practitioners, 2495 nurses, 1262 health extension workers and other different professionals providing preventive and curative services in the above mentioned institutions.
Sample size determination
All skilled attendants working at labour wards in all general hospitals of tigray region were taken like a census which was in number two hundred thirty three.
Sampling procedure
There are fourteen general hospitals in tigray region, which are; sehul (shire), Adigrat, Mekelle, Maychew (lemlem Karl), kidst Mariam (Axum), Adwa, Meareg (dansha), Abyiadi, Shiraro, Wekero, Kiha, korem, Alamata, Humera (kahsaye) hospital. All two hundred thirty three skilled attendants who were working at labour ward and follow laboring mother in the above general hospitals during the study period was included.
Data collection tools and procedures
Structured and pretested interviewer-administered questionnaires was prepared and utilized after reviewing relevant literatures. All skilled attendants who were working in labour wards of all the general hospitals found in tigray region and who fulfilled eligibility criteria was interviewed by structured questionnaires. Data was collected by structured interviewer-administered pre tested questionnaires and fourteen data collector was recruited one in each general hospital and four supervisor supervised the data collection.
Data quality control
Training was provided for data collectors for making common understanding of the study in general and the questioner in particular and pretest was conducted in Ayder referral hospital by delivering interviewer-administer questioner to skilled attendants to shape the questioner.
Data analysis
After data collection, the questioners were checked for completeness and code was given before data entry. Data was entered in to computer by Epi-info version 7 and exported to SPSS version 20 for further analysis. Descriptive statistics were computed to determine Frequencies and summary statistics (mean, standard deviation, and percentage) to describe the study population in relation to socio-demographic and other relevant variables. Data were presented using tables, graphs and figures. Variables with P value <0.05 in Bivariate analysis were transferred to multivariable analysis. Multivariable analysis was done to test association between predictors and dependent variables.
Ethical clearance
Ethical approval was obtained from the IRB (institutional review board) of Mekelle University, College of Health Sciences. Letter of permission was obtained from tigray regional health bureau to all general hospitals and informed consent from each study participants.
Results
Background characteristics of respondents
A total of two hundred thirty three skilled attendants were included in the study, making a response rate of 100%. The mean age of the respondents was 30.2 year, with a standard deviation of (SD ± 6.6) years, of them 152(65.3%) were in the age group of 20-29. Majority of the respondents were female 141(60.5%). Among the respondents 193 (82.8%) were orthodox Christians and 154(66.1%) were midwives. Of the respondents 81(34.8%) of were diploma holder. From the total majority of them 151(64.8%) had less than 5 years’ experience (Table 1).
Table 1 Socio-demographic characteristic of skilled attendants working at labour wards in tigray region general hospitals, North Ethiopia, October 1-30, 2016 G.C (n=233).
| Characteristics |
Frequency |
Percent (%) |
| Age |
| 20-29 |
152 |
65.3 |
| 30-39 |
56 |
24 |
| ≥ 40 |
25 |
10.7 |
| Religion |
| Orthodox |
193 |
82.8 |
| Protestant |
21 |
9.1 |
| Muslim |
15 |
6.4 |
| Other * |
4 |
1.7 |
| Profession |
| Midwife |
154 |
66.1 |
| Medical doctor |
35 |
15 |
| IESO |
32 |
13.7 |
| Nurse |
12 |
5.2 |
| Highest qualification |
| Diploma |
81 |
34.8 |
| BSc |
68 |
29.2 |
| MSc intern |
51 |
21.9 |
| Intern doctor |
33 |
14.1 |
| Clinical experience |
| ≤ 5 |
151 |
64.8 |
| 6-9 |
39 |
16.7 |
| ≥ 10 |
43 |
18.5 |
Other* = catholic and seventh day Adventist
Knowledge on labour pain management method type and attitude of respondents
All respondents’ 233(100%) responds as they knew about managing labour pain in general, of them 113(48.5%) knows only non-pharmacologic labour pain management methods whereas 120(51.5%) knows both pharmacologic and nonpharmacologic labour pain management methods.
Of the pharmacologic methods, systemic opoids 119(51.1%), regional analgesia 114(48.9%), non-opoid systemic analgesia 95(40.8%) and inhalational 94(40.3%) of respondents knows this methods respectively.
