Keywords
Type 2 diabetes mellitus; Prevalence; Determinants; Preventon; Arabic countries
Introducton
Diabetes in one of the most common public health problem in both developed and developing countries [1,2]. The prevalence of Type 2 Diabetes Mellitus (T2DM) is increasing and alarming causing threat to the populaton around the globe [3]. According to the World Health Organizaton (WHO) the prevalence of diabetes will double by 2030 [4]. There are three types of diabetes. Type 1 is an auto immune disease where pancreases produce litle or no insulin at all. T2DM is a lifestyle disease because it is triggered by obesity, physical inactvity and sedentary lifestyle and type 3 is a conditon specifc to women when they are pregnant and it disappears afer birth [5,6]. It is said that T2DM is the end stages of diabetes where it mostly afects people later in their lives or it can be hereditary to or for some rare cases where it will afect some in their younger years [7,8].
Sedentary lifestyle with low/zero amounts of physical exercise is a huge contributng factor to fat build up in the body [9]. This could be prevented through living a healthy life style. Study shows that most individuals, mainly Arabic people that are newly diagnosed have a high income making them more prone to obesity which is a contributng factor to T2DM [10]. The other research shows that people are provided with self- monitoring blood glucose to detect hypoglycemia. Therefore, there will be litle need for people to take care of their diet since they can just monitor their glucose level [11]. It also talks about the under testng and over testng which could be inconvenient.
It states that some of the strongest predicton of diabetes T2DM is obesity and family history of diabetes [12]. In additon, genetcs does play a role in the occurrence of T2DM but it is the poor lifestyle choices that contribute to the causes of diabetes that actually increases the susceptbility and severity of being diagnosed with T2DM [13]. So a poor/unhealthy diet does not only increase your chance of T2DM but an unhealthy/sedentary lifestyle too would highly likely contribute your chances [14].
To coincide the mentoned causes, the amount of preventons and interventons are very limited as they all target the same issues and that is to readjust patent’s lifestyle, both with a more healthy diet and a proactve physical lifestyle [15]. As, from the interventon studies perspectve, the main focus will lean more into the pharmaceutcal aspects. There are certain medicatons used in preventon studies but the most common, boostng role in preventng at-risk individuals who are at the pre-stages of T2DM to be diagnosed [16]. The artcle also notes that being in these pre- stages could leave one at risk of other health related problems like hypertension and Polycystc ovary syndrome (PCOS) [17].
Moreover, the causes of T2DM occurs right across the globe and, despite the many existng known causes and even underlining problems, there stll is much more to be discovered and further researched on its determinants and preventon. It was found that most of the artcles were specifcally describing how T2DM afects both genders especially those at their later years. Also, majority of the determinants are from poor lifestyle choices to looking afer one’s health and wellbeing.
The main objectve of this systematc review is look into the determinants, prevalence, and preventons of T2DM in Arabic countries. Hence, this systematc review will provide a T2DM scope and trend to the determinants and preventon strategies identfed from the various sourced artcles from 2000 to 2015.
Methodology
This systematc review was conducted based on the Cochrane library guideline and PRISMA criteria [18]. Through the duraton of the systematc review the following databases and search engines were used: Scopus, Google scholar, CINAHIL, Medline, and PubMed. Key-words like “Type 2 Diabetes Mellitus” AND “preventon” AND “prevalence” AND “determinants OR risk factor” AND “Arabic countries OR natons” were used to fnd relevant studies. We limited our search to be within the years 2000 to 2015, only English language papers and focused on Arabic countries. Those artcles that were before and afer the search years were considered as the exclusion criteria. Artcles were published in Arabic language or we could not fnd their full texts were also excluded.
Two independent reviewers coded the artcle separately to reduce the bias. Furthermore, we had three sets of review artcles afer omitng duplicated studies. The frst step was scanning papers’ ttles. Then the search was focused on the abstract of remained studies. The last step was about reviewing the full text of remained studies. When the last search was conducted it brought our fnding specifcally to the artcle we needed.
The number of artcles were found in each stage is shown in Table 1. In the systematc review out of 360 artcles found only 22 artcles were deemed to be relevant to the topic.
