Keywords
Transcultural nursing; Self-efficacy; Education
Introduction
The quality of nursing care can be improved significantly when nurses engage closely with patient-centered care considering the cultural context. Transcultural Self-efficacy (TSE) is a major influencing factor that aims to achieve cultural competence towards the cultural congruent care [1]. To meet the comprehensive nursing care of multicultural populations, all nursing students and nurses should be competent in cultural sensitivity care through formalized educational experiences [1]. Nurse educators continuously investigate the cultural competency outcomes for nursing students to meet the universal standards of practice guide for culturally competent care to be used in clinical practice, research, education, and administration [2,3]. Interventions on TSE require addressing social justice, transcultural nursing knowledge, education and training, cross-cultural leadership, cross-cultural communication and cross-cultural practice.
Perception of self-efficacy determines the accomplishment of knowledge in which transcultural nursing skills in relation to emotion regulation [1], procedural self-efficacy, support request, cultural motivation and interpersonal communication skills [4-6]. Emotional regulation is the results of the intrinsic and extrinsic process that influencing in observing, evaluating, controlling emotional responses [4,5]. Procedural selfefficacies is defined as the ability to handle the various dimensions of the social work practice, such as performing a fair and affectionate relationship with the client; support request concerns the confidence in the ability to expect and find support in others such as other professionals, superiors and colleagues [4]. Cultural motivation defined as the psychological processes that determine the direction, intensity, and persistence of action in a cultural context [6].
Moving forward in the 21st century, nursing education is not only for preparing nurses for cultural congruent nursing care but also preparing nurses for advancing professional development through nurses’ higher education. The trend is moving students from developing countries to developed countries to achieve their higher education expectations such as Master or Doctor of philosophy in nursing. Therefore, the students who have TSE might be more competent in nursing care for the multicultural community and adjust for the new cultural society where the potential to obtain higher education opportunities reducing acculturation stress.
Among the developing countries, Sri Lanka is a multicultural country, which importantly required cultural congruent care and there are no opportunities for transcultural nursing education to date. In addition, with the accelerating of present professional development, there is a new trend to move to developed countries for higher education. Hence, developing TSE in nursing students is an essential aspect which might be the wide influence in the future of nursing education system in Sri Lanka.
Theoretical approach
Five environmental systems appeared in ecological systems theory which was developed by Urie Bronfenbrenner for the purpose of examining the relationships of individuals within the community [7]. According to this model, individual (ontogenic) is the innermost level which describes one’s sex, age, health etc. Next level is microsystem which consists of institutions, organizations, and groups directly impact the one's development through family, educational institutions, religious organizations, neighbor and peers. Mesosystem indicates the interconnections between the microsystems, interactions between the family and teachers, the relationship between the one’s peers and the family. Exosystem creates links between social environments; results in one’s experience may be influenced by other’s experience at work. Macrosystem is the external level that involves the culture where individuals in which include socioeconomic status, religion and ethnicity. In this study, factors to be examined placed into four levels; ontogenic, microsystem, exosystem and macrosystem (Figure 1).