On the other hand; the most known non-pharmacologic labour pain management method was massage the back by all 233(100%) of respondents (Table 2).
Table 2 Professionals knowledge of non-pharmacologic method types in all TRGH, North Ethiopia, October 1-30, 2016 G.C (n=233).
| Methods |
frequency |
percent (%) |
| TENS |
| Yes |
20 |
8.6 |
| No |
213 |
91.4 |
| Acupuncture |
| Yes |
35 |
15 |
| No |
198 |
85 |
| Massage the back |
| Yes |
233 |
100 |
| No |
0 |
0 |
| Psychotherapy |
| Yes |
232 |
99.6 |
| No |
1 |
0.4 |
| Show how to bear down |
| Yes |
229 |
98.3 |
| No |
4 |
1.7 |
| Allow companionship |
| Yes |
228 |
97.9 |
| No |
5 |
2.1 |
| Hot/cold pack immersion |
| Yes |
156 |
67 |
| No |
77 |
33 |
| Breathing technique |
| Yes |
196 |
84.1 |
| No |
37 |
15.9 |
| Hypnosis |
| Yes |
27 |
11.6 |
| No |
206 |
88.4 |
| Divertional therapy |
| Yes |
100 |
42.9 |
| No |
133 |
57.1 |
| Music therapy |
| Yes |
137 |
58.8 |
| No |
96 |
41.2 |
| Subcutaneous water injection |
| Yes |
43 |
18.5 |
| No |
190 |
81.5 |
In this study out of the total respondents 140(60.1%) of professionals had adequate knowledge on list of method type while the rest 93(39.9%) respondents had inadequate knowledge even from the listed method types.
Among the respondents who knew about pharmacologic labour pain management methods 98(80%) of them reported labour analgesia had side effect by delaying progress labour and 31(25.83%) of them reported fetal distress as a side effect of labour analgesia.
Among the respondents 101(43.3%) professionals had Negative attitude while the rest 132 (56.7%) of them had Positive attitude towards managing labour pain. Among the study participants 154(66.1%) of them believed as managing labour pain help the mother on labour, but only 58(24.9%) professionals perceive as every mother pain during labour should be managed. Among the skilled attendants 178(76.4%) of them believed that analgesia (pharmacologic method) is not necessary for managing labour pain. Of the respondents 217(93.1%) believed as labour pain is natural and the mother has to face it, but majority 177(76%) of them consider managing labour pain as their responsibility of care for laboring mother.
Personal preference and pain expectation
Among the study participants all of them, two hundred thirty three (100%) expectation of labour pain was labour pain as a severe pain. Most professionals 191(81.9%) prefer non- Pharmacologic methods to manage labour pain.
Practice of non-pharmacologic labour pain management methods
From the total of 233 skilled attendants working at all tigray region general hospitals 101(43.3%) of them practiced nonpharmacologic labour pain management methods. From the non-pharmacologic labour pain management methods, Show how to bear down was the most widely used method by 229(98.3%) professionals followed by psychotherapy 179(76.8%) and allow companionship 135(57.9%) (Figure 1).
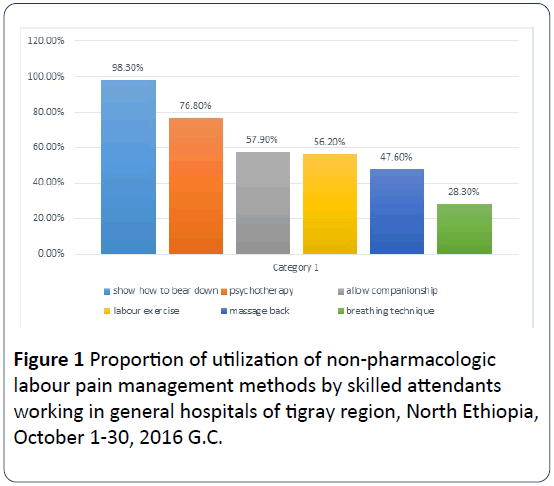
Figure 1: Proportion of utilization of non-pharmacologic labour pain management methods by skilled attendants working in general hospitals of tigray region, North Ethiopia, October 1-30, 2016 G.C.