Table 1 Frequency of studies were found in different steps.
| DATABASES |
STEP 1 |
STEP 2 |
STEP 3 |
| Scopus |
87 |
12 |
5 |
| Google Scholar |
122 |
22 |
8 |
| PubMed |
56 |
10 |
4 |
| CINAHIL |
45 |
8 |
3 |
| Medline |
50 |
6 |
2 |
| TOTAL |
360 |
58 |
22 |
By reviewing the bibliography of remained paper, 3 new studies were added so that in total 25 were used for this systematc review study. The relevant informaton from the artcles were obtained and included in the data extracton sheet (Annex) for further analysis. A descriptve analysis was used to calculate frequency, percentage of studies for diferent variables.
Results
Overall 25 studies were reviewed in this study. Saudi Arabia with 5 studies had the highest frequency of studies which is followed by UAE (3 studies) and Qatar, Oman, and Kuwait (two studies each) (Figure 1).
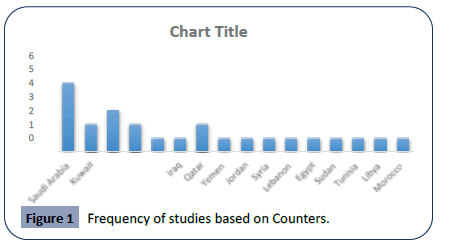
Figure 1: Frequency of studies based on Counters.
Table 2 illustrates that majority of studies were conducted among both male and female (8 studies). Five studies focused only on male and 2 studies were conducted among female only.
Table 2 Frequency of studies based on Gender.
| Gender |
Frequency |
Percentage |
| Men only |
5 |
20 |
| Woman only |
2 |
8 |
| Both Men and Women |
18 |
72 |
Table 3 reveals that 52% of the studies focus in all age group, 12% focus on the age group of below 20, 32% focus on the age group of 20 – 50 and 4% among more than 50 years old.
Table 3 Frequency of studies based on Age.
| Age |
Frequency |
Percentage |
| <20 |
3 |
12 |
| 20-50 |
8 |
32 |
| 50-over |
1 |
4 |
| All age groups |
13 |
52 |
Table 4 gives an illustraton from the studies been carried out, 24% of the studies was carried out in the Year 2000 – 2004; 56% was carried from the year 2005 to 2009 and 20% from 2010 to 2014.
Table 4 Frequency of studies based on the Year of study.
| Year of study |
Frequency |
Percentage |
| 2000-2004 |
6 |
24 |
| 2005-2009 |
14 |
56 |
| 2010-2014 |
5 |
20 |
Table 5 shows the partcipants were well chosen in order to carry out the research. According to the result, 44% of studies focused only on diabetc patents. 36% of the studies carried out focused on non-diabetc patent, 8% focused on high risk populaton. Similarly, 8% of the studies choose obesity people to be their partcipants. 4% of the studies focused on relatve of diabetc patents.
Table 5 Frequency of studies based on Participants.
| Participants |
Frequency |
Percentage |
| Relatives of diabetic patients |
1 |
4 |
| Diabetic patients |
11 |
44 |
| Non diabetic patients |
9 |
36 |
| High risk patients |
2 |
8 |
| Obesity |
2 |
8 |
As Table 6 shows, 28% of the studies used experimental and clinical method, 8% used case control method, another 56% use observatonal/cross sectonal method only, and 8% used prospectve community based method of studies.
Table 6 Frequency of studies based on Type.
| Study Type |
Frequency |
Percentage |
| Case Control |
2 |
8 |
| Clinical Studies |
7 |
28 |
| Observational/ Cross Sectional |
14 |
56 |
| Prospective Community Based |
2 |
8 |
Figure 2 demonstrates the diferent sampling methods. From the 25 studies reviewed, 53% use random sampling method, 41% use purposive and 6% use stratfed method.
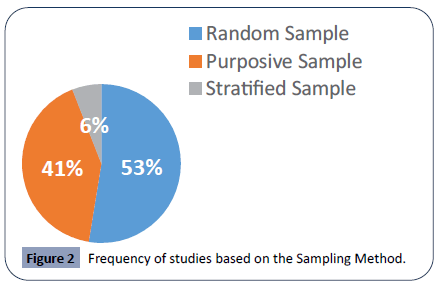
Figure 2: Frequency of studies based on the Sampling Method.
As Table 7 shows, majority of countries had a prevalence of 10- 20%. Qatar (50%) and Bahrain (30%) had the highest prevalence while Sudan had lowest rate (1.4%) which followed by Egypt (3.76%) and Morocco (6.4%).