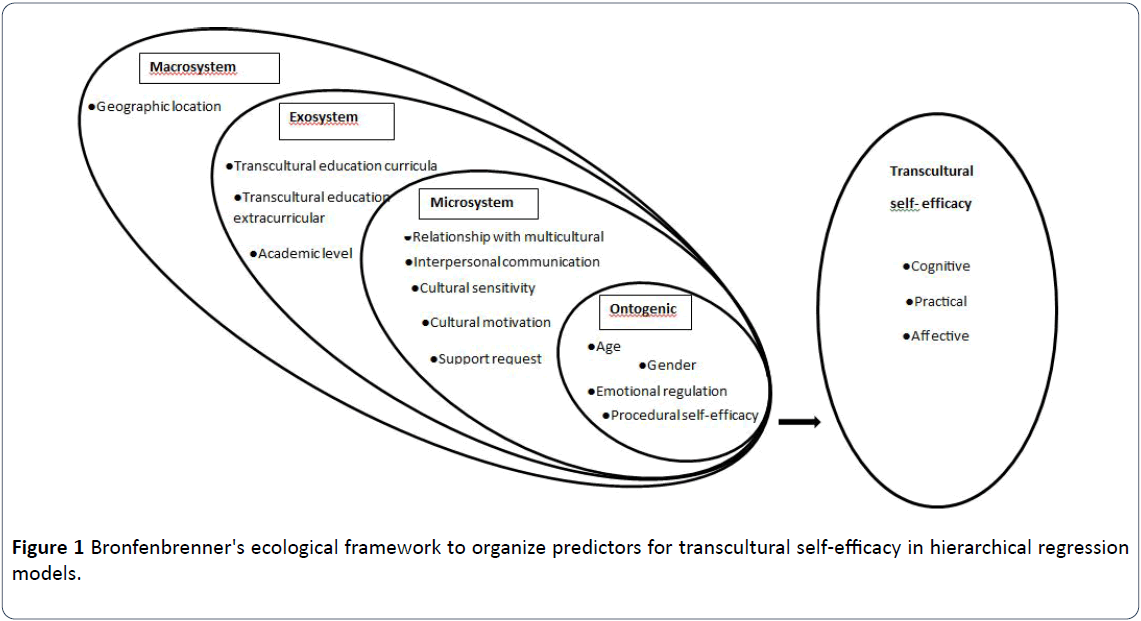
Figure 1: Bronfenbrenner's ecological framework to organize predictors for transcultural self-efficacy in hierarchical regression models.
Applying this theoretical framework, this analysis aimed to identify the significant factors for TSE which finding might be leading for developing education intervention in transcultural nursing. The objectives were to identify the degrees of three domains; cognitive, practical and affective of TSE, find the significant differences between demographic factors and TSE, the relationship among variables and explore the predictors for the TSE of nursing students according to the levels of the ecological model.
Methods
Design and sample
This was a cross-sectional, quantitative correlational design with secondary data analysis using hierarchical regression models to evaluate previously collected data from 145 nursing students in two nursing schools offering 3 years diploma in nursing in Sri Lanka during August in 2016. To select the subjects, the convenience sampling method was used. The total sample comprised second and third year of the study, 150 students consented to participate by completing questionnaires response rating of 96.6%. Of them, five questionnaires discarded due to uncompleted filling, 145 were selected for analysis.
Instruments
Data were collected using a self-administered questionnaire, consisted of a demographic questionnaire, Transcultural Selfefficacy Tool (TSET), social self-efficacy scale, cultural motivation subscale of cultural intelligence, interpersonal communication skills subscale of self- directed learning, cultural sensitivity subscale of cultural competence scale.
To measure the TSE, TSET designed and tested by Jeffreys et al. in 2010 consists of 83 items [1]. The total scale score is between 83 and 830 in 3 subscales: cognitive, practical and affective; a score greater than 600 indicate the acceptable level of self-efficacy for TCSE. Alpha coefficients were for cognitive 0.96 related to their knowledge of cultural factors that influence nursing care among culturally diverse groups; practical 0.97 related to interviewing culturally diverse clients about their beliefs and values; affective 0.96 related to values, attitudes and beliefs concerning cultural awareness, acceptance, appreciation, recognition and advocacy.
Emotional regulation, procedural self-efficacy and support request were measured by using self-efficacy scale for social workers developed by Monica et al. in 2013 [4]. Cronbach’s alphas for emotional regulation, procedural self-efficacy, and support request were 0.81, 0.76 and 0.80 respectively [4]. Cultural motivation was measured by, five items subscale; motivational factor in Cultural Intelligent Scale (CQS) developed by Ang et al. in 2007 [8]. Motivational factor indicated the Cronbach’s alphas, 0.75 and the total score was 35. Interpersonal communication skills was measured by using 5 items subscale of Self-Directed Learning Instrument (SDLI) for nursing students which was developed by Shen et al. in 2014 [9]. Cronbach’s alpha was 0.75 for interpersonal communication skills. Cultural sensitivity was measured by using cultural sensitivity subscale of cultural competence scale for nursing students developed by Han et al. in 2015 [10]. Cronbach’s alpha was 0.76 for cultural sensitivity.