Reason for non-utilization
The most common reasons mentioned by respondents for non-utilization of labour pain management were high patient flow by 233(100%) of respondents and small number of staff by 177(76%) of respondents (Figure 2).
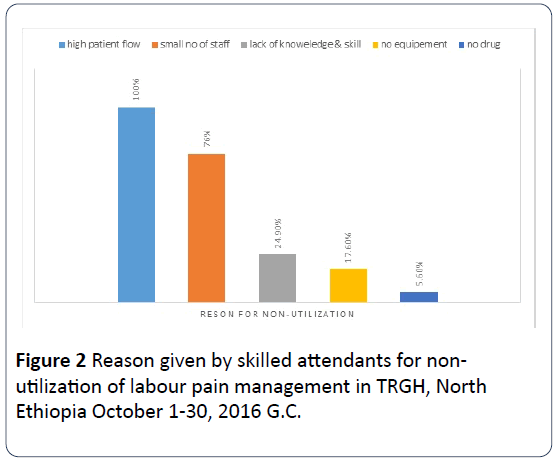
Figure 2: Reason given by skilled attendants for nonutilization of labour pain management in TRGH, North Ethiopia October 1-30, 2016 G.C.
Institutional factor
From the total respondents one hundred eighty one (77.7%) reported as allowing companion of choice it’s not allowed by their hospital and still all respondents didn’t gate any special training on managing labour pain. From the respondents who knows pharmacologic method type ninety six (80%) of them reported as Pethidine is available in their hospital.
Factor associated with practice of non-pharmacologic labour pain management methods: On the bivariate analysis professional age, level of knowledge, attitude, profession and professional’s highest qualification was identified to be significantly associated with current practice of labour pain management methods. But only attitude and highest qualification were remained significantly associated with current practice of non-pharmacologic labour pain management methods in the multiple logistic analysis.
The odds of current practice of non-pharmacologic labour pain management methods was higher among professionals who have positive attitude for managing labour pain. Skilled attendants who have positive attitude for managing labour pain were about 2.24 times more likely to practice nonpharmacologic labour pain management methods as compared to those professionals who have negative attitude for labour pain management {AOR=2.242, 95% CI= (1.242-4.048)}.
Professionals who had highest qualification of MSc (high level qualification) were 2.876 times more likely to practice non-pharmacologic labour pain management methods than professionals who had lower level qualification of diploma. {(AOR=2.876, 95% CI = (1.29-6.39)} (Table 3).
Table 3 Bivariate and multivariate analysis of factors associated with practice of non-pharmacologic labour pain management methods in TRGH, North Ethiopia, 2016.
| |
Practice of non-pharmacologic labour pain management method |
COR (95% CI) |
AOR (95%CI) |
| |
Yes |
No |
|
|
| Frequency (n) |
Frequency (n) |
| Age |
| 20-29 |
70 |
82 |
2.70(1.02-7.14) |
2.25(0.74-6.83) |
| 30-39 |
25 |
31 |
2.55(0.88-7.36) |
1.37(0.44-4.26) |
| ≥ 40 |
6 |
19 |
1 |
1 |
| Qualification |
| Lower level |
26 |
55 |
1 |
1 |
| Medium level |
41 |
60 |
1.45(0.78-2.66) |
1.28(0.68-2.40) |
| Higher level |
34 |
17 |
4.23(2.01-8.92) |
2.87(1.29-6.39)** |
| Attitude |
| Positive Negative |
72 |
60 |
2.98(1.72-5.17) |
2.24(1.24-4.05)** |
| |
29 |
72 |
1 |
1 |
| Knowledge |
| Adequate |
73 |
67 |
2.53(1.45-4.34) |
1.34(0.67-2.67) |
| Inadequate |
28 |
65 |
1 |
1 |
| Profession |
| Midwife |
59 |
95 |
0.55(0.31-0.95) |
0.96(0.51-1.81) |
| Other |
42 |
37 |
1 |
1 |
**= significant variable in backward stepwise logistic regression
Lower level: diploma, Mid-level: BSc and medical intern, Higher level: MSc
Other: Nurse, Medical intern, IESO
Discussion
There is no doubt that provision of pain relief services in labour would add value to obstetric services, managing labour pain is not luxury rather anticipated obstetrics care [11]. This institutional based cross sectional study has attempted to determine utilization of labour pain management methods and associated factors by skilled attendants working in tigray region general hospitals at labour ward, North Ethiopia.