Table 7 Frequency of studies based of Prevalence.
| Prevalence |
Number of studies |
| <10% |
8 |
| 10-20% |
11 |
| 20-30% |
5 |
| 30> |
1 |
Figure 3 revealed the areas the studies were conducted. From the 25 studies been carried out, 47% focused on determinant and risk factor, 23% focused on determinant with preventon, 24% focus on preventon only and the other 6% focused on the interventon.
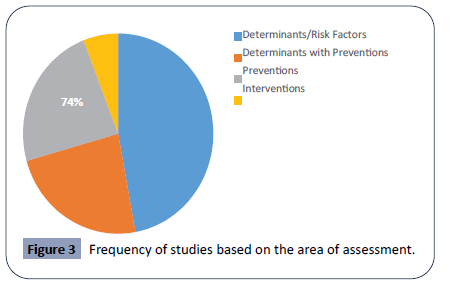
Figure 3: Frequency of studies based on the area of assessment.
Finding the determinants of diabetes was the one of the main aim in this review. The determinants were than classifed as modifable and non-modifable parts. As Figure 4 shows nutriton was the most common modifable determinants (14 studies) which followed by lifestyle and obesity (12 studies each).
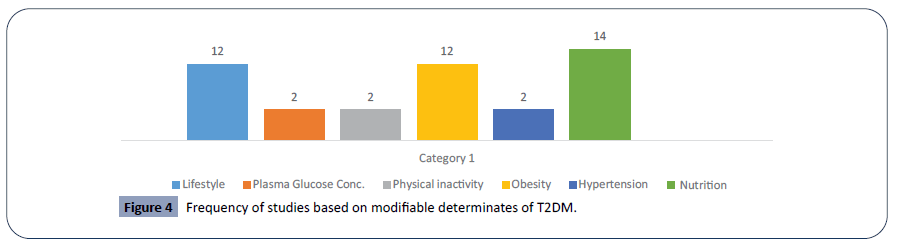
Figure 4: Frequency of studies based on modifable determinates of T2DM.
Figure 5 illustrates the non-modifable determinants which were of those cannot be changed. Age was the highest frequency of 14. The frequency at 12 which was the Race showed diferent cultures and way of life diferent races lived. Gender with 10 showed how the diferent sex respond to diabetes and lastly was 4 with genetc, which shared to of-springs with insulin productvity of various people determined through their genes.
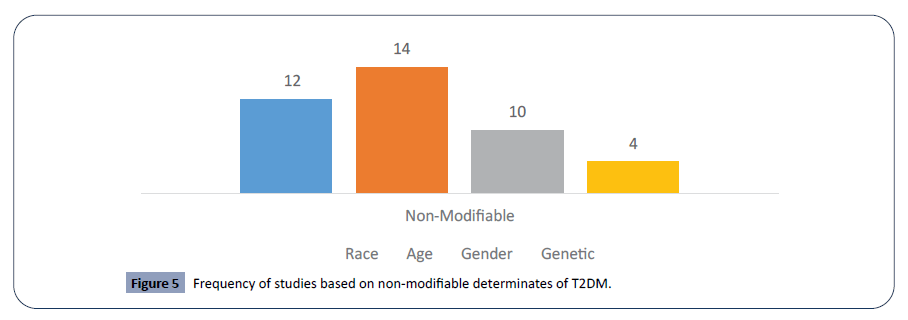
Figure 5: Frequency of studies based on non-modifable determinates of T2DM.
Figure 6 illustrated the preventon strategies were compiled from the diferent studies shown and listed to which of they occurred to be of efectve. Lifestyle interventons were at a frequency of 13. Physical actvites occurred 10, 8 was with frequent visits to health services and this leaves 5 due to the decreasing fat consumpton and intake of drugs occurred only two.
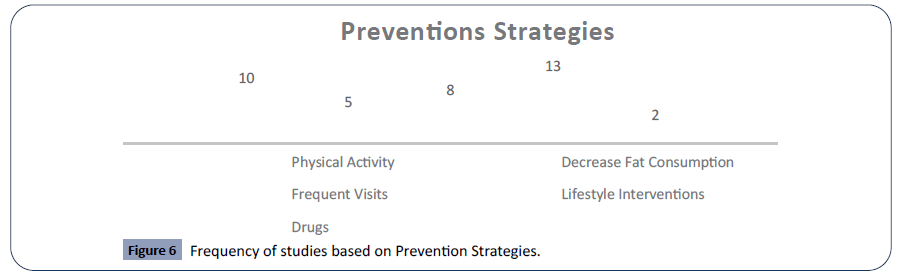
Figure 6: Frequency of studies based on Preventon Strategies.