Data collection
The ethical review committee of the Inje University approved this research and ministry of Sri Lanka granted permission for collecting data (No. 2015349-04, April 7, 2016). The settings were two nursing schools in the urban area and rural area in Sri Lanka. To recruit the participants, the convenience sampling method was used. There were 75 subjects selected in each nursing school and in second year 37 and the third year 38 subjects were selected. All participant were recruited after giving information about the study and after collecting their inform consent. Data collection was done by using self- administered questionnaire in a separate place in the school during August in 2016. The questionnaire was prepared in English because their course is in English medium. The students who could understand the questionnaire in English were included in this study. The average time was about 30 minutes to complete the questionnaire.
Data analysis
To analyze the data, Statistical Package for the Social Science (IBM SPSS) version 25.0 software was used. Frequencies were obtained and percentages were used to describe the demographic characteristics. The degree of the subscales of transcultural self-efficacy tool was described using means and standard deviations. To describe the associations between demographic characteristics of nursing students and TSE, ttests and F-tests were used. The relationship between ecological factors and TSE was assessed using Pearson correlation coefficient analysis. All the statistical inferential tests were assessed according to the significant level p<0.05. The predictors for TSE were identified by hierarchical regression analysis.
Results
Demographic characteristics
Demographic characteristics indicated the nursing students were 71 (49%) from the nursing school in the rural area and 74 (51%) in the urban area of total 145 students. There were 49.7% in the second year and 51.0% in the third year of the total. The age ranges, 40.7% were in 21 to 24 years and 59.3% were in 25 to 28 years, the mean age of the participants was 24.75. The majority (93.1%) were female; in religion, (98.6%) were Buddhist. Of these, 86.9% of students have participated in transcultural curriculum activities and 20.7% to transcultural extra curriculum activities.
Degree of transcultural self-efficacy
The findings of this analysis showed that the overall high score of TSE (m=6.89 (1.09)) in nursing students in Sri Lanka. Furthermore, highest score reported for cognitive subscale (m=7.26 (1.29), than the subscales practical (m=6.93 (1.35)) and affective (m=6.82 (1.15)). Comparing two groups which an urban and rural area, students of the school located in the urban area showed the significant higher transcultural selfefficacy for all subscale than the students who were in the rural area (Table 1).
Table 1 Degrees of transcultural self-efficacy related to three subscales.
| Subscale |
Urban |
Rural |
p |
| Cognitive |
7.62 (1.14) |
6.89 (1.35) |
0.001 |
| Practical |
7.29 (1.16) |
6.55 (1.43) |
0.001 |
| Affective |
7.15 (1.19) |
6.48 (1.00) |
0 |
| Overall transcultural self-efficacy |
7.24 (.99) |
6.52 (1.07) |
0 |
Note: p<0.05
Demographic characteristics according to transcultural self-efficacy
Demographic factors; geographic location, age, gender and relationship with multicultural groups were significantly associated with TSE. TSE (t=14.18, p<0.001) of nursing students in nursing school in urban area is higher (7.24 (0.99)) than rural area (6.52 (1.07)). Statistically significant differences were according to the geographical location; urban and rural area of studies for every subscales; cognitive subscale (p=0.001), practical subscale (p=0.001) and affective subscale (p<0.001) showed in Table 1, exhibiting higher score in school in urban area than rural. The age group 21 to 24 showed (t=2.72, p=0.007) higher confidence (7.18 (0.91)) than the age group 25 to 28 (6.69 (1.16)). Gender was significantly related with TSE (t=-2.04, p=0.040) female students (6.52 (1.07)) demonstrated higher score compared with male (6.52 (1.07)). Relationship with multicultural groups significantly associated with TSE (t=2.81, p=0.009) indicating higher score in the students with relationship with multicultural groups (6.98 (1.04)) than those who were not (6.24 (1.20)).