Childbirth is one of the most painful events that a woman is likely to experience, the multidimensional aspects and intensity of labour pain is not comparable with other circumstances, but majority of the respondents in this study 178(76.4%) of them believed that analgesia (pharmacologic method) is not necessary for managing labour pain, which is unlike the study in Zaria, Nigeria. There 94.8% of health care provider agreed that labour analgesia is needed during labor [11]. The possible reason for this difference might be the awareness of pharmacologic agents used to relieve pain during labor by health care provider in Zaria, Nigeria was high as compared with this study, which is observed by the attitude difference between these two populations.
The current study found out that the proportion of skilled attendants utilizing non-pharmacologic labour pain management methods were 43.3%. This study finding is in line with the study done in Bangladesh; there utilization of nonpharmacologic labour pain management was 40%. But specific to each method utilization, in this study utilization of nonpharmacologic labour pain management methods was lower than Bangladesh. While comparing utilization in Tigray, Ethiopia versus Bangladesh, labour exercise 56.2% versus 78.4%, massage the back 47.6% versus 53.6%, breathing technique 28.3% versus 40.2% and allow companionship 57.9% versus 77.3% of respondents’ utilization. But higher than Bangladesh by showing the mother how to bear down 98.3% versus 72.2% of respondents utilization [5]. This difference is expected difference from place to place because health professionals couldn’t be identical in every aspect from one site to another.
Regarding pharmacologic labour pain management this study found out proportion of skilled attendants utilizing pharmacological labour pain management methods was zero, the finding of this study is in line with a study done in Amhara region referral hospital which was zero [10]. But this study finding is much lower as compared to other studies like obstetric analgesia utilization in Addis Ababa, Ethiopia (54.2%) [12], epidural obstetric analgesia use in France (75%), Sweden (71%), Bangladesh (58.5%) [5], Colombia (31.5%) and South Africa (49%) [9]. Even in Nigeria 49% of obstetricians offered obstetric analgesia of which the commonest analgesia was opioids (41.1%)(13). And 27% of mothers in Canada received the commonest (92.6%) IM Pentazocine Hydrochloride for labour pain relief [13,14]. The possible reason for this incomparable difference is this study was conducted in tigray region general hospitals, they are found in rural area they are far from the capital Addis Ababa, but in other countries the hospitals are modern and all equipment’s and drugs for labour analgesia are available in those modern setup. And the other possible reason is vast majority of the respondent’s here are diploma holder and even they didn’t have adequate knowledge about pharmacologic labour analgesia and the other reason might be negative attitude towards utilization of labour analgesia.
This study also revealed those skilled attendants who have positive attitude for managing labour pain were 2.24 times more likely to use labour pain management method than skilled attendants who have negative attitude. {AOR(95%CI)=2.24(1.24-4.05)} which is consistent with a study in Bangladesh, which reported negative attitude of health care providers were restrictive towards utilization of analgesic for normal labour, and they also thought it would interfere with normal progress of labour. However, they expressed positive attitude to help mothers to cope with labour pain through assurance and carry out some activities to comfort the women in labour [5].
In this study highest qualification was statistically significant predictor of utilization of labour pain management methods. Skilled attendants who were MSc intern (higher level qualification) were 2.87 times more likely to use labour pain management methods than professionals who had diploma (low level qualification). {AOR (95%CI)=2.87(1.29-6.39)}.
This finding is opposite with study done in Amhara regional state referral hospitals which reported Obstetric care givers who had diploma (low level qualification) were 2.69 times more likely to use obstetric analgesia methods than professionals who had second degree (high level qualification) {AOR(95%CI)=2.69(1.13-6.41)} [10].
The possible explanation for this difference might be in this study professionals who have higher level qualification are MSc interns, since they are students so their evaluation also depend on their management skill and client professionals’ relationship, so this implication is reflected by their utilization of labour pain management methods.