Discussion
T2DM is a well-known disease afectng many countries nowadays. From the many studies identfed, 25 of the artcles were selected and compiled to determine the main determinant, prevalence and preventon strategies for T2DM in Arabic countries.
As the results of this study showed Saudi Arabia had the highest number of studies conducted on T2DM. It shows more atenton needs to be considered by other countries to T2DM as one of the serious public health issues and do more study about it. The number of studies conducted in Arabic countries shows there could be lacking presence of valuable data about T2DM in many Arabic countries. Moreover, not everybody could excess the health services due to some social determinates faced, and thirdly, most cases would be either unaware of the importance of diabetes self-management behaviors or environmental, and systems barriers to diabetes self-management [19,20].
The results revealed that out of 25 studies, more than half of them were conducted in 2005-2009 while the number is reduced to 20% between 2010 - 2014. This shows, there were a lot of T2DM cases and researchers were working hard to fnd out the main determinants or causes of this disease as well as how to prevent them from happening. Majority of the studies were cross sectonal studies (56%) it shows the need for doing other types of studies and especially interventonal studies to measure eth efectveness of diferent interventon in preventng T2DM. To fnd out the determinants and preventon for T2DM, researches chose their partcipants well. According to the study, 11/25 studies intentonally chose their partcipants to be diabetc patents while the other 9 focused on non-diabetc patent, obesity patents, and the rest among relatves of diabetc patents and high risk patents.
The prevalence of T2DM reported in this study shows, it is a main health issue among Arabic countries. Since then researchers made T2DM as a leading issue when coming to research to fnd an interventon to the reducton in number of diabetes. It is recommended that primary health care initatves such as awareness programs be improved upon as many of the artcles writen emphasized a lack in the efectveness of primary health care which if given the proper atenton can cut of the problem of T2DM from its roots [21,22].
According to the study, it has been found that there the majority of determinants for T2DM were classifed into two types; the modifed and non-modifed determinants.
For the modifed determinants, 14/25 of the studies show that nutriton is the main determinant of T2DM. What we eat defne how we are and for this case more intake of sugar will lead to high glucose level and then insulin resistance in the body which then leads to T2DM. Nutriton itself leads to obesity which is one of the determinants of T2DM. According to the result, 12/25 studies agreed to that obesity and unhealthy lifestyle were the main determinants for T2DM. It is reported by previous research that around 90% of those who are living with T2DM are overweight or obese [21,23]. Hence, these at-risk people have additonal pressure on their body's capacity to consume insulin to control blood sugar levels appropriately, and are in more chance to develop T2DM. Also to note about they have also made themselves susceptble to other medical complicatons [24].
Previous studies showed that lifestyle determinants have the greatest impact with regards to T2DM, followed by social status, environmental and poor policies and legislatons. This shows that non modifable risk factor are major contributng factor to T2DM [25,26].
Coinciding this to the non-modifed determinant, 14/25 studies agreed that age is one of the main determinants of T2DM. The older people have more chance to practce sedentary lifestyle which leads to obesity and T2DM. Gender and genetcs could also defne the health of a person when comes to T2DM. Interestng fnding by several studies showed that women with polycystc ovary syndrome (PCOS) are insulin resistant, so that they are high risk for glucose intolerance [27] that increase the factor of T2DM and would even underline other medical problems.
T2DM varies within diferent age groups; however, it can be similar within males and females [28]. According to the result 18/25 studies focused on both gender because they both have the same risk of getng this disease. There are many studies who agree on the above result. In a study carried out in Iran, female have high prevalence compare to male [29]. The similarity of the results is because women’s spend more tme at home and they are not physically actve like women in Arabic countries [30]. This study shows that all age group are at risk and majority are from the age group of 20-50. The above mentoned age group is at risk due to them being exposed to change in lifestyle and as well as they are within an age group which is also known as working age group [31,32]. By looking at the results the main insight reveals that T2DM is very common among young adults or middle age group mainly living in urban areas. This shows that the lifestyle in the urban areas have been changing rapidly for most due to people relying on fast foods and trapped in work ofces resultng in inactvity. People tend to be careless about their health. Other contributng factors are diet, obesity, inactvity, hypertension, socioeconomic, age, gender etc. To support this idea from the result, a partcular study which has been used in the review above states that obesity and diabetes in Arabic countries among males and females age 15 to 64 years revealed the key infuence of diabetes in the Arabic countries was due to lifestyle, socioeconomic factors and weak legislatons [33]. These factors can be improved with the help of health facilitators and engaging people in advocatng healthy behaviors.