Relationships among variables
Considering TSE and other related variables, the highest level of positive relationship showed TSE and interpersonal communication (r=0.39 (p<0.001)). There were significant positive relationship between TSE and cultural sensitivity (r=0.37 (p<0.001)), emotional regulation (r=0.35 (p<0.001)), cultural motivation (r=0.31 (p<0.001)) and perceived selfefficacy (r=0.22 (p<0.006)). In addition, among all variables, procedural self-efficacy exhibited the strong correlation with support request (r=0.53 (p<0.001)) and emotional regulation (r=0.46 (p<0.001)) (Figure 2). Moreover, significant relationships showed between cultural motivation and emotional regulation (r=0.19 (p=0.020)), interpersonal communication (r=0.28 (p=0.001)), cultural sensitivity (r=0.16 (p=0.042); cultural sensitivity with interpersonal communication (r=0.23 (p=0.005)) positively.
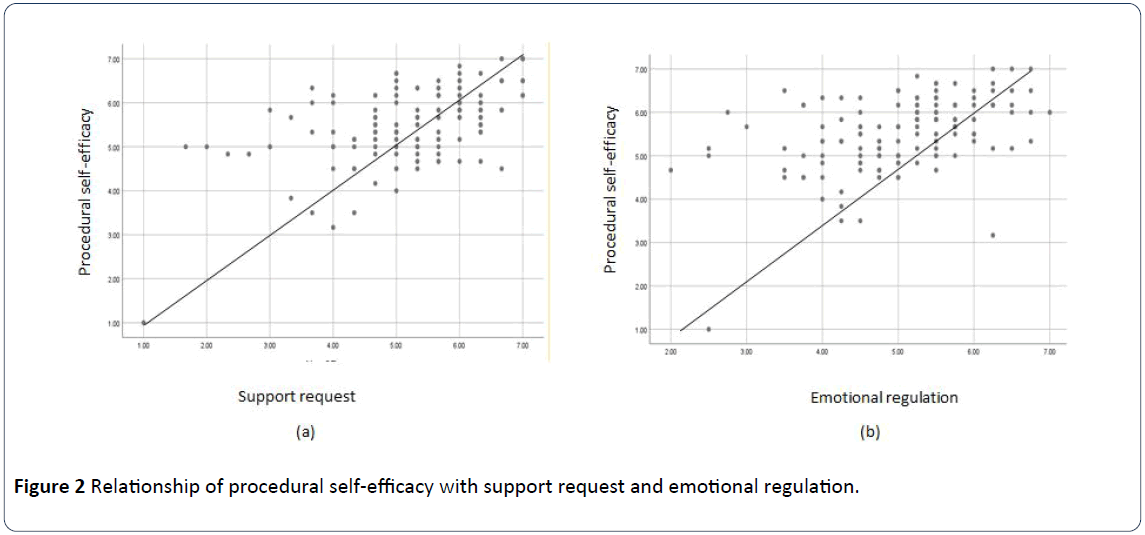
Figure 2: Relationship of procedural self-efficacy with support request and emotional regulation.
Predictors for transcultural self-efficacy
The hierarchical linear regression model tested the macro, exo, microsystem and ontogenic factors to contribute to TSE. The four-level model of factors was associated with 41% of the variation in transcultural self-efficacy (F=7.08, df 144, p<0.001). Geographic location (t=2.89, df 144, p=0.004), cultural sensitivity (t=3.06, df 144, p=0.003), interpersonal communication skills (t=-2.39 df 144, p=0.022) and emotional regulation (t=2.30, df 144, p=0.023) were the predictors for TSE (Table 2).
