Porta-Etessam J1,2*, García-Ramos R2, Ruiz-Giménez J3, Moreno T3, Ruiz-Morales-J3
1Headache and Neuroophthalmology Unit.
2Neurology Department. Hospital Universitario Clínico San Carlos
3Neurology department. Hospital Universitario “12 de octubre”. Madrid. Spain.
*Corresponding Author:
Jesús Porta-Etessam MD C
Andrés Torrejón, 15, 7º. 28014 Madrid Spain.
E-mail: jporta@yahoo.com
Pretectal syndrome refers to a complex clÃnical elements andsymptoms secundary to damage of the pretectum structures.The two most important pretectal areas are the rostral intersticialnucleus of the medial longitudinal fasciculus (riRLF) and interstitialnucleus of Cajal. This syndrome is highlighted by supranuclearvertical upgaze paresis, pupillary, eyelid and convergegenceretraction nystagmus1,2. We report a 35-years-old womanwho present pretectal syndrome due to a multiple sclerosis.
Pretectal syndrome refers to a complex clínical elements and symptoms secundary to damage of the pretectum structures. The two most important pretectal areas are the rostral intersticial nucleus of the medial longitudinal fasciculus (riRLF) and interstitial nucleus of Cajal. This syndrome is highlighted by supranuclear vertical upgaze paresis, pupillary, eyelid and convergegence retraction nystagmus[1,2]. We report a 35-years-old woman who present pretectal syndrome due to a multiple sclerosis.
She complains about diplopia and blurred vision at near. General examination was normal and on neurological examination, she showed supranuclear gaze restriction affecting both vertical saccades and pursuit, but the saccades deficit was more prominent. When she attempted upwards saccades the eyes jerk inward and the left eye had an abduction deficit which easily overcome by horizontal oculocephalic movements (fig 1-3). There was no pupillary anormalities, lid retraction or convergence insufficience.
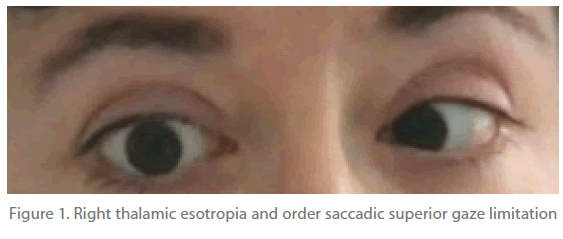
Figure 1. Right thalamic esotropia and order saccadic superior gaze limitation
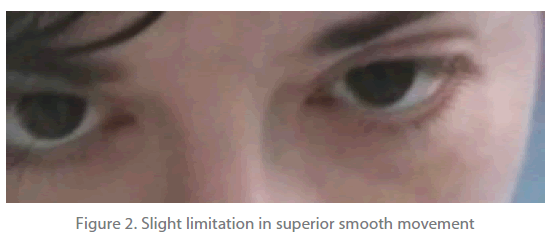
Figure 2. Slight limitation in superior smooth movement
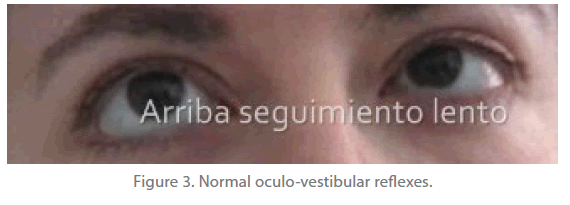
Figure 3. Normal oculo-vestibular reflexes.
A cranial CT scan revealed no abnormality. An oligoclonal band was detected in CSF. An MRI using General Electric revealed an abnormal high signal intensity lesion on T2-weigted imaginng at the ventral area of the midbrain aqueduct whith gadoliniumenhanced ,another small lesion in the temporal white matter on the left and T2-hyperintense lesion traversing the corpus callosum on 1.5-mm thick, T2-weighted imaging.
The most common causes of pretectal syndrome are hydrocephalus, tumours and cerebrovascular disorders; however multiple sclerosis is really rare [3] Problems associated with the similar terminologies including Parinaud’s syndrome, sylvian aqueduct syndrome or dorsal midbrain syndrome were discussed. The eponym is attributed to Henri Parinaud, an ophthalmologist who worked under Charcot at the Salpetriere in Paris in the late 19th century and wrote two landmarks articles describing various types of conjugate gaze palsies and paralyses of convergence4. Nowadays, the syndrome includes pupillary and eyelid abnormalities, as well as convergence retraction nystagmus, for this reason the term pretectal syndrome are more popular[4,5]. The supranuclear vertical gaze restriction in this syndrome results from involment of the posterior commisure, intersticial nucleus of Cajal or riMLF. Upgaze deficits may be seen alone as in our case, or in combination wit downgaze paresis, lesions affecting posterior commisure usually produce greater involment of upgaze while those located more ventrally are associated with greater downgaze paresis 5. Fibers mediating the upward gaze originate in the rostral interstitial MLF (riMLF) project ipsilateraly to ipsilateral oculomotor complex, cross through the posterior commissure, and terminate in the contralateral oculomotor complex . On the other hand, fibbers from interstitial nucleus of Cajal cross within the posterior commisure before reaching the oculomotor complex and the superior rectus and inferior oblique subnuclei. However, for downgaze each riFLM supplies the ipsilateral inferior nucleus and the fourth nucleus. This may be a reason for the dissociation of the upward and downward gaze palsy, and the different topography for upward and downward gaze. And MS should be considering in the differential diagnosis in a patient with a pretectal syndrome.
2307
References
- Keane JR. The pretectal syndrome: 206 patients. Neurology 1990; 40(4):684-690.
- Keane JR, Davis RL. Pretectal syndrome with metastatic malignant melanoma to the posterior commissure. Am J Ophthalmol 1976; 82(6):910-914.
- Keane JR. The pretectal syndrome: 206 patients. Neurology 1990; 40(4):684-690.
- Liu GT VNGSL. Neuro-ophthalmology. Liu GT VNGS, editor. 1est, 584- 626. 2004. Philadelphia, WB Saunders company. Ref Type: Serial (Book,Monograph)
- Corbett JJ, Schatz NJ, Shults WT, Behrens M, Berry RG. Slowly alternating skew deviation: description of a pretectal syndrome in three patients. Ann Neurol 1981; 10(6):540-546.