Amongst diferent studies which have been used in this study they state that the fast ratng prevalence is the category of likeliness to prevail afer 10-20 years with the highest percentage. This refects that people whose age falls in this age group are in the actve stage age 18 and above. On the other hand middle age group also have a high percentage with regards to the increasing rate of T2DM. The contributng factor that cause them to be victms are numerous such as child obesity, inappropriate feeding when they are litle like, early introducton of faty and junk foods leading to child overweight and obesity that might cause them to be inactve. This has made them to more susceptble and prone to becoming victms to T2DM [34].
Based on the results of this study the majority of the research artcles contained advice or interventons relevant to the preventon of T2DM. The recommendatons include increased physical actvity, healthier diet and healthier lifestyle choices in preventng type diabetes [35].
Targetng specifc lifestyle to prevent diabetes was of the most. Doing clinical and experimental studies will show causes and efects. Furthermore, complementng this is the discovery of having the highest majority of the studies to be regarding ‘Determinants with Preventon’ and ‘Preventon which then leaves ‘Interventon’ topic of study to be the very least. A cleared logical explanaton for this is because T2DM is a preventable disease compared to its type 1, also there had to be a majority of Clinical and Experimental studies in alignment these topics of study for the sole purpose of trial and error of discovering among test subjects which are the most suitable preventon strategies that would not just be the best alternatve but the most efectve out the other majority [36]. Our research fndings projected preventons ideas where majority really focused on the changing ones unhealthy lifestyle to a more proactve one and minority of the study actually looked at the pharmaceutcal aspects of preventng T2DM using efectve preventatve drugs like metormin, perindopril and indapamide [37,38] but then these drugs had even severe side-efects and require strict a lot of complicated follow-ups to accompany its most efectve use.
Thus studies have shown that a healthy and proactve lifestyle prevents diabetes the most. This was more efectve than those taking drugs, and frequent visits to the health services. Having healthy lifestyle which included the healthy diets, physical actvity and preventng sedentary behaviors [39].
With the completon of this result there are some strengths and limitaton which have been encountered along the way. This study is the frst study reviewed all the determinate, and preventve strategies were used for T2DM along with the prevalence of this issue in Arabic countries. The limitaton was limited number of artcles published about T2DM in Arabic naton as well as difculty to achieve the full text of studies using diferent database to include in this review (Annexure [40-64]).
Conclusion
In conclusion, it is obvious that the prevalence rate of T2DM has been very high amongst young adults and middle aged group, not forgetng the old people with the age of 50 years and above. This may be due to lifestyle, social status, environmental and policies and legislatons. Other factors include diet, inactvity, obesity, hypertension, age and gender. Thus, it is clear that modifable factors are responsible for the increasing rate of T2DM more than non-modifable factors. On the same note, developing countries are more susceptble to T2DM than developed countries. Therefore, to reduce T2DM, it is very important at the regional, natonal, provincial and community level to work together to established polices and ways to addresses the prevalence of diabetes as it is one of the most common NCD in the world today.
In this study it can be said that diabetes is a serious concern as it is increasing rapidly. Some of the identfed risk factors that triggers diabetes are: cardiovascular disease, alcohol intake, and smoking. Similarly, people look at diabetes as inevitable which is a major drawback, thus, afectng them psychologically. However, diabetes is a lifestyle disease and most people are not aware of this, hence, vigorous awareness must be carried out in a way that people fully understand what diabetes is and how it can be prevented.
People have diferent lifestyles due to the conditon they live in and the conditon they have been through. To further elaborate, developing countries have the highest prevalence due to usage and availability of health care and health facilites installed for them. Some are more actve to have a monthly medical checkup while some are very ignorant. Sometmes people think these small things have nothing to do with their health statuses but it does.