Table 2 Predictors for the transcultural self-efficacy.
| Predictors |
Model 1 Macrosystem |
Model 2 Exosystem |
Model 3 Microsystem |
Model 4 Ontogenic |
| Macrosystem |
β |
SE |
β |
SE |
β |
SE |
β |
SE |
| Geographic location |
0.331*** |
0.172 |
0.437*** |
0.185 |
0.293*** |
0.174 |
0.241** |
0.182 |
| Exosystem |
| Transcultural education curricula |
|
|
0.184* |
0.263 |
0.089 |
0.245 |
0.074 |
0.239 |
| Transcultural education extracurricula |
|
|
-0.205* |
0.238 |
-0.160* |
0.217 |
-0.104 |
0.218 |
| Academic level |
|
|
-0.169* |
0.18 |
-0.096 |
0.171 |
-0.123 |
0.167 |
| Microsystem |
| Relation with multicultural groups |
|
|
|
|
-0.096 |
0.24 |
-0.108 |
0.238 |
| Interpersonal communication skills |
|
|
|
|
0.252** |
0.13 |
0.176* |
0.133 |
| Cultural sensitivity |
|
|
|
|
0.236** |
0.14 |
0.220** |
0.136 |
| Cultural motivation |
|
|
|
|
0.099 |
0.105 |
0.068 |
0.104 |
| Support request |
|
|
|
|
-0.038 |
0.024 |
-0.133 |
0.027 |
| Ontogenic |
| Age |
|
|
|
|
|
|
-0.109 |
0.159 |
| Gender |
|
|
|
|
|
|
0.063 |
0.312 |
| Emotional regulation |
|
|
|
|
|
|
0.203* |
0.117 |
| Procedural self-efficacy |
|
|
|
|
|
|
0.079 |
0.105 |
| R2 |
0.109*** |
|
0.179*** |
|
0.353*** |
|
0.413*** |
|
| ΔR2 |
0.103 |
|
0.155 |
|
0.31 |
|
0.354 |
|
Note. SE, standard error, Values -0.00 or 0.00 indicate -0.01< β <0.01,
*p<0.05, **p<0.01, ***p<0.001
Discussion
Nurses are the professionals that interact with the people with differences in ethnicity, religion, gender, age, physical and psychological disabilities, language barriers, geographical location, and socioeconomic status to deliver health care on a holistic approach [11,12]. With the growth of culturally diverse population, it is recommended to be national strategies in relation to the cultural needs of the patients or a client reducing health disparities [11]. Therefore, today, transcultural nursing is an influential facet of healthcare because nurses require recognizing and appreciating values, beliefs, and customs in cultural diversity populations indicating TSE is a significant factor towards the cultural congruent care. The findings of this work indicated that overall higher score of TSE in nursing students in Sri Lanka for three subscales; cognitive, practical and affective. A previous study showed that moderate level of transcultural self-efficacy of nurses who works in a hospital in China on the Cognitive (87.9%), Practical (87%) and Affective (89.2%) TSET subscales [13].
Statistically significant differences were according to the geographical location, age group, gender and relationship between multicultural groups in this study. Students were in school in the urban area showed a higher score than students were in school in the rural area making the geographical location of studies a characteristic that was found to be statistically important. There subscales; cognitive, practical and affective were in the higher level of confidence of school in the urban area than the rural area. This was supported with the finding of Franklin, [14] which was conducted as the first study in different institutional settings in 2015 indicating statistically significant differences found in the affective subscale where there were no significant differences between the two groups in the cognitive or practical subscales. This difference in the present study because nursing students in urban area nursing school received additional cultural education program experience as a benefit to the students who participated and their clinical education in nursing under the hospital where more multicultural patients were occupied. The previous studies provide evidence of the benefit of transcultural experience in clinical setting to increase students’ TSE scoring higher level of cognitive subscale [15], TSE positively correlated with English language proficiency, degrees of interest in multi-culture, degree of experience in caring for multi-cultural clients and educational needs for cultural competent care [16].