In this study professionals reason for not using labour pain management method were; high patient flow, small number of staff, lack of knowledge and skill and unavailability of equipment’s and drugs for managing labour pain. The finding is consistent with a study done at public hospitals of Addis Ababa Ethiopia [12].
Limitation and Strength of the Study
Limitation of the study
In this study head nurses were recruited as a data collector which has social desirability bias.
Strength of the study
In this study census was employed to recruit study participants, which eliminate sampling error.
Conclusion
Even though managing labour pain is anticipated obstetrics care, this study revealed poor practice of non-pharmacologic labour pain management methods. The major predictor for practice of non-pharmacologic labour pain management methods as per this study finding was professionals’ positive attitude towards managing labour pain and highest qualification.
In a setup like us with high patient flow practicing methods for managing labour pain was considered as luxury rather than anticipated obstetrics care, as a result high patient flow was the number one listed reason for non-practicing of labour pain management methods.
Recommendation
Federal ministry of health and TRHB
To incorporate education of pharmacologic and nonpharmacologic labour pain management methods in the curriculum at all level of qualification including diploma program.
Tigray region general hospitals
An institutional framework that includes education and supply of required equipment will help care providers to bridge the gap between their attitudes and provision of pain relief services in labor.
Non-governmental organization
To participate in education, positive attitude creation and information regarding benefits of managing labour pain and strengthen short term trainings on issues related to labour pain and obstetric analgesia.
Researcher
A qualitative study needs to be done on utilization of labour pain management methods from mothers’ satisfaction point of view.
20128
References
- Beigi NM, Broumandfar K, Bahadoran P, Abedi HA (2010) Women's experience of pain during childbirth. Iran J Nurs Midwifery Res 15: 77-82.
- Eisenach JC, Pan P, Smiley RM, Lavand'homme P, Landau R, et al. (2013) Resolution of pain after childbirth. Anesthesiology 118: 143-151.
- Soet JE, Brack GA, DiIorio C (2013) Prevalence and predictors of women's experience of psychological trauma during childbirth. Birth (Berkeley, Calif) 30: 36-46.
- Tasnim DS (2010) Perception about pain relief during normal labour among health care providers conducting delivery. Medcine today 22: 20-23.
- Bonnet MP, Prunet C, Baillard C, Kpea L, Blondel B, et al. (2017) Anesthetic and obstetrical factors associated with the effectiveness of epidural analgesia for labor pain relief: An observational population-based study. Reg Anesth Pain Med 42: 109-116.
- Klein MC, Grzybowski S, Harris S, Liston R, Spence A, et al. (2001) Epidural analgesia use as a marker for physician approach to birth: Implications for maternal and newborn outcomes. Birth (Berkeley, Calif) 28: 243-248.
- Mugambe JMNM, Hiemstra LA, Steinberg WJ (2007) Knowledge of and attitude towards pain relief during labour of women attending the antenatal clinic of Cecilia Makiwane Hospital, South Africa. Medpharm 49: 16-20.
- Ortiz GD, Navarro-Vargas JR, Eslava-Schmalbach J (2013) Inequity in healthcare-the outlook for obstetric analgesia. Colombian J Anesthisology 41: 5-7.
- Bitew AWA, Seyum T (2016) Utilization of obstetric analgesia in labor pain management and associated factors. J Biomedical Sci 5: 1-6.
- Ogboli-Nwasor E, Adaji S, Bature S, Shittu O (2011) Pain relief in labor: A survey of awareness, attitude, and practice of health care providers in Zaria, Nigeria. J Pain Res 4: 227-232.
- Mulugeta H (2016) The practice of labor analgesia and its perceived barriers among health care providers working in public hospitals of Addis Ababa, Ethiopia.
- Lawani JNELO, Okechukwu BA, Iyoke CA, Ekem NN (2014) Obstetric analgesia for vaginal birth in contemporary obstetrics: A survey of the practice of obstetricians in Nigeria. BMC 14: 1-6.
- Likis FE, Andrews JC, Collins MR, Lewis RM, Seroogy JJ, et al. (2014) Nitrous oxide for the management of labor pain: A systematic review. Anesth Analg 118: 153-167.