26717
References
- Ferrara A (2007) Increasing prevalence of gestational diabetes mellitus: a public health perspective. Diabetes care 30: S141-S146.
- Ludwig DS, Ebbeling CB (2001) Type 2 diabetes mellitus in children: primary care and public health considerations. JAMA 286: 1427-1430.
- Wild S, Roglic G, Green A, Sicree R, King H (2004) Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes care 27: 1047-1053.
- Shaw JE, Sicree RA, Zimmet PZ (2010) Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes research and clinical practice 87: 4-14.
- Zheng Y, Ley SH, Hu FB (2018) Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol 14: 88.
- Mayer-Davis EJ, Lawrence JM, Dabelea D, Divers J, Isom S, et al. (2017) Incidence trends of type 1 and type 2 diabetes among youths, 2002–2012. N Engl J Med 376: 1419-1429.
- Chen L, Magliano DJ, Zimmet PZ (2012) The worldwide epidemiology of type 2 diabetes mellitus-present and future perspectives. Nature Reviews Endocrinology 8: 228.
- Evans JM, Newton RW, Ruta DA, MacDonald TM, Morris AD (2000) Socio‐economic status, obesity and prevalence of Type 1 and Type 2 diabetes mellitus. Diabet Med 17: 478-480.
- Association AD (2005) Role of insulin secretion and sensitivity in the evolution of type 2 diabetes in the diabetes prevention program: effects of lifestyle intervention and metformin. Diabetes 54: 2404-2414.
- Badran M, Laher I (2011) Obesity in Arabic-speaking countries. J Obes 2011: 686430.
- Welschen LM, Bloemendal E, Nijpels G, Dekker JM, Heine RJ, et al., (2005) Self-monitoring of blood glucose in patients with type 2 diabetes who are not using insulin: a systematic review. Diabetes care 28: 1510-1517.
- Freemark M, Bursey D (2001) The effects of metformin on body mass index and glucose tolerance in obese adolescents with fasting hyperinsulinemia and a family history of type 2 diabetes. Pediatrics 107: e55.
- DeFronzo RA (2004) Pathogenesis of type 2 diabetes mellitus. Med Clin North Am 88: 787- 835.
- Mitra A, Dewanjee D, Dey B (2012) Mechanistic studies of lifestyle interventions in type 2 diabetes. World J Diabetes 3: 201-207.
- Diabetes Prevention Program Research Group (2002) Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 346: 393-403.
- Bailey CJ, Gross JL, Pieters A, Bastien A, List JF (2010) Effect of dapagliflozin in patients with type 2 diabetes who have inadequate glycaemic control with metformin: a randomised, double-blind, placebo-controlled trial. Lancet 375: 2223-2233.
- Napolitano A, Miller S, Nicholls AW, Baker D, van Horn S, et al. (2014) Novel gut-based pharmacology of metformin in patients with type 2 diabetes mellitus. PLoS ONE 9: e100778.
- Ramadas A, Quek KF, Chan CKY, Oldenburg B (2011) Web-based interventions for the management of type 2 diabetes mellitus: a systematic review of recent evidence. International journal of medical informatics 80: 389-405.
- Habashneh RA, Khader Y, Hammad MM, Almuradi M (2010) Knowledge and awareness about diabetes and periodontal health among Jordanians. J Diabetes Complications 24: 409-414.
- Schoenfeld ER, Greene JM, Wu SY, Leske MC (2001) Patterns of adherence to diabetes vision care guidelines: baseline findings from the Diabetic Retinopathy Awareness Program. Ophthalmology 108: 563-571.
- Alberti KG, Zimmet P, Shaw J (2007) International Diabetes Federation: a consensus on Type 2 diabetes prevention. Diabet Med 24: 451-463.
- Astrup A, Finer N (2000) Redefining type 2 diabetes:‘diabesity’or ‘obesity dependent diabetes mellitus’? Obes Rev 1: 57-59.
- Vikram N, Tandon N, Misra A, Srivastava MC, Pandey RM, et al. (2006) Correlates of Type 2 diabetes mellitus in children, adolescents and young adults in north India: a multisite collaborative case‐control study. Diabet Med 23: 293- 298.
- Heine RJ, van Gaal LF, Johns D, Mihm MJ, Widel MH, et al. (2005) Exenatide versus insulin glargine in patients with suboptimally controlled type 2 diabetes: a randomized trial. Ann Intern Med 143: 559-569.