There were no significant differences between the academic levels in this work, although a higher mean score for three subscales for TSE was for senior students than for freshmen students of study in Greek University [17], and furthermore, the findings of a previous study showed that fourth-year nursing students at a Western Australian University portrayed a higher perception of self-efficacy than first-year nursing students in performing transcultural nursing skills [18]. There were significant differences found for the cognitive subscale by class rank [15]. This result was supported by the study which conducted at the University of South Dakota in Guatemala for the students of inter professional teams regarding servicelearning experience [19]. The present study showed significant differences in the overall confidence score in age groups; youngest age group (21-24) had significantly high scores than the students’ ages of 25 to 28 years. By contrast, that nurses are in the age of 25 years exhibited the lower scores than the nurses are in the age group between 30 to 35 or more than 35 in China [13].
Statistically, the significant difference was between male and female respondents in the present study. This evidence supported by the research of Herrero-Hahn et al. [20]. However, a study of baccalaureate nursing students in the Midwest revealed that there are no significant differences in gender and age in relation to TSE [1,13,15]. In addition, a previous study revealed that age and gender did not influence the nursing students' perception of self-efficacy in performing transcultural care [19]. In this work, nursing students who had a relationship with multicultural groups portrayed the higher self-efficacy than those were not interacting with the multicultural group. This result was supported by the previous studies revealing that students who had opportunities to interact with the patients or clients demonstrated the high confidence than the student who had not similar experience related to the culture [21]. Findings from the current study were also persistent with several other pieces of research that have demonstrated that clinical experience and appropriate education is an important approach in enhancing the clinical confidence in nurses. Hierarchical regression results showed the predictors for the TSE in nursing students in Sri Lanka under the category of macrosystem (geographical location), microsystem (interpersonal communication, cultural sensitivity) and ontogenic (emotional regulation).
It is stated that developing culturally sensitive is essential to facilitate positive interaction with the clients and the inter professional in multicultural view [19]. With the evaluation of interventions, previous researches suggested to improving the interpersonal communication skills through the transcultural educational interventions towards the improving ability to provide culturally competent care [21]. Supporting this viewpoint, the current study provides the evidence; interpersonal communication is the predicted variable for TSE. Geographic location where diverse population living is energizing the attitudes of interacting with multicultural groups in the nursing students. The studies undertaken in selfregulation have highlighted that regulating emotions of nursing students increase their self-confidence on nursing care because emotional self-control makes the nurse flexible and display empathy with others, therefore can respond to every people without taking over their self-emotions [22,23].
According to the regression analysis results, it is assumed that cultural motivation and transcultural education extra curricula have a mediating effect on TSE. The nursing education system in Sri Lanka has been remarkably reformed from last few years. Although the minimum level of attention is in the area of transcultural nursing in nursing education in Sri Lanka, even multicultural population continuously growing up. To introduce the concept of “transcultural nursing” in the nursing curricula is justifiable approach and contributing research in this area would be great to make strategies related to cultural congruent care towards the enhancing quality of health service. Not surprisingly, institutions have emphasized the necessity for healthcare professionals to improve and maintain knowledge, skills, and attitudes consistent with confidence in culturally appropriate care. Therefore, this work is one of the efforts to understand the level of TSE and explore the contributing factors of nursing students to develop the cultural competence education programs in Sri Lanka.
Conclusion
This analysis explored the archeological factors according to the four system levels appeared to influence their confidence on the transcultural knowledge, skills, and attitudes. The nursing students in both urban and rural school have acceptable levels of TSE, although showing urban area school students have confidence higher than rural requiring nurse educators to adopt teaching strategies that optimize their confidence with more multicultural experience opportunities with a multicultural community. According to the findings, macro and microsystem and ontogenic factors emphasize the needs of developing knowledge, skills and most importantly attitudes towards the social justice, interacting with every people with no bias on their race, religion, social status controlling their self-emotions, and being empathy.
24082
References
- Brusic V, Rudy G, Honeyman G, Hammer J, Harrison L (1998) Prediction of MHC class II- binding peptides using an evolutionary algorithm and artificial neural network. Bioinformatics 14: 121-130.
- Jeffreys MR, Dogan E (2010) Factor analysis of the transcultural self-efficacy tool (TSET). J Nurs Meas 18: 120-139.