- Schram MT, Sep SJ, van der Kallen CJ, Dagnelie PC, Koster A, et al. (2014) The Maastricht Study: an extensive phenotyping study on determinants of type 2 diabetes, its complications and its comorbidities. Eur J Epidemiol 29: 439-451.
- Young TK, Reading J, Elias B, O'Neil JD (2000) Type 2 diabetes mellitus in Canada ‚s First Nations: Status of an epidemic in progress. CMAJ 163: 561-566.
- Legro RS (2006) Type 2 diabetes and polycystic ovary syndrome. Fertility and sterility 86: S16-S17.
- Hasslacher CH, Ritz E, Wahl P, Michael C(1989) Similar risks of nephropathy in patients with type I or type II diabetes mellitus. Nephrology Dialysis Transplantation 4: 859-863.
- Azimi-Nezhad M, Ghayour-Mobarhan M, Parizadeh MR, Safarian M, Esmaeili H, et al. (2008) Prevalence of type 2 diabetes mellitus in Iran and its relationship with gender, urbanisation, education, marital status and occupation. Singapore Med J 49: 571-576.
- Ali HI, Baynouna LM, Bernsen RM (2010) Barriers and facilitators of weight management: perspectives of Arab women at risk for type 2 diabetes. Health Soc Care Community 18: 219-228.
- Mohan V, Sandeep S, Deepa R, Shah B, Varghese C (2007) Epidemiology of type 2 diabetes: Indian scenario. Indian J Med Res 125: 217-230.
- Brown LC, Majumdar SR, Newman SC, Johnson JA (2005) History of depression increases risk of type 2 diabetes in younger adults. Diabetes Care 28: 1063-1067.
- Hill J, Nielsen M, Fox MH (2013) Understanding the social factors that contribute to diabetes: a means to informing health care and social policies for the chronically ill. Perm J 17: 67.
- Haire-Joshu D, Nanney MS (2002) Prevention of overweight and obesity in children: influences on the food environment. Diabetes Educ 28: 415-423.
- Astrup A (2001) Healthy lifestyles in Europe: prevention of obesity and type II diabetes by diet and physical activity. Public Health Nutr 4: 499-515.
- Satterfield DW, Volansky M, Caspersen CJ, Engelgau MM, Bowman BA, et al. (2003) Community-based lifestyle interventions to prevent type 2 diabetes. Diabetes care 26: 2643-2652.
- Asif M (2014) The prevention and control the type-2 diabetes by changing lifestyle and dietary pattern. J Educ Health Promot 3: 1.
- Kushi LH, Doyle C, McCullough M, Rock CL, Demark-Wahnefried W, et al. (2006) American Cancer Society Guidelines on Nutrition and Physical Activity for cancer prevention: reducing the risk of cancer with healthy food choices and physical activity. CA Cancer J Clin 56: 254-281.
- Moreno L, González-Gross M, Kersting M, Molnár D, de Henauw S, et al. (2008) Assessing, understanding and modifying nutritional status, eating habits and physical activity in European adolescents: the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study. Public Health Nutr 11: 288-299.
- Al-Nozha MM, Al-Maatouq MA, Al-Mazrou YY, Al-Harthi SS, Arafah MR, et al. (2004) Diabetes mellitus in saudi arabia. Saudi Med J 25: 1603-1610.
- Almajwal AM, Al-Baghli NA, Batterham MJ, Williams PG, Al-Turki KA, et al. (2009) Performance of body mass index in predicting diabetes and hypertension in the Eastern Province of Saudi Arabia. Ann Saudi Med 29: 437-445.
- Al‐Rubeaan K, Al-Manaa HA, Khoja TA, Ahmad NA, Al-Sharqawi AH, et al. (2015) Epidemiology of abnormal glucose metabolism in a country facing its epidemic: SAUDI‐DM study. J Diabetes 7: 622-632.
- Al-Rubeaan K, Al-Manaa H, Khoja T, Ahmad N, Al-Sharqawi A, et al. (2014) The Saudi abnormal glucose metabolism and diabetes impact study (SAUDI- DM). Ann Saudi Med 34: 465-475.
- Mansour AA, Al-Jazairi MI (2007) Predictors of incident diabetes mellitus in Basrah, Iraq. Ann Nutr Metab 51: 277-280.
- Musaiger AO, Shahbeek NE (2005) The relationship between obesity and prevalence of chronic diseases in the Arab women. J Hum Ecol Special 13: 97-100.
- Al-Habori M, Al-Mamari M, Al-Meeri A (2004) Type II Diabetes Mellitus and impaired glucose tolerance in Yemen: prevalence, associated metabolic changes and risk factors. Diabetes Res Clin Pract 65: 275-281.
- Ajlouni K, Khader YS, Batieha A, Ajlouni H, El-Khateeb M (2008) An increase in prevalence of diabetes mellitus in Jordan over 10 years. Journal of Diabetes and its Complications 22: 317-324.
- Albache N, Ali RA, Rastam S, Fouad FM, Mzayek F, et al. (2010) Epidemiology of Type 2 diabetes mellitus in Aleppo, Syria. J Diabetes 2: 85-91.
- Hirbli KI, Jambeine MA, Slim HB, Barakat WM, Habis RJ, et al. (2005) Prevalence of diabetes in greater Beirut. Diabetes Care 28: 1262.
- Abolfotouh MA, Soliman LA, Mansour E, Farghaly M, El-Dawaiaty AA(2008) Central obesity among adults in Egypt: prevalence and associated morbidity. East Mediterr Health J 14: 57-68.
- Noor SKM, Bushara SOE, Sulaiman AA, Elmadhoun WMY, Ahmed MH(2015) Undiagnosed diabetes mellitus in rural communities in Sudan: prevalence and risk factors. Eastern Mediterranean Health Journal 21.
- Bouguerra R, Alberti H, Salem LB, Rayana CB, Atti JE, et al. (2007) The global diabetes pandemic: the Tunisian experience. Eur J Clin Nutr 61: 160-165.
- Kadiki OA, Roaeid RR (2001) Prevalence of diabetes mellitus and impaired glucose tolerance in Benghazi Libya. Diabetes Metab 27: 647-654.
- Rguibi M, Belahsen R (2006) Prevalence and associated risk factors of undiagnosed diabetes among adult Moroccan Sahraoui women. Public Health Nutrition 9: 722-727.
- Moussa MA, Alsaeid M, Abdella N, Refai TMK, Al-Sheikh N, et al. (2008) Prevalence of type 2 diabetes mellitus among Kuwaiti children and adolescents. Med Princ Pract 17: 270-275.
- Al-Mahroos F, Al-Roomi K (2001) Obesity among adult Bahraini population: impact of physical activity and educational level. Ann Saudi Med 21: 183-187.
- Al‐Lawati J, Riyami AMA, Mohammed AJ, Jousilahti P (2002) Increasing prevalence of diabetes mellitus in Oman. Diabetic medicine 19: 954-957.
- Baynouna LM, Revel AD, Nagelkerke NJ, Jaber TM, Omar AO, et al.(2008) High prevalence of the cardiovascular risk factors in Al-Ain, United Arab Emirates. Saudi Med J 29: 1173-1178.
- Saadi H, Carruthers SG, Nagelkerke N, Al-Maskari F, Afandi B, et al., Prevalence of diabetes mellitus and its complications in a population-based sample in Al Ain, United Arab Emirates. Diabetes Res Clin Pract 78: 369-377.
- Al-Moosa S, Allin S, Jemiai N, Al-Lawati J, Mossialos E (2006) Diabetes and urbanization in the Omani population: an analysis of national survey data. Population Health Metrics 4: 5.
- Bener A, Zirie M, Janahi IM, Al-Hamaq AO, Musallam M, et al. (2009) Prevalence of diagnosed and undiagnosed diabetes mellitus and its risk factors in a population-based study of Qatar. Diabetes Res Clin Pract 84: 99-106.
- Al-Daghri NM, Al-Attas OS, Alokail MS, Alkharfy KM, Yousef M, et al. (2011) Diabetes mellitus type 2 and other chronic non-communicable diseases in the central region, Saudi Arabia (Riyadh cohort 2): a decade of an epidemic. BMC Med 9: 76.
- Malik M, Bakir A, Saab BA, King H (2005) Glucose intolerance and associated factors in the multi-ethnic population of the United Arab Emirates: results of a national survey. Diabetes Res Clin Pract 69: 188-195.
- Al‐Asi T (2003) Overweight and obesity among Kuwait Oil Company employees: a cross‐sectional study. Occupational Medicine 53: 431-435.