- Douglas MK, Pierce JU, Rosenkoetter M, Callister LC, Hattar-Pollara M, et al. (2009) Standards of practice for culturally competent nursing care: a request for comments. J Transcult Nurs 20: 257-269.
- Li J, He Z, Luo Y, Zhang R (2016) Perceived transcultural self-efficacy of nurses in general hospitals in guangzhou, China. Nurs Res 65: 371-379.
- Pedrazza M, Trifiletti E, Berlanda S, Bernardo GAD (2013) Self-Efficacy in social work: development and initial validation of the self-efficacy scale for social workers. Soc Sci 2: 191-207.
- Kraaij V, Garnefski N (2019) The behavioral emotion regulation questionnaire: development, psychometric properties and relationships with emotional problems and the cognitive emotion regulation questionnaire. Pers Individ Differ 137: 56-61.
- Chen G, Kirkman BL, Kim K, Farh CIC (2010) When does cross-cultural motivation enhance expatriate effectiveness? A multilevel investigation of the moderating roles of subsidiary support and cultural distance. Acad Manag J 53: 1110-1130.
- Bronfenbrenner U (1979) The ecology of human development: experiments by nature and design. USA: Harvard University Press.
- Linn V, Soon A (2007) Development and validation of the CQS the cultural intelligent scale.
- Shen W, Chen H, Hu Y (2014) The validity and reliability of the self-directed learning instrument (SDLI) in mainland Chinese nursing students. BMC Medical Educ 14: 108.
- Han SY, Cho CH (2015) Development of a cultural competence scale for nursing students. J Korean Acad Nurs 45: 684-693.
- Cupelli L (2016) An innovative service-learning project to develop cultural competency in undergraduate nursing students. Teaching and Learning in Nursing 11: 113-117.
- Prosen M (2015) Introducing transcultural nursing education: implementation of transcultural nursing in the postgraduate nursing curriculum. Procedia-Social and Behavioral Sci 174: 149-155.
- Li J, Zhuang He, Luo Y, Zhang R (2016) Perceived transcultural self-efficacy of nurses in general hospitals in Guangzhou, China. Nurs Res 65: 371-379.
- Franklin WJ (2015) Transcultural self-efficacy perceptions in nursing students in private and public higher educational groups. Transcultural self-efficacy perceptions in nursing students in private and public higher educational groups. Sigma theta Tau International Honor Society of Nursing. (43rd Biennial Convention conference).
- Halter M, Grund F, Fridline M, See S, Young L, et al. (2015) Transcultural self-efficacy perceptions of baccalaureate nursing students. J Transcult Nurs 26: 327-335.
- Kim SH (2013) Transcultural self-efficacy and educational needs for cultural competence in nursing of Korean nurses. J Korean Acad Nurs 43: 102-113.
- Sarafis PA, Malliarou MM (2013) Cultural self-efficacy of baccalaureate nursing students in a Greek University. Iran J Nurs Midwifery Res 18: 446-450.
- Lim J, Downie J, Nathan P (2004) Nursing students’ self-efficacy in providing transcultural care. Nurse Education Today 24: 428-434.
- Cerny SL, Svien L, Johnson J, Hansmeier B (2018) Using international, interprofessional service learning to promote transcultural self-efficacy and interprofessional attitudes in health science students. JOTE 2: 1-20.
- Herrero-Hahn R, Rojas JG, Montoya-Juarez R, Garcia-Caro MP, Hueso-Montoro C (2018) Level of cultural self-efficacy of Colombian nursing professionals and related factors. J Transcult Nurs.
- Larsen R, Reif L (2011) Effectiveness of cultural immersion and culture classes for enhancing nursing students' transcultural self-efficacy. J Nurs Educ 50: 350-354.
- Fernandez R, Salamonson Y, Griffiths R (2012) Emotional intelligence as a predictor of academic performance in first year accelerated graduate entry nursing students. JCN 21: 3485-3492.

